
Abstract
Aortic atresia with interrupted aortic arch is a rare and critical congenital cardiac anomaly. We report a unique case of Type B interruption with aortic atresia, in which cerebral and coronary perfusion were solely dependent on the left vertebral artery without alternative circulatory pathways within the thoracic cavity. The patient underwent successful single-stage biventricular repair and continues to demonstrate favorable neurodevelopmental progress.
Introduction
Interrupted aortic arch (IAA) with aortic atresia (AA) is an exceptionally rare and typically fatal congenital heart defect. Of the 3 types of IAA, only Type C is considered compatible with life when AA is also present. Type B is not survivable without additional circulatory support in the setting of AA, as it relies solely on the left vertebral artery for blood supply to both the brain and the coronary arteries. 1 We present a rare case of AA with Type B IAA, combined with a large ventricular septal defect (VSD) and complex cerebral vascular anatomy characterized by hypoplastic right anterior and right middle cerebral arteries, along with diffusely hypoplastic internal carotid arteries. In this patient, the anterior cerebral and coronary circulations were dependent on the Circle of Willis (CoW), which was supplied solely by the left vertebral artery. This complex vascular and cardiac anatomy posed clinical and surgical challenges. To the authors’ knowledge, this cardiovascular anatomy has not been previously described in the literature.
Case Presentation
