
Abstract
Background:
Pistol grip deformity of the proximal femur has been reported as a potential cause of hip pain and early-onset arthritis. The exact incidence of patients with osteoarthritis resulting from femoral acetabular impingement (FAI) is unknown. The purpose of this study was to explore the relationship between radiographic markers of FAI in patients undergoing hip arthroplasty.
Methods:
We retrospectively reviewed the radiographs of patients undergoing hip arthroplasty by a single surgeon over a 2-year period. The patients were divided by age, those younger than 65 years and (group A) and those 65 years and older (group B). The radiographs were evaluated for morphology consistent with FAI including an α angle >55°, crossover sign, coxa profunda, acetabular protrusio, and ischial spine sign. Three independent reviewers evaluated all the radiographs. The incidence of CAM, Pincer, and mixed deformities were compared between the 2 groups.
Results:
A total of 255 patients with 258 hip arthroplasties were included in this analysis. Group A was found to have a greater number of patients with CAM morphology. Linear regression analysis revealed that the α angle was greater in younger patients.
Conclusion:
Patients undergoing hip arthroplasty exhibit a high incidence of radiographic abnormalities consistent with FAI. The CAM-type morphology occurs more frequently in younger patients with advanced arthritis requiring hip arthroplasty. This morphology is thought to cause a delaminating injury to the cartilage of the acetabulum. This study supports the notion that CAM-type morphology is a risk factor for early development of degenerative arthritis of the hip.
Introduction
Reports of a potential link between a pistol grip deformity of the proximal femur and progressive early-onset arthritis have appeared in the orthopedic literature since the 1960s. 1 More recently, the concept of femoral acetabular impingement (FAI) has emerged as a mechanical cause of hip pain. Abnormal morphology of the proximal femur or the acetabulum is thought to lead to an anatomic conflict between the proximal femur and the acetabulum, resulting in chondrolabral injury. This pathoanatomic process is thought to be a major cause of idiopathic osteoarthritis of the hip, especially in young patients. 2,3
Femoral acetabular impingement is grouped into 3 basic forms, CAM-type impingement, Pincer-type impingement, and mixed deformities, which are most common and occur approximately 85% of the time. 4,5 The CAM-type impingement is characterized by an aspherical femoral head that causes an obligatory decrease in the femoral head neck offset. 3,4 Flexion and torsional motions at the hip are believed to cause a characteristic pattern of acetabular delamination and injury to the chondrolabral transitional zone at the acetabular rim. The severe chondral injury is thought to result from this and is most often seen in young males. 3,5 Pincer-type impingement is related to abnormal morphology of the acetabulum, characterized by a relative overcoverage of the femoral head. This may be the result of coxa profunda, acetabular protrusio, or excessive retroversion of the acetabulum. 3,4 Overcoverage of the femoral head results in impingement between the acetabular rim and the femoral neck, levering the femoral head into the posterior acetabular fossa causing a “contra-coup” chondral injury. Significant labral maceration and subsequent ossification is also observed from the impingement of the acetabular rim and femoral neck. 3,4 Middle-aged females who engage in athletics are most commonly found to exhibit this type of impingement.
Morphologic characteristics of FAI can be recognized on plain x-rays of the hip. The CAM-type impingement is usually characterized by abnormal femoral head neck offset or an increase in the α angle. 5 –7 A normal α angle has been defined as <55°. 5 –8 Pincer-type impingement is recognized with a crossover sign on an anterior–posterior (AP) pelvis radiograph, indicating a retroverted acetabulum. 6 Coxa profunda can also cause Pincer-type impingement and is recognized when the acetabular teardrop is medial to the ilioischial line. 6 Other radiographic parameters of Pincer-type impingement include the ischial spine sign and acetabular protrusion. 7,9
Although FAI morphology has been identified as a potential cause of early-onset osteoarthritis of the hip with distinct morphologic characteristics, the exact incidence of patients with osteoarthritis resulting from FAI is unknown. Abnormal morphology typical of FAI can be seen in asymptomatic patients with a reported rate of 14% CAM morphology on magnetic resonance imaging. 2 A separate study found 39% of asymptomatic hips to have at least one morphologic characteristic of either CAM or Pincer impingement when evaluated with a computed tomography scan. 10 Identifying the pattern of degenerative arthritis associated with FAI is important as surgical correction of the anatomic abnormality offers a potential intervention to prevent this sequela. The hypothesis of this study was that there would be morphological difference in the proximal femoral and acetabular morphology in patients below the age of 65 (group A) compared to patients aged 65 and older (group B) who were undergoing total hip arthroplasty (THA) or hip resurfacing arthroplasty in a single surgeon practice.
