
Abstract
Keywords
Introduction
Aortic valve neocuspidization (AVNeo), initially proposed by Ozaki 1 for the treatment of AV disease in adults and the elderly, is recently gaining increasing attention in pediatric patients.2–4 In fact, given the unique anatomical and physiological features in children, AV reconstruction using autologous pericardium has emerged as a promising alternative to traditional methods for its potential advantages over valve replacement or repair. The AVNeo procedure aims to preserve the natural anatomy of the aortic root while allowing a physiological laminar flow pattern 5 and its growth potential. As a result, several pioneering pediatric hospitals worldwide have focused on adapting this technique to pediatric patients.6–8 Preliminary short-term reports have shown promising results2,7 although concerns have been raised regarding the use of materials other than autologous pericardium, the incidence of endocarditis, and the questions from the scientific community about the durability of the repair.4,6,9 In fact, despite the remarkable medium- and long-term results in the adult and elderly population reported in the literature10–13 there is still a lack of follow-up data to conclusively support or dismiss the use of the AVNeo procedure in the pediatric age group. The aim of this study is to analyze the results of a single-center case series that began 8 years ago to determine whether the AVNeo procedure has a viable role in pediatric patients and, if so, to identify the most appropriate areas for its application.
Material and Methods
This is a single center retrospective observational cohort study enrolling all patients who successfully underwent the AVNeo procedure at the Bambino Gesù Children's Hospital IRCCS between July 2016 and August 2024. Given the retrospective nature of the analysis, our study, whose protocol complies with the ethical guidelines of the Declaration of Helsinki, did not require approval from the local ethics committee and patient consent was waived according to current legislation, although a notification was sent.
We offered AVNeo to a consecutive series of patients with acquired or congenital AV disease, sometimes with aortic annulus hypoplasia and/or other associated cardiac pathologies. We defined simple associated annular enlargement both 1-sinus or 2-sinus widening of the aortic annulus, whereas complex associated procedures included mainly concomitant relief of subaortic obstruction.
Surgical technique used in our institution was video detailed and made available on the web in 2022. 14 Valve leaflets were trimmed out from either pretreated native autologous pericardium or glutaraldehyde- (CardioCel®, Milton, Australia) or photo-oxitized (Photofix®, Crylife, Kennesaw, GA, USA) decellularized bovine pericardium using the original Ozaki apparatus (Sanamedi, Inc., Tokyo, Japan). Exclusive use of heterologous pericardium was performed both in previously unoperated patients and in reoperations in the first part of our series (up to March 2018) when, for internal hospital regulatory reasons, the intraoperative use of glutaraldehyde solution was not yet permitted. Subsequently, we moved to the exclusive use of pretreated autologous pericardium, reserving the heterologous pericardium exclusively for reoperations in which no suitable autologous pericardium was available. Pretreatment of the autologous pericardium consisted of its fixation on the appropriate metal support, cleaning of pericardial fat and treatment with buffered 0.6% glutaraldehyde solution for 5 min in patients up to 15 years of age, for 7 min in patients up to 18 years of age and for 8 min in young adults followed by 3 final rinsings of 6 min each in saline solution.
Either single or both-sinus enlargement of the aortic annulus 15 was associated in patients with annular Z-scores below −2 and in any case when native annulus measured less than 15 mm. 7 Associated complex left ventricular outflow tract obstruction was addressed with a concomitant Konno operation. Mitral valve (MV) replacement was associated with cases of unrepairable MV disease. The adequacy of repair was assessed intraoperatively after weaning the patient from cardio-pulmonary bypass by transesophageal echocardiography (TEE).
Every patient underwent transthoracic echocardiography (TTE) before discharge and followed every 6 months by TTE in our outpatient clinic. For a few patients referred from elsewhere, echocardiographic reports were obtained from the referring cardiologist. The antiplatelet/anticoagulant policy, standardized since July 2018, was based on initial anticoagulant therapy with warfarin (target international normalized ratio progressively increased to 2-2.5) for 3 months, followed by long-term antiplatelet treatment.
