
Abstract
Background
Despite advances in congenital heart surgery (CHS) and improvements in outcomes, disparities continue to exist. Social Drivers of Health (SDoH) have been associated with many aspects of health and wellness including congenital heart disease. The goal was to evaluate the impact of individual and neighborhood-level SDoH on outcomes following CHS.
Methods
Retrospective review of the Society of Thoracic Surgeons Congenital Heart Surgery Database from 2014 to 2022 linked via ZIP code with the Centers for Disease Control and Prevention Social Vulnerability Index (SVI). ZIP codes were ranked by their SVI score with the first quintile the least vulnerable and the fifth the most vulnerable. The primary outcome was STS perioperative mortality.
Results
A total of 49 centers with ≥85% ZIP code completion rate were included. Those with missing ZIP codes (n = 1329) or missing data (n = 5651) were excluded resulting in a final cohort of 16,238 (69.5%, 11,285/16,238) cases. Of the final cohort, 8,977/16,238 (55.3%) were Non-Hispanic White and 7084/16,238 (43.6%) had private insurance. There were 448/16,238 (2.8%) STS perioperative mortalities. In the fully adjusted model, individual Non-Hispanic Black race (OR:1.76 [95% CI: 1.20-2.52]), Non-Hispanic Other race (OR: 2.39 [95% CI: 1.10-4.99]), Medicaid (OR:1.55 [95% CI: 1.04-2.30]), None/Self/Charity Insurance (OR:2.60 [95% CI: 1.09-5.93]), as well as increasing SVI quintile with SVI2 (OR: 1.22 [95% CI: 0.86-1.75]), SVI3 (OR: 1.71 [95% CI: 1.07-2.73]), SVI4 (OR: 1.92 [95% CI: 1.04-3.53]) and SVI5 (OR: 3.09 [95% CI: 1.36-6.87]), had increased odds of STS perioperative mortality.
Conclusions
After adjusting for clinical characteristics, both individual and neighborhood Social Drivers of Health conferred increased odds of perioperative mortality following CHS. These results spotlight the disparities driven by individual circumstances beyond clinical characteristics and reinforce the need to intervene at both the individual and community levels to improve outcomes.
Keywords
Background
Advances in medical and surgical care have resulted in improved survival for children born with congenital heart disease (CHD).1,2 However, significant variability in CHD surgical outcomes still exists. 3 A portion of this variability may be explained by disparities in outcomes following CHD surgery across individual Social Drivers of Health (SDoH) domains, such as race/ethnicity, income, education, and insurance status. 4 In addition to individual factors, the SDoH of the area where individuals live and work have been shown to be related to many aspects of health and health outcomes.5–7 These neighborhood-level SDoH have been associated with outcomes after CHD surgery in single center, administrative database, such as the Pediatric Hospital Information System (PHIS), analyses, and using the Pediatric Heart Network–Single Ventricle Reconstruction Trial cohort analyses with those from more disadvantaged areas having worse outcomes.8–10
It has become increasingly clear over the last decade that both individual and neighborhood-level SDoH impact operative outcomes for children undergoing CHD surgery. While this knowledge has been informative for the CHD community at large, the CHD population is highly heterogeneous, including >200 different diagnoses and >200 different procedures. Data thus far have either focused on single ventricle/transplant patients or have grouped all CHD patients into one cohort, using established, yet highly imperfect, risk stratification. Few actionable data exist that quantify effects of SDoH for specific CHD populations, such that tailored interventions can be developed to improve outcomes for the most vulnerable populations. Thus, we leveraged the leading, national, CHD surgical registry, linked to neighborhood-level measures of SDoH, to quantify the relative impacts of race/ethnicity, payor, and neighborhood for the 10 Society of Thoracic Surgeons – Congenital Heart Surgery Database (STS-CHSD) defined “benchmark procedures”—the 10 most common, most homogeneous, congenital heart surgery procedures performed in the USA.
Methods
Data Sources
Society of Thoracic Surgeons Congenital Heart Surgery Database
The STS-CHSD contains > 600,000 operations from > 113 centers in North America. 11 The registry includes demographic, preoperative, perioperative, and outcomes data.
Center for Disease Control and Prevention Agency for Toxic Substances and Disease Registry Social Vulnerability Index (SVI)
The SVI, used to rank neighborhood SDoH, ranks U.S. Census tracts based on a range of social factors across four different subscales (Socioeconomic Status [SES], Household Characteristics, Race and Ethnic Minority Status, and Housing Type and Transportation). Tracts are ranked from 0 to 1 in each domain as well as for the overall social vulnerability index. 12 ZIP codes were ranked by their SVI score and four domain scores independently and binned into quintiles with the first quintile containing the least vulnerable ZIP codes and the fifth quintile containing the most vulnerable ZIP codes.8,13–15
Approvals
The data were provided by The Society of Thoracic Surgeons’ National Database Participant User File Research Program. 16 Data analysis was performed at the Dell Medical School at The University of Texas at Austin and was deemed non-human subjects research by the Dell Medical School at The University of Texas at Austin IRB (IRB# 2019070078).