Methods
After institutional review board approval was obtained, we queried our billing database for patients treated by a single surgeon (CD) for degenerative disease of the hip with hip resurfacing or THA between September 1, 2009 and August 31, 2011. The medical records and preoperative radiographs of each patient were reviewed. Inclusion criteria included patients aged 18 or older with degenerative arthritis of the hip undergoing hip arthroplasty. Exclusion criteria included radiographic signs of acetabular dysplasia indicated by a center edge angle of <24°, Perthes disease, a history of slipped capital femoral epiphysis, rheumatoid or systemic inflammatory arthritides, posttraumatic arthritis, revision hip surgery, or patients without radiographs adequate for assessing FAI morphology.
Three independent reviewers (RW, WM, and RL) evaluated the radiographs of each patient. Each reviewer recorded the α angle as measured on the preoperative cross-table lateral radiograph and the acetabular index, center edge angle, and presence of coxa profunda, acetabular protrusion, crossover sign, ischial spine sign, and joint space narrowing on the preoperative AP pelvis radiograph. Acetabular dysplasia was defined as a center edge angle of <24°. These patients were excluded. A CAM deformity was defined as an α angle ≥55° (Figure 1). This was measured on the lateral radiograph as the angle between a line drawn down the center of the femoral neck and a line drawn from the center of the femoral head to the portion of the femoral head that was no longer round. Pincer impingement was defined as the presence of a crossover sign, coxa profunda, acetablular protrusio, or an ischial spine sign.

A, Cross-table lateral x-ray of a 47-year-old female undergoing hip arthroplasty with an increase α angle of 72° characteristic of CAM-type femoral acetabular impingement. B, Cross-table lateral x-ray of a 73-year-old male undergoing hip arthroplasty with a normal α angle and characteristic central wear of the femoral head on the acetabulum.
Statistical analysis was first performed on the data from each reviewer separately using SAS 9.2 and then considered for interreviewer reliability using intraclass correlation (ICC) and κ statistic. The patients were broken into 2 groups, group A consisted of patients aged <65 and group B as those aged ≥65. The total number of radiographic abnormalities for each patient was calculated as the summation of the CAM, coxa profunda, acetabular protrusion, ischial spine sign, and crossover sign. We investigated the effect of age <65 and procedure performed, THA or resurfacing arthroplasty, on the probability of having any radiographic abnormality consistent with FAI, the presence of 3 or more abnormalities compared to 2 or fewer abnormalities, CAM morphology, and Pincer morphology. When evaluating the groups for any radiographic abnormality and the presence of a CAM or a Pincer deformity, the chi-square test was used. When evaluating the groups for the presence of 3 or more abnormalities compared to 2 or fewer abnormalities, the Fisher exact test was used. For each value that was statistically significant, an odds ratio was calculated. A logistical regression analysis was then performed with age as a continuous variable to test the probability of having a CAM deformity.
Results
The database query identified 361 hip arthroplasties performed between September 1, 2009 and August 31, 2011. Of these, 103 were excluded for radiographic signs of dysplasia, avascular necrosis, rheumatoid or other inflammatory arthritis, previous trauma, history of slipped capital femoral epiphysis, Perthes disease, or prior hip surgery. This left 255 patients with 258 hips. The number of patients in each group with average age can be seen in Table 1. In all, 193 hips were in the under the age of 65 group, 154 of which underwent hip resurfacing arthroplasties. In all, 65 patients were in the group of age 65 or older. All patients had preoperative radiographs available for review. The AP pelvis radiograph was determined to be inadequate if the coccyx was not centered over and 1 cm cephalad to the pubic symphisis. This was determined to be inadequate in 64 patients by reviewer 1 and in 59 patients by both reviewers 2 and 3. These patients were excluded from the analysis for those reviewers in regard to the presence of any abnormality, presence of 3 or more abnormalities, and presence of Pincer impingement, thus reviewer 1 evaluated 194 patients and reviewers 2 and 3 evaluated 199 patients. Reviewer 3 determined the lateral radiographs of 2 patients were of too poor quality to adequately measure the α angle, and thus 256 hips were included in the analysis of CAM deformity for reviewer 3. All 258 hips were included in the CAM analysis for reviewers 1 and 2.