For the study, a single reviewer independently made calculations on preoperative, postoperative, and follow-up TTE images with a second reviewer analyzing a random sample. The AV annulus and the peak gradients across the AV were measured in parasternal long axis view. The aortic valve incompetence (AVI), determined by vena contracta (VC) jet width was measured in parasternal long axis views and indexed to the patients body surface area (BSA). Finally, leaflet mobility of AVNeo was observed in parasternal long- and short-axes views, using 3D imaging where applicable. Categorization of aortic valve stenosis (AVS) and aortic valve incompetence (AVI) was performed in accordance with Baird et al. 7
Statistical Analysis
Continuous variables are presented as medians with interquartile ranges or means with standard deviations (SD), as appropriate. Normality was assessed using the Shapiro-Wilk test. Comparisons between continuous variables were performed using Student's t-test for normally distributed data and the Wilcoxon rank-sum test for nonparametric comparisons. For repeated measurements, the Wilcoxon signed-rank test was applied. Categorical variables are reported as frequencies and percentages and were compared using chi-square or Fisher's exact tests, as appropriate.
A time-to-event analysis was performed using Kaplan-Meier estimates, with survival distributions compared via the log-rank test. Logistic regression models were used to evaluate associations between redo surgery or death, whichever occurred first, and relevant clinical variables, with odds ratios (OR) and 95% confidence intervals (CIs) reported. The choice of variables for the multivariable model was dictated by clinical relevance.
To assess differences in peak aortic gradient across different leaflet materials, one-way analysis of variance was applied, with post hoc pairwise comparisons where necessary. Aortic annular growth over time was assessed using indexed and paired comparisons. Missing data were handled using listwise deletion where necessary. A 2-tailed P-value <.05 was considered statistically significant.
The primary outcome measure was a redo procedure or death, whichever occurred first.
Statistical analyses were performed using Stata version 11.1 (StataCorp LP, College Station, TX, USA).
Results
From July 2016 to August 2024, we performed the AVNeo procedure in 49 patients. Preoperative characteristics are summarized in Table 1. Median age and weight were 13.8 years (10.9-16.3) and 55 kgs (33-66) respectively. Of the cohort, 32/49 (65.3%) were male. Patients were categorized into 3 age groups: 14/49 patients (28.6%) were between 1 and 10 years (Group I, children), 31/49 (63.2%) were11-18 years (Group II, adolescents), and 4/49 (8.2%) were 19-25 years (Group III, young adults). The prevalent AV defect was incompetence in 29/49 (59.2%) followed by stenosis in 20/49 cases (40.8%). Functional classification 16 of prevalent AVI was as follows: Type II in 8/29 cases (27.6%) and Type III in 21/49 (72.4%). Preoperative measurements showed an AV peak and mean gradient of 60 (12.6-77.5) and 33 (5.5-46.5) mm Hg respectively, with a VC and indexed vena contracta jet width (IVC) of 6.8 (2.2-7.4) and 4.2 (1.8-5.8) mm respectively.
Preoperative Characteristics.