Patient Population
The STS-CHSD was retrospectively queried from 6/2014-6/2022 for all patients from the USA < 18 years of age who underwent one of the 10 benchmark operations (Table 1). Centers with ≥ 85% completed ZIP codes were included. Individual patients with missing/undefined ZIP codes, demographics, or outcomes (mortality, readmission, and length of stay [LOS]) were excluded.
Patient Characteristics by Benchmark Operation and Comparing Included and Excluded Patients.
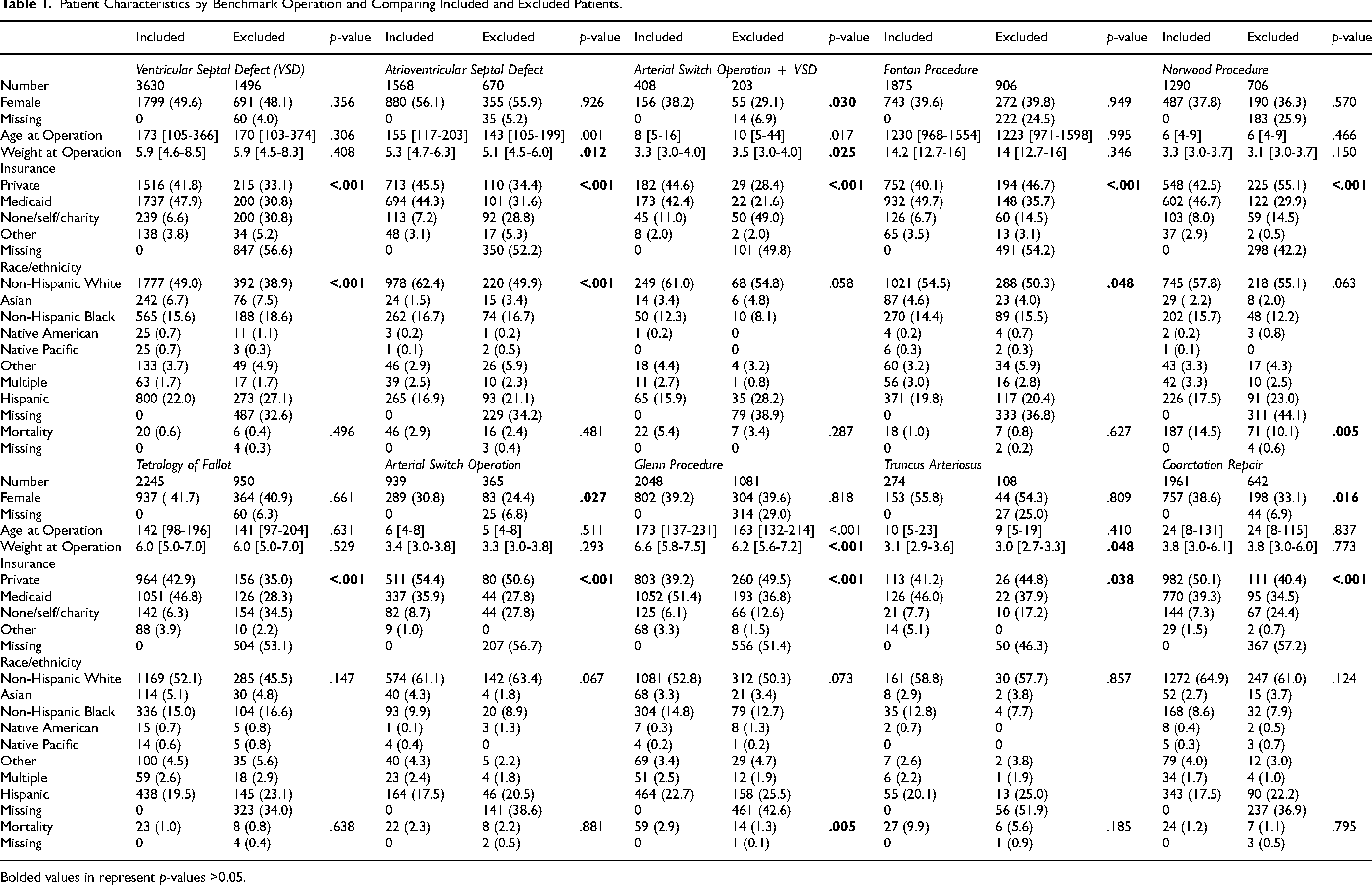
Bolded values in represent p-values >0.05.
Outcomes
Primary Outcome
The primary outcome was perioperative mortality, defined as death before hospital discharge or within 30 days after benchmark operation, whichever was longer.