Demographic Data of Group A and B.
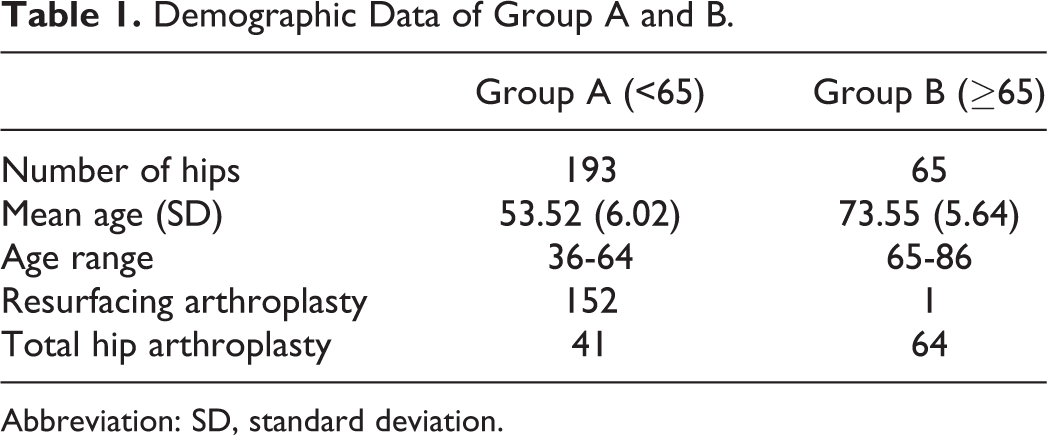
Abbreviation: SD, standard deviation.
Each reviewer evaluated the radiographs for CAM deformity, coxa profunda, acetabular protrusion, crossover sign, and ischial spine sign. The percentages of patients below the age of 65, age 65 or older, who underwent hip resurfacing, and who underwent THA were calculated (Table 2). When evaluating the effect of age, 2 of the 3 reviewers found o be a statistically significant greater number of patients in group A to have at least 1 radiographic abnormality consistent with a diagnosis of FAI and statistically significantly more likely to display CAM morphology (Table 3). No difference was seen when evaluating for the presence of 3 or more radiographic abnormalities or the presence of Pincer morphology. When the logistical regression analysis was performed with age as a continuous variable, all 3 reviewers found that the α angle was greater in younger patients (Figure 2). When evaluated for joint space narrowing, reviewer 1 found 255 of the 258, reviewer 2 found all 258 hips, and reviewer 3 found 257 or the 258 hips to have joint space narrowing to <2 mm on at least 1 view.
Percentage of Patients With Abnormal Morphology Consistent With FAI.
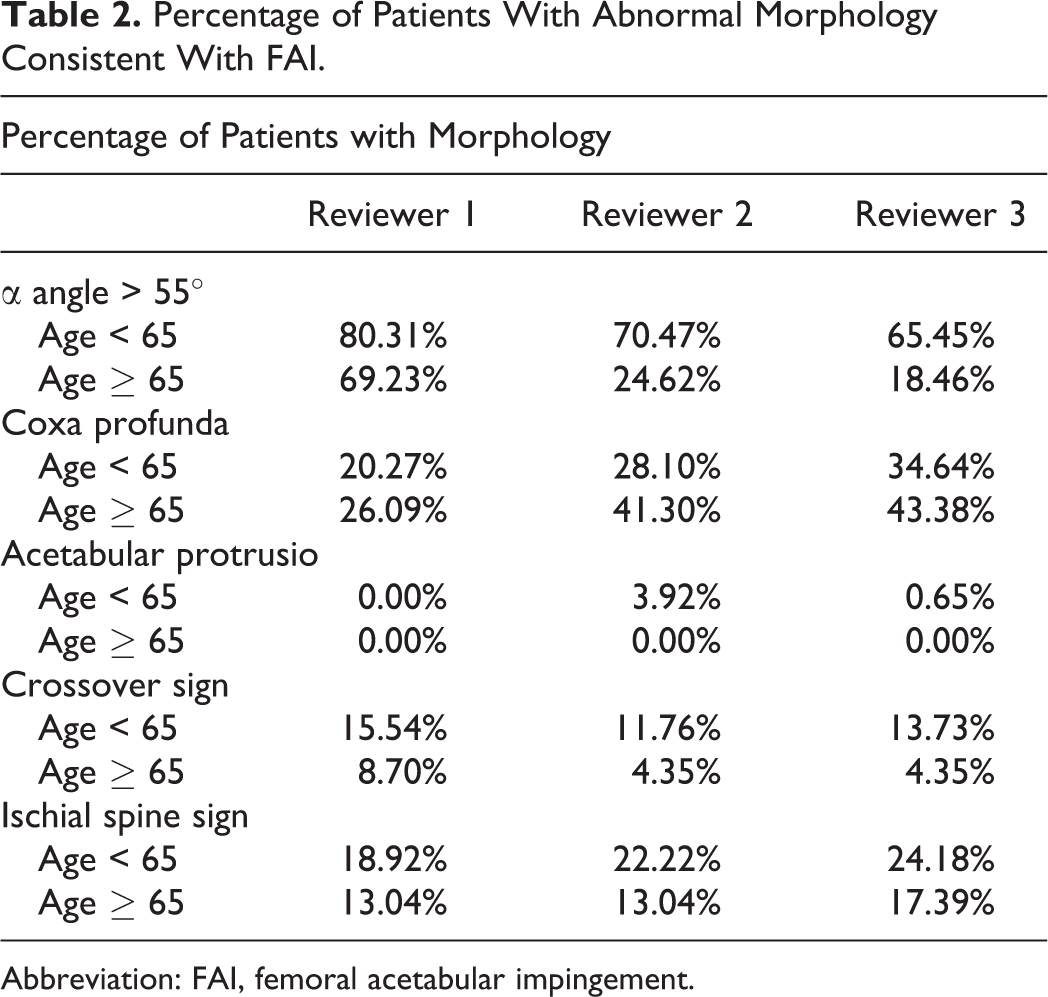
Abbreviation: FAI, femoral acetabular impingement.
P Value of Having at Least 1 Abnormality, 3 or More Abnormalities, CAM Morphology, or Pincer Morphology for Patients Below the Age of 65.


Linear regression analysis shows that younger patients are more likely to display CAM morphology with an elevated α angle than older patients.
When evaluating the procedure performed, all 3 reviewers found there to be a statistically significant greater number of patients undergoing resurfacing arthroplasty to have at least 1 radiographic abnormality consistent with a diagnosis of FAI and statistically significantly more likely to display CAM morphology. No difference was seen when evaluating for the presence of 3 or more abnormalities or the presence of Pincer morphology.