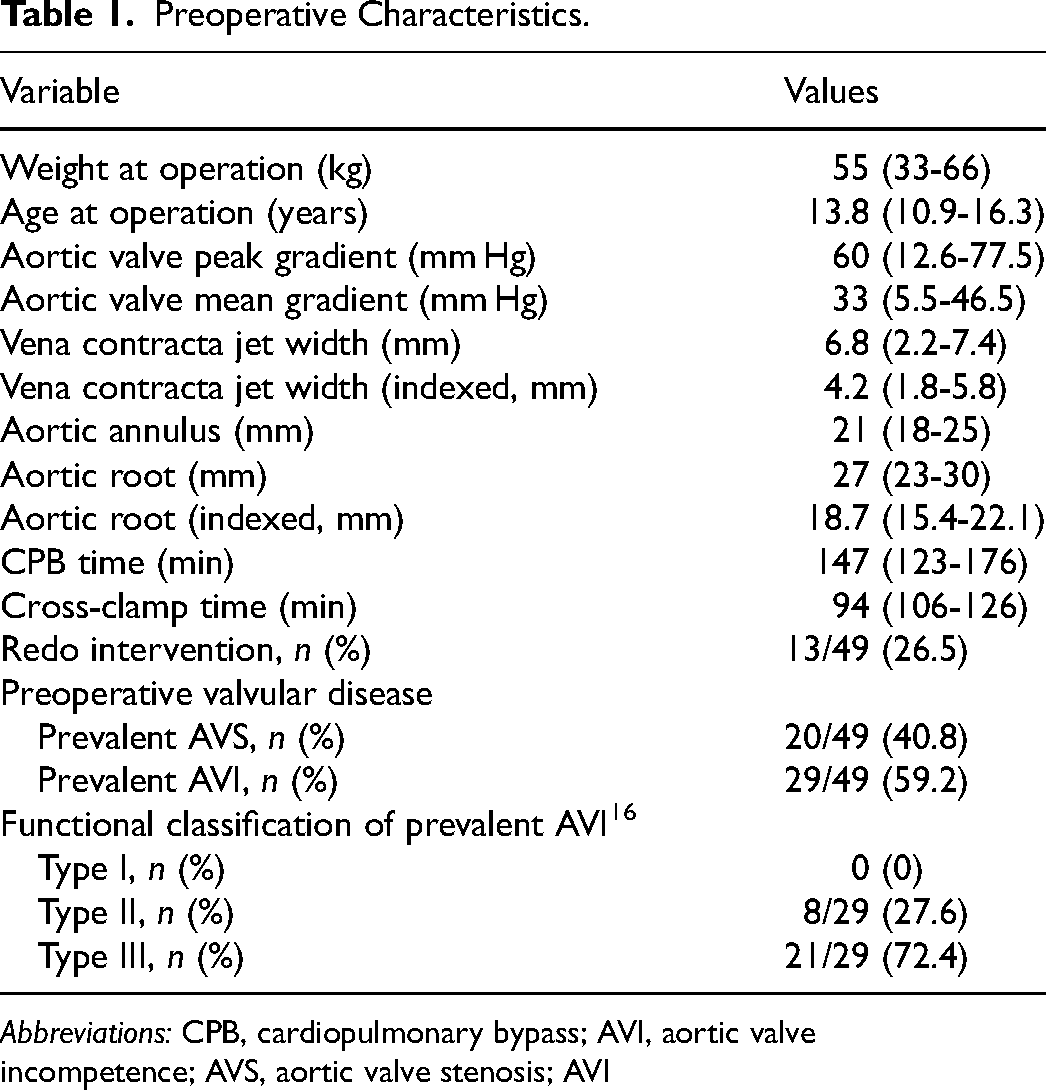
Abbreviations: CPB, cardiopulmonary bypass; AVI, aortic valve incompetence; AVS, aortic valve stenosis; AVI
In terms of AV valve morphology, 18/49 (37%) patients had tricuspid valves, 21/49 (43%) had bicuspid valves, and 8/49 (16%) had unicusp valves. Two of 49 patients (4%) had structural degeneration of a bioprosthesis, stented in one case and stentless in the other; both completely explanted at reoperation to allow neocuspidization on the native aortic annulus. Congenital lesions were predominant, accounting for 39 of 49 cases (80%), while the remaining 10 patients had noncongenital causes, including 8/49 (16%) with a history of rheumatic disease. Of these 49 patients, 13 (26.5%) underwent AVNeo as a redo procedure following previous surgeries (modified Konno procedure in 4, AV repair ± ventricular septal defect (VSD) closure in 3, surgical aortic valve replacement (SAVR) in 2, multiple VSD + tricuspid vlave (TV) repair in 1, mitral valve (MV) repair in 1, arterial switch + VSD closure + aortic arch repair in 1, isolated aortic arch repair in 1).