Secondary Outcomes
Secondary outcomes included total LOS and postoperative LOS (poLOS), 30-Day readmission, and a composite of complications as defined by the STS-CHSD and considered positive if a patient had at least one of the included complications.17,18
Data Linkage
ZIP codes were converted to U.S. Census tracts using the Housing and Urban Development ZIP code crosswalk. 19 Where ZIP codes resided in multiple census tracts, the tract which contained the largest percentage of the ZIP code's population was selected. 20 Each tract was given a random unique identifier by the STS Research Team in order to de-identify the dataset. Additionally, individual centers were de-identified and given unique identifiers.
Analysis
A sensitivity analysis was performed to evaluate any differences between included and excluded centers and patients. As no benchmark procedure specific risk models exist, the 2019 STS-CHSD Mortality Risk Model was utilized to calculate risk scores for each patient. 21 Bayesian logistic multivariable regression modeling with mixed effects was used to analyze binary outcomes and Bayesian linear multivariable regression modeling with mixed effects was used to analyze continuous outcomes after log transformation for non-normality. The posterior distributions of the parameters were estimated using Markov Chain Monte Carlo (MCMC) sampling. Four MCMC chains were run, each with up to 3000 iterations, including 1000 warm-up iterations. Convergence of the MCMC chains was assessed using the potential scale reduction factor, with values close to 1.00 indicating convergence. Effective sample sizes were also examined to ensure sufficient precision of the posterior estimate. The results of the Bayesian regression models were summarized using the posterior mean (point estimate) and 95% credible intervals (95% CI) for each parameter. Predictors with 95% CIs that excluded 1 for odds ratios or excluded 0 for percent change were considered to have strong evidence of an association with the outcome. Factors included in the model include those of known clinical relevance and those found to be statistically significant