The ICC for the α angle and the κ statistic for the coxa profunda, ischial spine sign, and crossover sign were calculated using SAS 9.2. Acetabular protrusio was excluded from the κ statistic because of the low prevalence reported by each reviewer. The consistency between reviewers 2 and 3 was high while the consistency of reviewer 1 was inconsistent with both reviewers 2 and 3 (Table 4).
Results for Estimates for the ICC of α Angle and the κ Statistics for Coxa Profunda, Ischial Spine Sign, and the Crossover Sign, Along With Their Corresponding 95% Confidence Intervals.

Abbreviations: CI, confidence interval; ICC, intraclass correlation.
Discussion
The results of this study support the hypothesis that there are differences in the morphology of the proximal femur in patients younger than the age of 65 undergoing arthroplasty of the hip compared to patients older than the age of 65. However, the hypothesis that there would be differences in the acetabular morphology is rejected. Previous authors have shown a high rate of radiographic features consistent with FAI in young patients undergoing hip arthroplasty and in patients with degenerative arthritis compared to patients without degenerative disease. 11,12 However, these authors did not compare young patients with degenerative disease to an older group of patients undergoing hip arthroplasty as we have in the current study. Although our definition of young patients was the age of 65, which was an arbitrary divide, we did show with linear regression analysis that younger patients were more likely to have CAM deformity. We believe our results would have been the same had we divided our 2 groups using a younger age such as 55.