Informed consent was obtained from the patient's mother for the case report. A full-term infant was delivered via Cesarean section due to fetal distress, with a prenatal diagnosis of AA, large VSD, and 2 normally sized ventricles. Birth weight was 3320 gms. The baby required intubation at birth due to perinatal depression and was started on prostaglandin (PGE1) for ductal-dependent systemic circulation. Postnatal echocardiogram confirmed the prenatal diagnosis of AA. In addition, the study demonstrated IAA Type B, moderate-sized secundum atrial septal defect, a large conoventricular VSD, normal biventricular size and systolic function, severely hypoplastic ascending aorta, and a large patent ductus arteriosus (PDA) with retrograde flow into the brachiocephalic and left carotid arteries supplying the coronaries. Cardiac computed tomography (CT) revealed that cerebral perfusion was solely via the left vertebral artery, with retrograde flow in the right vertebral artery into the right subclavian and the brachiocephalic trunk. In addition, there was retrograde flow in both hypoplastic internal carotid arteries fed through the CoW. As a result of this complex anatomy, the entire cerebral circulation was dependent on the flow through the left vertebral artery. Figures 1 and 2 show the complex vascular anatomy and flow pattern as confirmed by cardiac and head and neck CT and subsequent magnetic resonance imaging angiography.
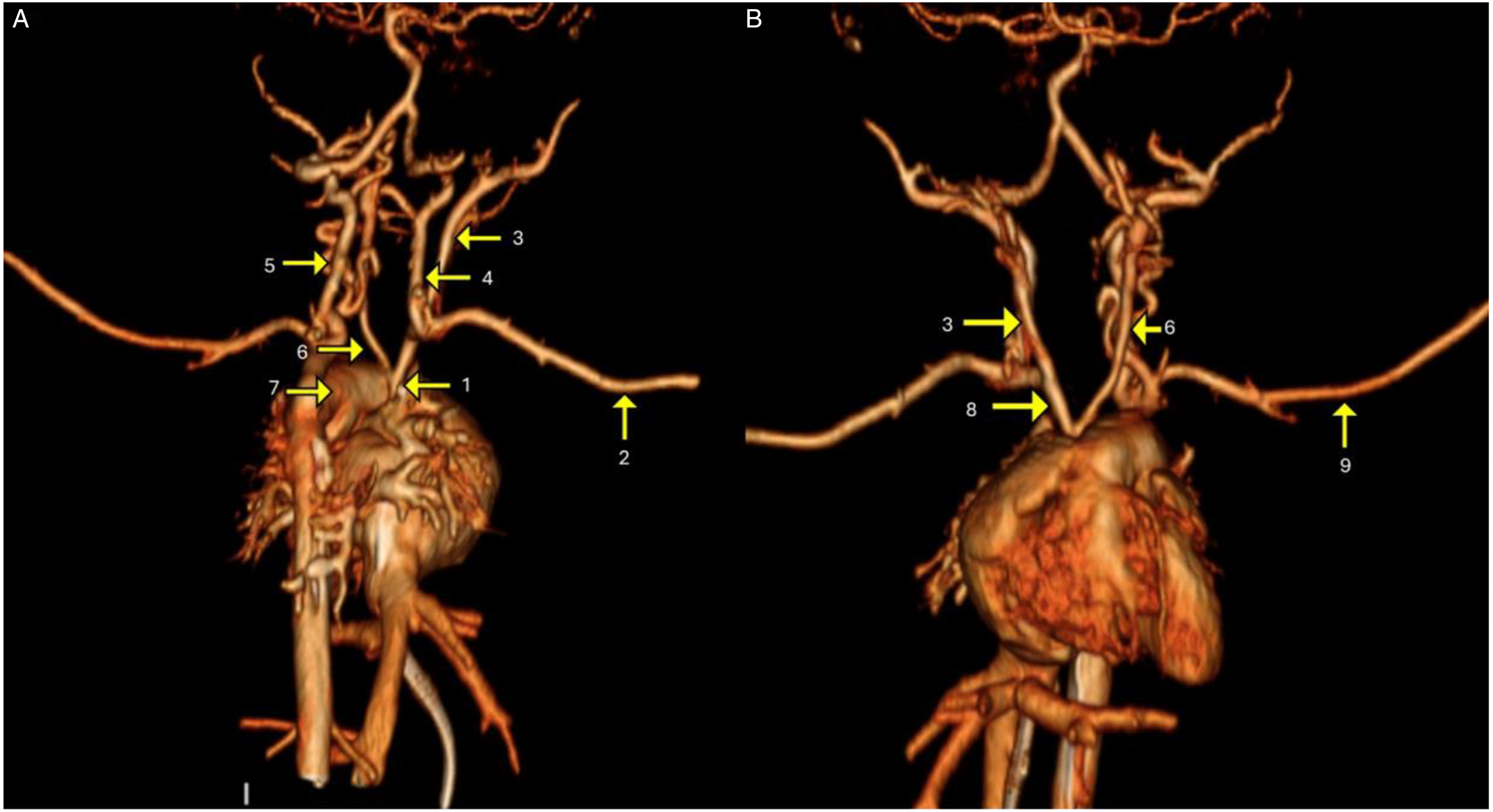
Three-dimensional reconstruction from a contrast-enhanced cardiac CT showing the anatomy of aortic atresia with interrupted aortic arch Type B and branches. (A) CT angiogram, posterior view. (B) CT angiogram, anterior view. 1. Ascending aorta. 2. Right subclavian artery. 3. Right common carotid artery. 4. Right vertebral artery. 5. Left vertebral artery. 6. Left common carotid artery. 7. PDA. 8. Brachiocephalic trunk. 9. Left subclavian artery.