in univariate analysis. Operating center was treated as a random effects parameter. Individual models for each benchmark procedure were unable to be performed given the low number of mortalities in each procedure, aside from the Norwood procedure. Therefore, a single model with the benchmark operations included as a categorical variable was used. As the STS-CHSD Mortality Risk Score was developed for congenital heart surgery broadly and not specifically for the benchmark procedures, it was evaluated for differences in the score between benchmark procedures and a statistically significant association was identified (P < .001). An interaction term for benchmark procedure and STS-CHSD Mortality Risk Score was included in the final models and was nonsignificant (OR: 0.98, 95% CI: 0.94-1.01). Interaction terms between individual and neighborhood SDOH were included in models where indicated to account for the complex relationships between them. A mediation analysis was performed to assess the role SVI plays in mediating the impact of race/ethnicity on perioperative mortality. A fully adjusted model was utilized which risks overfitting and biases mediation analysis findings towards the null. Analysis was performed utilizing R and RStudio. 22
Results
A total of 49 centers representing all regions were included (Table S1). The median percent of ZIP codes entered was 96.2% [IQR: 93.3%-98.7%] (Figure 1). There were 23,365 benchmark cases of which 1359 (5.8%) had missing ZIP codes and 5768 (24.7%) had missing SDoH or outcomes data resulting in a final cohort of 16,238 (69.5%) cases (Figure 2). When comparing patient characteristics and outcomes for included and excluded centers, there were small but statistically significant differences in sex, insurance, benchmark case distribution, preoperative factors, and 30-day readmission. These differences did not show any consistent directionality (Tables S2-S5).
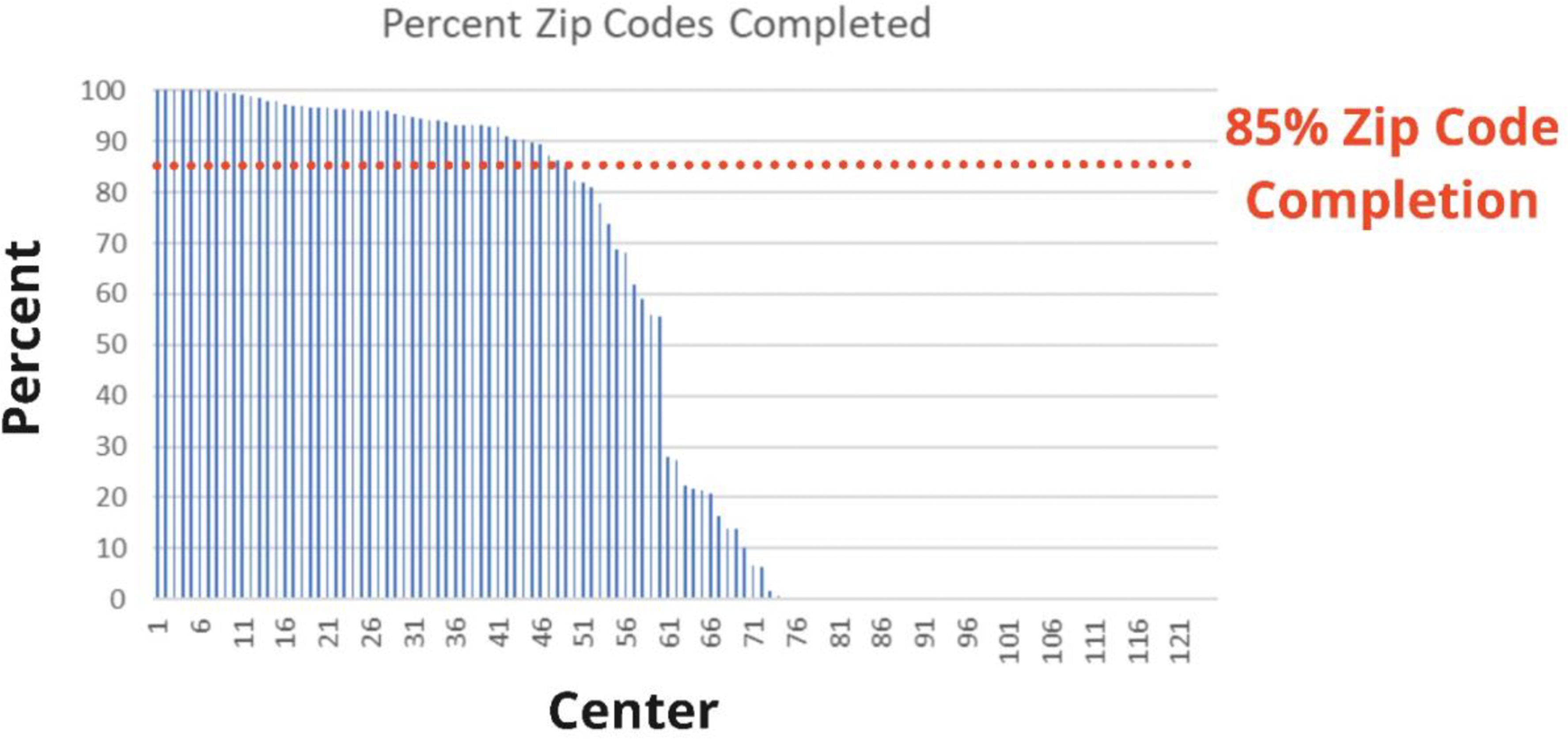
Percent of ZIP codes completed by center.
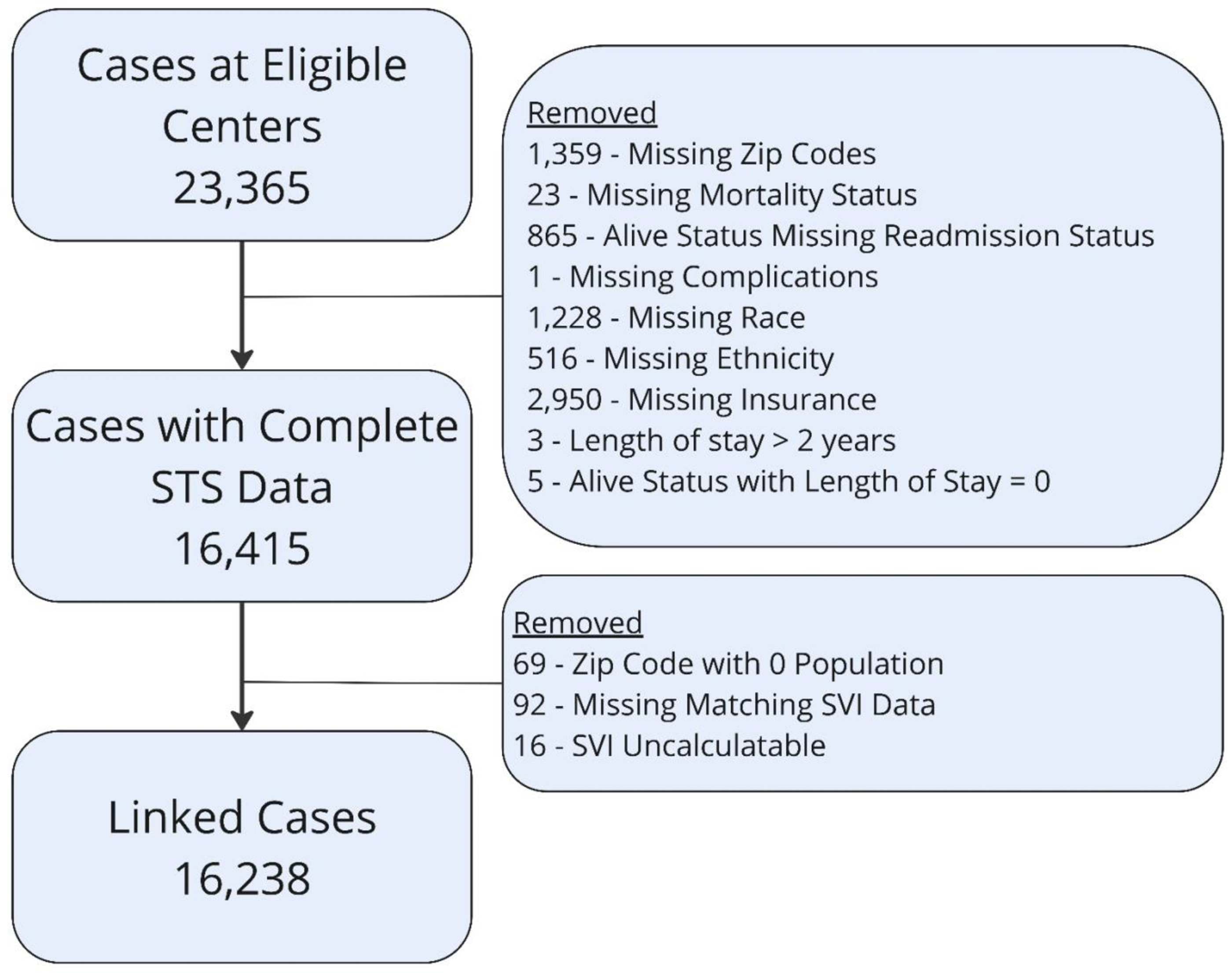
Consort diagram. Abbreviations: STS, Society of Thoracic Surgeons; SVI, Social Vulnerability Index.