Autologous pericardium was used in 36/49 patients (73.5%), while bovine pericardium was used in 13/49 patients (26.5%), with Cardiocel® used in 9 cases and Photofix® in 4 cases; the latter is only available in Italy from May 2019 until the end of 2022 due to European Community certification issues. In terms of leaflet reconstruction, 3 equal leaflets were created in 27 cases, and unequal leaflets (2 equal and 1 either larger or smaller) were used in 22 cases (15 with a larger leaflet and 7 with a smaller one).
The median cardiopulmonary bypass (CPB) time was 147 min (123-176). The median aortic cross-clamp time was 94 min (106-126). Concomitant surgical procedures were performed in 12 of 49 cases (24.5%), including simple associated procedures in 6 (single-sinus aortic annular enlargement in 3, double-sinus aortic annular enlargement in 1, reduction aortoplasty in 1, ascending aorta replacement in 1) and complex associated procedures in 6 (aorto-ventriculo-septoplasty (Konno) in 5 and Konno + MV replacement + ECMO in 1). Overall, 43 of 49 patients (87.8%) underwent the AVNeo procedure with or without a simple associated procedure, while 6/49 patients (12.2%) underwent AVNeo alongside a simultaneous complex associated procedure.
Early Results
The median hospital stay was 8 days (5-85). One patient, an 11-year-old boy who had developed severe mitral valve stenosis-insufficiency, severe subaortic stenosis, and moderate-to-severe AVI following neonatal repair of a complete atrioventricular septal defect and aortic coarctation, died 3 days after undergoing a Konno operation with AVNeo (using autologous pericardium) and mechanical mitral valve replacement. The patient, who was transferred from the operating room on ECMO, developed a fatal cerebral hemorrhage despite normal AVNeo function.
Survival/Reoperations
The median follow-up for the whole cohort, based on the last available TTE was 37.8 (13.1-53.9) months with 100% completion. No late deaths occurred. However, 3/49 patients (6%) required early conversion to AVNeo replacement. The first patient was an 8-year-old boy with stenotic bicuspid AV, who developed intermittent myocardial ischemia due to redundancy of the left coronary cusp (Cardiocel® heterologous pericardium) obstructing at times the left coronary ostium. The patient was successfully converted to a Ross procedure 4.9 months after AVNeo. The second patient was a 17-year-old boy who had previously undergone combined MV and AV repair for rheumatic disease. He later underwent the AVNeo procedure, using Cardiocel® heterologous pericardium as a rescue treatment following a failed attempt at mechanical AV replacement. He experienced aseptic aortic root disruption with lung congestion and was successfully converted to homograft aortic root replacement 3.5 months after AVNeo. The third patient was an 11-year-old boy who had been treated twice for complex LVOTO. He developed mediastinitis with an aortic pseudoaneurysm 1.5 months after the Konno operation associated with AVNeo (using autologous pericardium) and was successfully converted to homograft aortic root replacement.
Late reoperations of NeoAV replacement were required in 8/49 (17%) patients due to structural valve degeneration in 4 (all treated with Cardiocel®), endocarditis in 3 (1 treated with Cardiocel® and 2 with autologous pericardium), and aortic wall cusp incorporation (using Photofix®) in 1 patient with associated hypertrophic cardiomyopathy. Regarding the 3 cases of endocarditis that necessitated reoperation, the identified etiological agents were Streptococcus oralis in 1 patient, Staphylococcus epidermidis in the second patient, and an undetermined agent in the third patient. In the first case, dental procedures were documented without primary prophylaxis of bacterial endocarditis. Details are provided in Table 2.