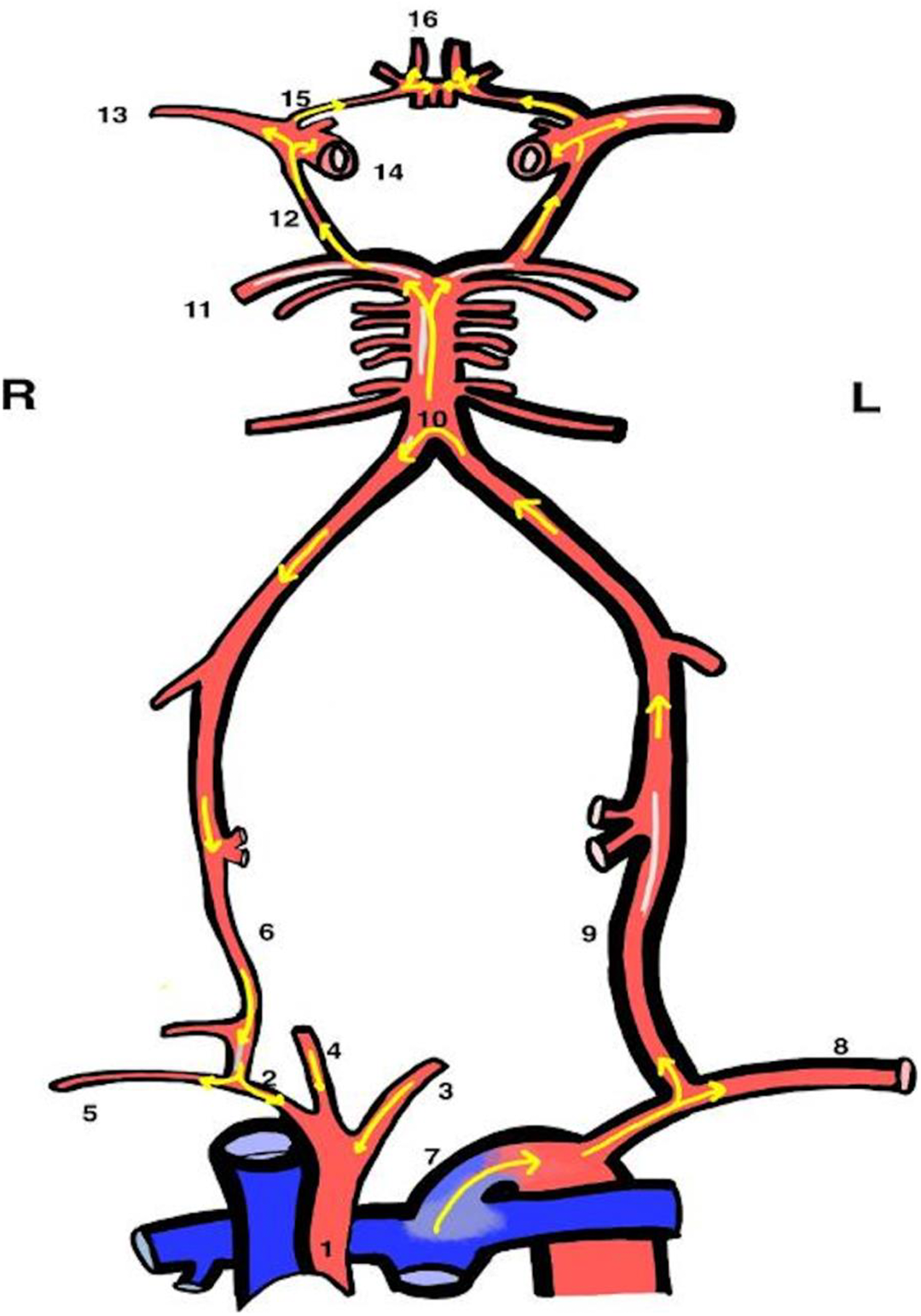
Illustration of CoW-dependent retrograde blood flow to the coronary arteries. This diagram depicts the intricate pathway of blood flow from the PDA to the descending aorta, and subsequently to the left subclavian artery, left vertebral artery, and, in a retrograde manner, to the right vertebral artery, right subclavian artery, and AA. Also, blood flows antegrade from the left vertebral artery to the posterior cerebral artery via the basilar artery, supplying the middle and anterior cerebral arteries. Concurrently, retrograde flow occurs through the bilateral internal carotid arteries, ultimately reaching the ascending aorta and coronary arteries, demonstrating a complex hemodynamic pathway. 1. Ascending aorta. 2. Brachiocephalic trunk. 3. Left common carotid artery. 4. Right common carotid artery. 5. Right subclavian artery. 6. Right vertebral artery. 7. PDA. 8. Left subclavian artery. 9. Left vertebral artery. 10. Basilar artery. 11. Posterior cerebral artery. 12. Posterior communicating artery. 13. Middle cerebral artery. 14. Internal carotid artery. 15. Anterior communicating artery. 16. Anterior cerebral artery.