Cohort Characteristics
Of the included cohort, 8977/16,238 (55.3%) were Non-Hispanic White, 7003/16,238 (43.1%) were female, and 7084/16,238 (43.6%) had private insurance. Ventricular septal defect repair was the most frequent operation, accounting for 3630/16,238 (22.4%) of the cases (Table 1). When comparing included to excluded benchmark operations, significant missingness was present for the excluded operations in both race/ethnicity and insurance data (range: 32.6%-57.2%) (Table 1). Significant differences in distribution of insurance were identified across all benchmark operations (All P < .038). A significant difference in mortality was identified in the Norwood [n = 187/1290 (14.5%) versus n = 71/706 (10.1%), P = .005] and Glenn [n = 59/2048 (2.9%) versus n = 14/1081 (1.3%), p = .005] procedures (Table 1).
Outcomes
There were a total of 448 (2.8%) mortalities. Median LOS and poLOS, excluding mortalities, were 9 [IQR:5-22] and 8 [IQR:5-16] days respectively, with 2364/16,238 (15.0%) of those surviving having a composite complication. Readmission within 30 days occurred in 1798/16,238 (11.4%) who survived to discharge.
Social Drivers of Health and Outcomes
Individual SDoH
In univariate analysis, race/ethnicity and insurance status were each associated with operative mortality, composite complications, 30-day readmission, LOS, and poLOS (Table S6).
Neighborhood SDoH
Overall SVI was associated with composite complications, 30-day readmission, LOS, and poLOS (Table S6). Additionally, the SES subscale was associated with composite complications, 30-day readmission, LOS, and poLOS. The Household Characteristics subscale was associated with composite complications, LOS, and poLOS. The Housing and Transportation subscale was associated with perioperative mortality, composite complications, LOS, and poLOS (Table S7).
Multivariable Model
Perioperative Mortality
Medicaid insurance (OR:1.55, 95% CI: 1.04-2.30) and None/Self/Charity Care insurance (OR: 2.60, 95% CI: 1.09-5.93), Non-Hispanic Black race (OR: 1.76, 95% CI: 1.20-2.52) and Other race (OR: 2.39, 95% CI: 1.10-4.99), and increasing SVI quintiles were associated with increased odds of mortality with quintiles 3 (OR:1.71, 95% CI: 1.07-2.73), 4 (OR: 1.92, 95% CI: 1.04-3.53), and 5 (OR: 3.09, 95% CI: 1.36-6.87) reaching significance (Table 2). In separate models, more vulnerable quintiles in the SVI SES subscale was associated with perioperative mortality, with quintiles 2 (OR: 1.50, 95% CI: 1.04-2.12), 3 (OR: 1.69, 95% CI: 1.03-2.74), 4 (OR: 2.62, 95% CI: 1.36-4.99), and 5 (OR:2.91, 95% CI: 1.22-6.73,) having increased adjusted odds. Additionally, the Racial and Ethnic Minority Status subscale with quintile 4 (OR: 2.08, 95% CI: 1.02-3.95) and 5 (OR: 2.71, 95% CI: 1.05-6.40), and Housing Type and Transportation subscale with quintile 5 (OR: 2.36, 95% CI: 1.06-5.22) were associated with increased odds of perioperative mortality (Table S8).
Multivariable Models of Individual and Neighborhood Social Drivers of Health and Outcomes.