Late Reoperations Following Aortic Valve Neocuspidization (AVNeo).
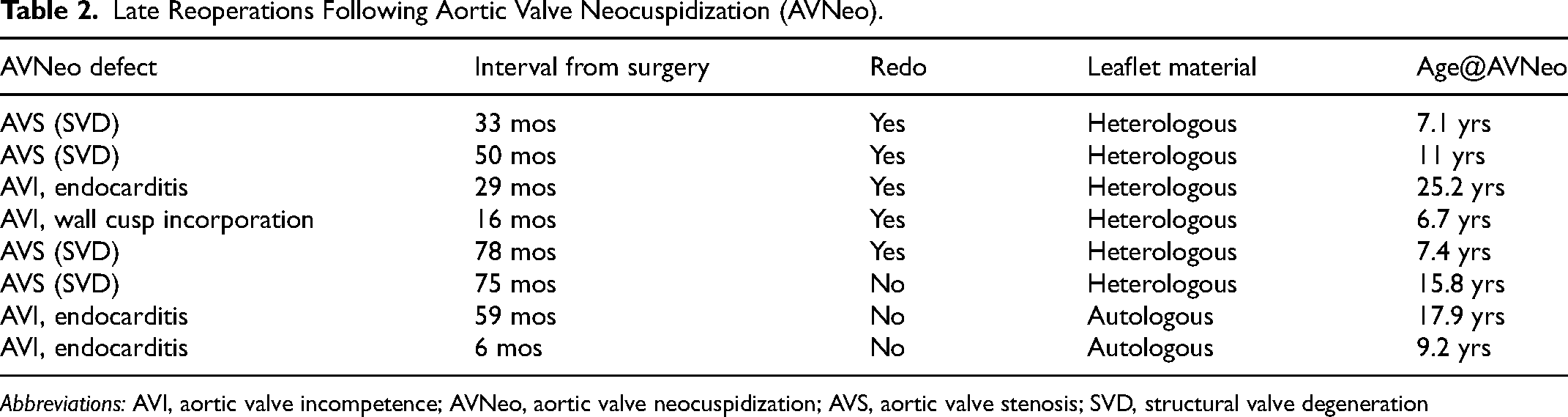
Abbreviations: AVI, aortic valve incompetence; AVNeo, aortic valve neocuspidization; AVS, aortic valve stenosis; SVD, structural valve degeneration
All patients survived. The patient with hypertrophic cardiomyopathy underwent successful heart transplant 4 months after AVNeo replacement.
Data analysis revealed that the AVNeo procedure was more likely to be associated with later reoperation when performed as a redo procedure. In particular, 7 out of 12 (58%) patients undergoing AVNeo as a redo procedure required reoperation later in life, compared with 4 out of 36 (11%) patients who received AVNeo as their first operation (P = .002). Regarding the type of material used for neoleaflet construction, 4/36 (11.1%) patients who received autologous leaflets underwent reoperation, compared with 7/12 (58.3%) who received heterologous pericardial leaflets (P < .001) (Figure 1).