The patient was also diagnosed postnatally with DiGeorge syndrome on whole exome sequencing. Given the complexity of this case, the patient was transferred at 2 months of age to Boston Children's Hospital, via airlift while intubated, sedated, and maintained on a continuous PGE1 infusion. Complete biventricular repair (Yasui procedure) was performed, including: Damus–Kaye–Stansel anastomosis with aortic arch reconstruction, left ventricle-to-neo-aorta baffle, 12 mm GORE-TEX® right ventricle (RV)-to-pulmonary artery (PA) conduit, PDA ligation, and patent foramen ovale closure. Arterial cannulation for the open-heart surgery involved a 6 French cannula in the left vertebral artery and a 3.5 French cannula inserted retrogradely into the aortic arch to facilitate ascending aortic perfusion and a single venous cannulation in the right atrium. Cardiopulmonary bypass, cross-clamp, and regional perfusion times were 403, 203, and 128 min, respectively. There was deep hypothermia to 28°C. Postoperative recovery was uneventful. The patient was transferred back to our center via airlift on continuous positive airway pressure and was discharged home 7 weeks postoperatively on room air. At 8 months, neurodevelopmental progress remains normal. Follow-up echocardiography revealed no RV-to-PA conduit stenosis or valvar insufficiency and preserved biventricular systolic function. The patient has progressed well, with normal growth and development during the most recent follow-up.
Discussion
Aortic atresia is a rare congenital heart defect, occurring in approximately 2 per 100,000 live births. 2 It results from posterior deviation of the conal septum, leading to hypoplasia of the aortic valve and ascending aorta, typically accompanied by an outlet VSD that allows formation of 2 well-developed ventricles.1,3 The coexistence of AA with IAA is exceedingly uncommon, with only a few cases reported. 1 Interrupted aortic arch is classified into 3 types, with Type B (interruption between the left carotid and left subclavian arteries) being the most common. These defects are frequently associated with DiGeorge syndrome, as in the present case.
When AA occurs alongside IAA, the blood supply to the coronary arteries and central nervous system becomes entirely dependent on collateral circulation from the descending aorta. In the literature, this rare combination is most frequently reported with Type C IAA, and less commonly with Type B.1,4–7 Most documented cases of AA with IAA involve additional vascular anomalies—such as bilateral ductus arteriosus, double aortic arch, aberrant right subclavian artery, an aortopulmonary window, or other collateral vessels—that help maintain perfusion of vital organs.1,5 Our case is particularly noteworthy as it involves AA with Type B IAA, without any additional cardiac circulatory vascular anomalies such as those mentioned previously to support coronary or cerebral circulation. In addition, this case was complicated by additional cerebral vascular hypoplasia of the internal carotid and right middle and anterior cerebral arteries. These findings posed additional major surgical and clinical risks.
Although data on survival in cases of isolated AA with IAA Type B—without additional circulatory support and with complex cerebral vascular anatomy—are limited, after thorough discussions with the family, we opted to pursue all available treatment options. Given the infant's full-term birth, normal birth weight, initial stabilization, and our timely referral to a center with prior successful surgical experience on similar patients, we were able to achieve an optimal outcome. This case underscores the challenges of managing such rare congenital cardiovascular anomalies and the importance of early, expert intervention for achieving optimal outcomes.
Supplemental Material
Supplemental Material
sj-pdf-1-pch-10.1177_21501351261423197 - Supplemental material for A Rare Case of Aortic Atresia and Interrupted Aortic Arch Type B Survival, Anatomic Importance of a Vertebral Artery and the Circle of Willis, a Case Report and Review of the Literature
Supplemental material, sj-pdf-1-pch-10.1177_21501351261423197 for A Rare Case of Aortic Atresia and Interrupted Aortic Arch Type B Survival, Anatomic Importance of a Vertebral Artery and the Circle of Willis, a Case Report and Review of the Literature by Anusha Bai Kalithkar, Juanita Montoya Arango, Phillip Zegelbone, Christopher Schettino, Sethuraman Swaminathan and Jaime Alkon in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Abbreviations
Author Contributions
ABK collected data, drafted the initial manuscript, and reviewed and revised the manuscript. JMA contributed to the initial manuscript. PZ coordinated and supervised data collection, reviewed, and revised the manuscript. CS coordinated the imaging figures. SS coordinated and supervised data collection, critically reviewed, and revised the manuscript. JA conceptualized, coordinated, and supervised data collection, critically reviewed, and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.