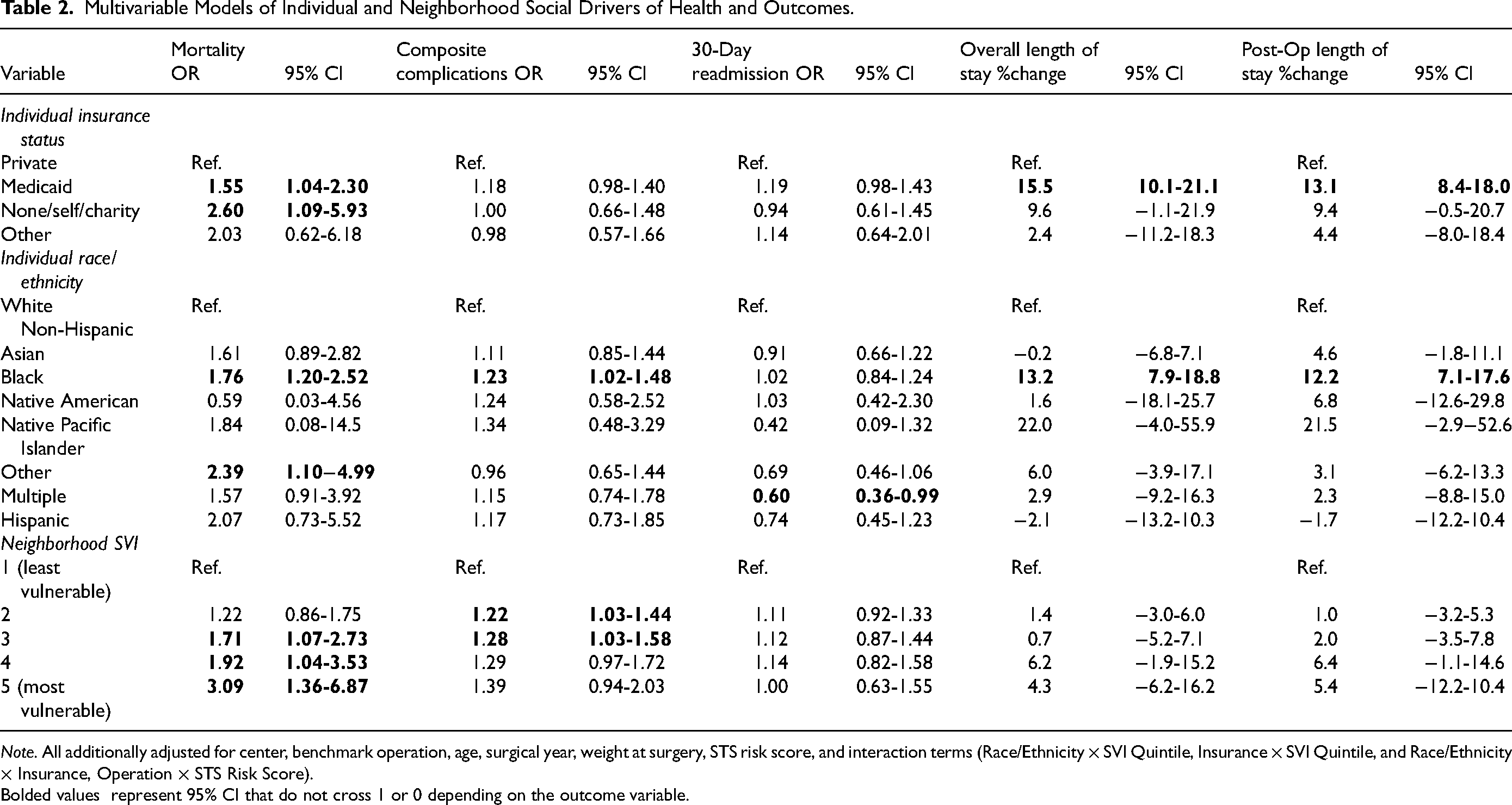
Note. All additionally adjusted for center, benchmark operation, age, surgical year, weight at surgery, STS risk score, and interaction terms (Race/Ethnicity × SVI Quintile, Insurance × SVI Quintile, and Race/Ethnicity × Insurance, Operation × STS Risk Score).
Bolded values represent 95% CI that do not cross 1 or 0 depending on the outcome variable.
Composite Complications
Excluding mortalities, Non-Hispanic Black race (OR: 1.23, 95% CI: 1.02-1.48) and increasing SVI quintiles were associated with increasing odds of composite complications, with quintiles 2 (OR: 1.22, 95% CI: 1.03-1.44,) and 3 (OR: 1.28, 95% CI: 1.03-1.58) reaching significance (Table 2). In separate models, the Neighborhood Housing Type and Transportation quintile 2 (OR: 1.32, 95% CI: 1.12-1.56) and 4 (OR: 1.40, 95% CI: 1.04-1.87) as well as the Household Characteristics subscale quintile 5 (OR :1.53, 95% CI: 1.03-2.23) were associated with increased odds of composite complication (Table S8).