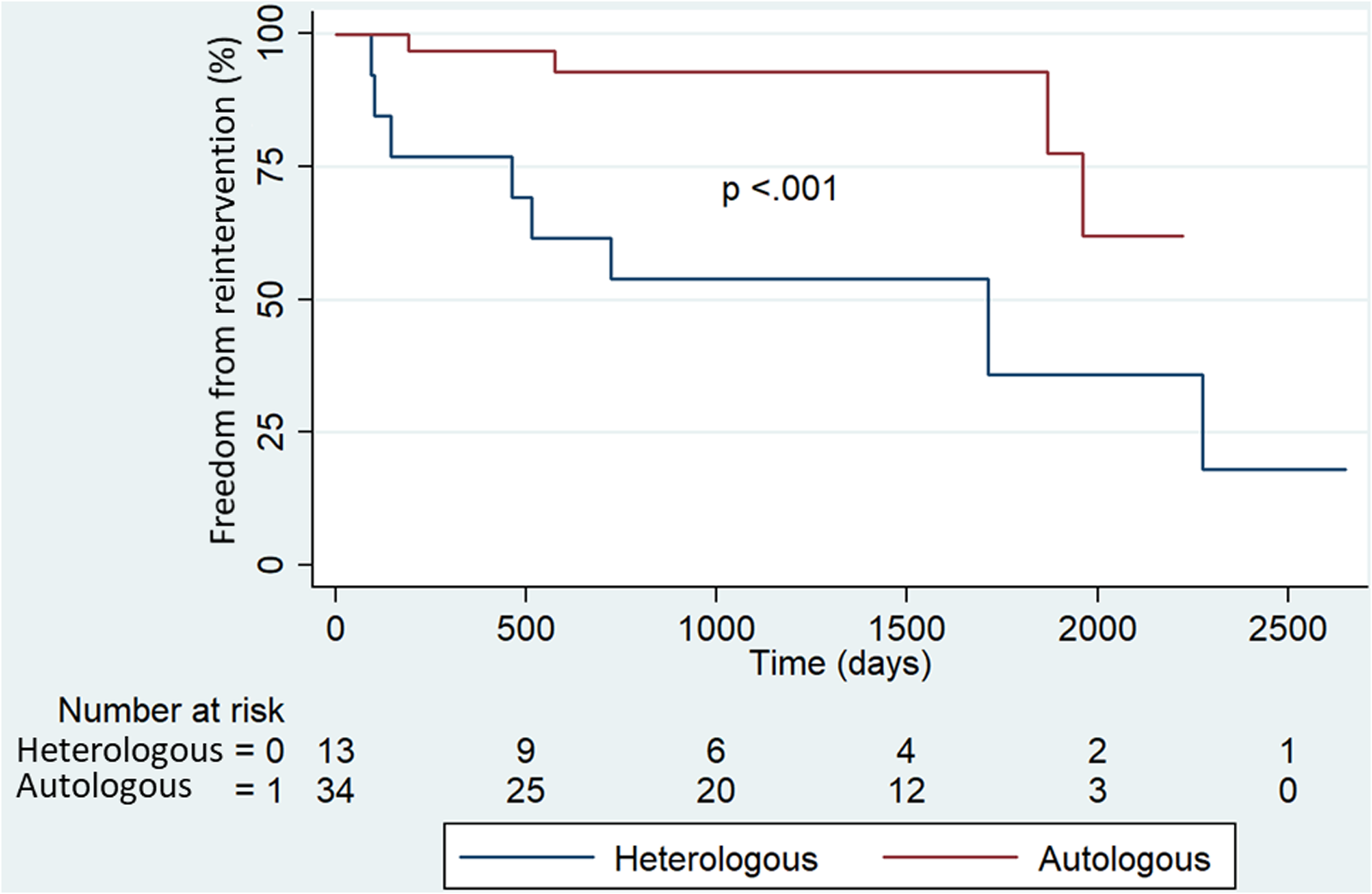
Freedom from reoperation according to the material used for aortic valve neocuspidization.
AVNeo Performance
All 48 patients discharged from the hospital showed good AVNeo function, as evidenced by a median peak gradient of 13.5 (10.6-16.5) mm Hg and a median indexed vena contracta of 1.2 (0-2) mm. At the final follow-up, both median AV peak gradient and IVC values showed a significant increase, reaching 18.7 (11.7-29.7) mm Hg (P = .005) (Figure 2A) and 1.9 (1-3) mm (P = .014) (Figure 2B) respectively. No significant differences were observed based on patients’ age group (Figure 3).