Understanding that younger patients requiring hip arthroplasty for degenerative disease are more likely to display CAM morphology is important in understanding the effects of CAM impingement on articular cartilage. We believe that the CAM deformity plays a significant role in pathophysiology of the chondral injury and subsequent development of painful degenerative hip disease. The CAM morphology has been shown to be associated with 2.2 times greater risk in developing hip arthritis compared to patients without CAM deformity in cross-sectional population studies. 13 There are likely other factors that are involved in the pathogenesis of the degenerative changes frequently observed in these patients. Further studies are necessary to elucidate these biologic factors involved in the pathogenesis of early-onset degenerative arthritis.
Identifying abnormal anatomy as a contributing factor to symptomatic hip disease is important as FAI can be successfully addressed using arthroscopic techniques. Philippon et al has shown that failure to correct this abnormal morphology at the time of arthroscopy is a significant technical cause of surgical failure 14 and has demonstrated improvements in the Harris Hip Score from 58 preoperatively to 84 postoperatively after arthroscopic intervention for FAI with associated chondrolabral dysfunction. 6 Further understanding the contribution of CAM lesions to hip pain and impingement syndrome is important as treatments continue to evolve.
We have shown a high rate of CAM deformity of the proximal femur in patients requiring hip arthroplasty for degenerative arthritis. Our results also show that patients who develop symptomatic degenerative arthritis at a younger age are more likely to have a CAM-type deformity than older patients. These results are consistent with the current understanding of the pathophysiology of CAM-type deformity and resulting chondrolabral separation and subsequent delamination of the articular cartilage in the weight-bearing surface. 4,15 The incidence of Pincer-type impingement did not vary between patients of different ages requiring hip arthroplasty. Although Pincer impingement may cause significant damage to the labrum, the cartilage damage is located circumferentially and may involve only a small strip. 4 Isolated Pincer impingement leaves the cartilage in the weight-bearing area of the acetabulum relatively intact. The chondral damage caused by Pincer impingement may not be severe enough to warrant hip arthroplasty at a younger age.
The major limitation of our study is the inability to conclude a causal relationship between abnormal morphology and degenerative arthritis. This can only be accomplished with prospective study design following a large group of patients over a prolonged period of time. This is practically difficult to carry out. We have only retrospective studies to gain information relationship between FAI and degenerative arthritis. One could speculate that femoral deformity may be linked to the development of degenerative hip disease. Johnston et al has observed a correlation between higher α angles and the severity of the chondral injury seen at the time of arthroscopy. 16 Although it is possible that this deformity is part of a reactive response to abnormal forces seen as part of the degenerative process, it would not explain the different rates of CAM morphology observed in younger and older patients with degenerative arthritis. Our results are important to show that younger patients with degenerative arthritis are more likely to display radiographic characteristics of CAM-type FAI, helping to further understand the relationship between FAI and degenerative arthritis. The lack of correlation of reviewer 1 with the other 2 reviewers is also a limitation. We feel this is due to the inexperience of reviewer 1 in closely evaluating radiographs for FAI characteristics and highlights the importance of detailed evaluation of preoperative radiographs for those treating FAI.
The current study is a radiographic study and lacks functional outcomes. Further work is needed to compare the outcomes of hip arthroplasty in patients with and without FAI morphology. The radiographs used in this study to determine FAI morphology were taken when significant degenerative changes were present. This makes it difficult to interpret radiographic abnormalities such as the crossover sign due to the amount of sclerosis present. Another limitation of our study is that it evaluated patients who had already developed end-stage arthrosis requiring hip arthroplasty. It may be beneficial to study patients with earlier stages of arthritis and evaluate their morphology for signs of FAI. This is a difficult group of patients to capture, and obtaining radiographs on a large number of patients with minor symptoms may be difficult.
The strengths of the study include 3 independent reviewers evaluating every radiograph. All patients were also selected for surgery by a single surgeon, making the criteria for surgery consistent between patients.
Conclusion
In summary, there is a significantly higher rate of CAM-type morphology observed in patients younger than age 65 with advanced arthritic disease requiring hip arthroplasty compared to older patients. This abnormal morphology resulting in an anatomic conflict between the acetabulum and the proximal femur may play a significant role in cartilage injury and early-onset arthritis of the hip.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Michael Maloney and Brian Giordano are Paid Consultant for “Mitek.” Financial payments for lectures and educational programs from “Arthrex.” No other financial payments or benefits from any other commercial entity related to the subject of this article.
Funding
The project described in this publication was supported by the University of Rochester CTSA award number TL1 RR024135 from the National Center for Research Resources and the National Center for Advancing Translational Sciences of the National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.