30-Day Readmission
Only the multiple race category (OR: 0.60, 95% CI: 0.36-0.99) was significantly associated with odds of 30-day readmission (Table 2 and S8).
Length of Stay
Medicaid insurance was associated with longer LOS (15.5%, 95% CI: 10.1%-21.1%) and poLOS (13.1%, 95% CI: 8.4%-18.0%) as was Non-Hispanic Black race (LOS:(13.2%, 95% CI: 7.9%-18.8%) and poLOS: [12.2%, 95% CI: 7.1%-17.6%]) (Table 2 and Table S8).
Mediation Analysis
Social Vulnerability Index mediated 5.5% (95% CI: 0.3%-17.0%) of the association between Black race and perioperative mortality. No other percent mediated was significant (Table S9).
Subgroup Analyses of Perioperative Mortality
Insurance
In those with private insurance, no individual or neighborhood SDoH factors were associated with perioperative mortality (Table S10). In those with Medicaid insurance, Non-Hispanic Black race (OR:2.01, 95% CI: 1.32-3.06), Other race (OR:3.93, 95% CI: 1.57-9.54), and Hispanic (OR: 3.50, 95% CI: 1.45-8.30) were associated with increased odds of perioperative mortality (Table S10).
Norwood Procedure
The Norwood procedure was the only benchmark procedure with a sufficient number of mortalities to perform a robust multivariable analysis. Medicaid insurance status (OR: 2.34, 95% CI: 1.18-4.77), None/Self/Charity insurance status (OR:5.32, 95% CI: 1.26-26.48), and Asian race (OR: 0.12, 95% CI: 0.01-0.90) were associated with perioperative mortality (Table S10).
Discussion
In this analysis of a large, national, clinical registry of CHD surgery, linked at the ZIP code level with neighborhood SDoH, both individual and neighborhood level SDoH were associated with outcomes following CHD surgery. These associations persisted after adjustment for center and known clinical factors associated with CHD surgical outcomes. Importantly, Medicaid and None/Self-Pay/Charity insurance status, Non-Hispanic Black and Other race, and more disadvantaged neighborhood quintiles as measured by SVI were associated with increased adjusted odds of perioperative mortality following an STS benchmark CHD surgery.
Similar to previous reports, Non-Hispanic Black and Other race were found to confer increased odds of perioperative mortality.8,23 Additionally, Medicaid and None/Self/Charity insurance status conferred increased adjusted odds of perioperative mortality. These proved to be independent risks while adjusting for neighborhood vulnerability, individual clinical risk factors, and center. Compared to prior evaluations, this analysis allowed for more granular risk stratification and the evaluation of discreet, well defined surgical interventions across a larger, more diverse, patient population allowing a more robust comparison.
Previous work has evaluated different measures of how vulnerable or disadvantaged a neighborhood is in relation to CHD surgical outcomes. These have suggested a threshold effect of neighborhood disadvantage where negative effects occur above a certain level of disadvantage.8,24 In this study, results were not consistent with a threshold. Instead, increasing disadvantage was found to have increasing adjusted odds of perioperative mortality. This was present even with adjustment for individual SDoH and clinical factors.
Among the SVI subscales, SES Status showed the most robust association with perioperative mortality with Race and Ethnicity Minority Status and Housing Type and Transportation showing less robust associations. This suggests that the factors in the SES scale (percent population below 150% of the federal poverty line, unemployment, housing cost burden, percent of population with no high school diploma, and uninsured), may be the prominent drivers of the association with overall SVI. These factors represent population financial and education characteristics more than demographics or the built environment. These factors represent interesting targets for population health-based intervention as all are potentially modifiable.
Other measures of neighborhood disadvantage exist, including the Area Deprivation Index (ADI) and the Childhood Opportunity Index (COI). 25 While each index was developed with a different underlying purpose, there is significant overlap in the factors making up the indicies. 26 Importantly, these indices have significant correlation with each other and have shown similar correlations with health measures in pediatric populations.26,27 While the overall indices of the SVI, ADI, and COI have been shown to be mostly interchangeable, future work evaluating the individual unique factors contained in each index may provide additional insight into the drivers of the association between neighborhood disadvantage and CHD outcomes.
Interestingly, Non-Hispanic Black, Hispanic, Multiple race, Medicaid insurance, and more disadvantaged SVI quintiles all had an increased adjusted odds of having a composite complication. A suggestion of increased odds of complications in Non-Hispanic Black has been previously reported. 28 This increase in complications may, at least partially, drive the increased mortality. However, the association remains even when excluding mortalities. A mechanism for the increase in complications cannot be ascertained from this analysis and may include factors such as differential access to prenatal care, bias in the care received, social stressors, and unmeasured or unknown physiologic or biologic differences.
While Non-Hispanic Black race and Medicaid insurance were also found to have increased LOS and poLOS after adjustment, neighborhood-level SDoH was not. The increased LOS potentially reveals families with reduced abilities to provide the frequently complex necessary care for their child at home postoperatively. Additionally, only multiple race was associated with 30-day readmission. Previous work has shown associations with modest effect sizes for 30-day readmission for Hispanic, and government insurance.29,30 The current study focuses on the STS benchmark cases while previous studies have included all cases. This difference in included case types may account for the differences in the associations with 30-day readmission as only utilizing the benchmark cases excludes a wide range of significantly complex operations who may have different risk profiles for readmission.
The interaction between individual and neighborhood level SDoH is complex. When evaluating only those with private insurance, other individual and neighborhood SDoH were no longer associated with perioperative mortality. Conversely, within the Medicaid group, Non-Hispanic Black and Other race, continued to confer increased odds of perioperative mortality in addition to Hispanic now having increased adjusted odds. This suggests access and ability to obtain private insurance may mediate some of the negative consequences of other SDoH factors.
The pathways between SDoH factors and differences in outcomes are assuredly multifactorial. Multiple social and systemic pathways have been proposed including access to any care, access to quality care, systemic racism and, implicit bias. 31 Unfortunately, deidentified ZIP codes and centers precluded evaluation of differential access. There is also a growing body of evidence on the biological alterations that occur when individuals, including pregnant individuals, are exposed to stress from social disadvantage, discrimination, and racism. One such biologic alteration is in the hypothalamic-pituitary-adrenal and particularly cortisol levels and response.32–34 These biologic alterations and increased risk of worse health outcomes appears to persist over time.35,36 It is imperative to continue work to alter the structural and systemic healthcare issues that likely contribute to differential outcomes. However, it is just as imperative to further investigate biologic alterations and differences that may be targets of medical intervention to improve outcomes.
It is important to note that these data should not be taken as support for inclusion of individual or neighborhood-level SDoH in risk or outcomes modeling for congenital heart surgery. Inclusion of adjustment for SDoH may result in masking important differences and disparities that require intervention. Instead, these data should be taken as a signal for the imperative to expand the focus of care and intervention beyond the traditional clinical settings and into the communities.
Limitations
This is a retrospective review which prohibits the assessment of causality. Additionally, a significant number of centers reported no or few patient ZIP codes and were excluded from the analysis. While the sensitivity analysis revealed no meaningful differences between included and excluded centers, other unmeasured differences could still exist potentially biasing the analysis and/or reducing the generalizability of these data. As only the patient ZIP code of residence and not the complete address was known, the individuals could not be geocoded to a specific census tract. Where multiple census tracts fall within a single ZIP code, it is possible that the characteristics assigned to that ZIP code are not representative of the census tract where the individual actually resides. However, it would be expected that this misclassification would be random; thus, biasing towards the null. Surgery-specific and detailed subgroup analyses were limited due to relatively small numbers of outcome events, particularly perioperative mortalities, which prevented the ability to perform multivariable regression analysis. As the STS-CHSD and SVI only provide an assessment of individual and neighborhood level SDoH at a single time point, the impact of duration of exposure and changes in exposure is unable to be evaluated preventing the assessment of potentially more nuanced associations with SDoH. Lastly, the STS-CHSD does not capture longer-term outcomes on which SDoH may have even greater impact.
Conclusions
In a large national clinical registry for CHD surgery individual and neighborhood level Social Drivers of Health were associated with perioperative mortality after adjusting for clinical risk factors. These data reinforce the fact that individual circumstances beyond clinical characteristics play a significant role in health outcomes. As these individual and neighborhood-level SDoH likely contribute to differences in outcomes across a spectrum of health conditions, these data should galvanize the health care community at large to continue work to further characterize mechanisms of action and to remove systemic barriers to care and best potential outcomes.
Supplemental Material
sj-docx-1-pch-10.1177_21501351261418279 - Supplemental material for Impact of Neighborhood and Individual Social Drivers of Health on Outcomes Following Congenital Heart Surgery
Supplemental material, sj-docx-1-pch-10.1177_21501351261418279 for Impact of Neighborhood and Individual Social Drivers of Health on Outcomes Following Congenital Heart Surgery by Andrew Well, Heather Van Diest, Brett R. Anderson, Wei Zhang, Kathleen Carberry, Alexandra Lamari-Fisher, Jeremy T. Affolter, Erin A Gottlieb, Jeffery P. Jacobs, Charles D. Fraser and Carlos M. Mery in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Acknowledgments
The data for this research were provided by The Society of Thoracic Surgeons’ National Database Participant User File Research Program. Data analysis was performed at the investigators’ institutions. The views and opinions presented in this article are solely those of the authors and do not necessarily represent those of The Society of Thoracic Surgeons. This research was determined to be exempt research with a waiver of informed consent from Advarra Institutional Review Board (Mod01760092, Version 1.1, Approval date 17 July 2023).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.