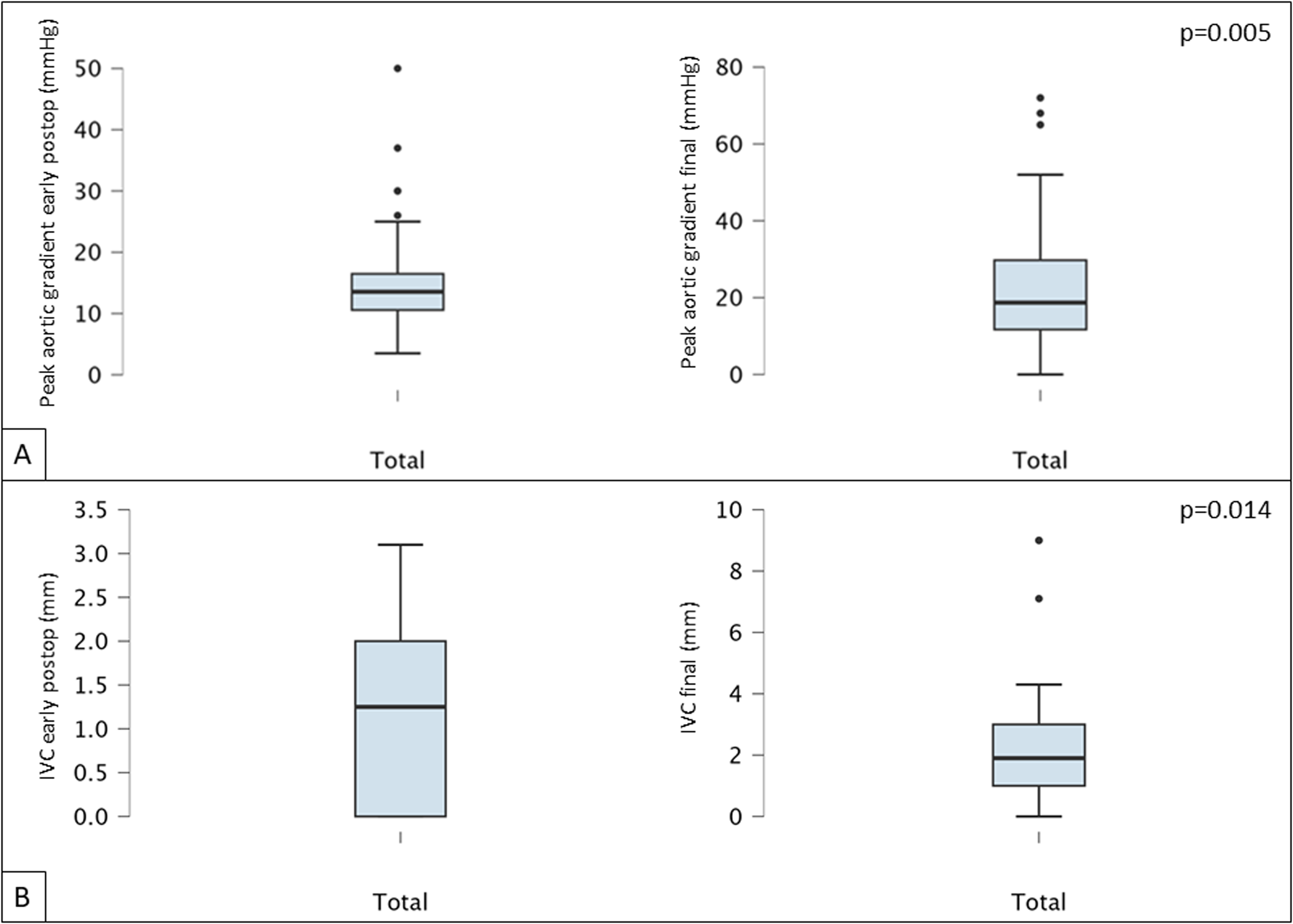
(A) Early postoperative versus final aortic valve peak gradient; (B) early postoperative versus final indexed vena contracta jet width (IVC).
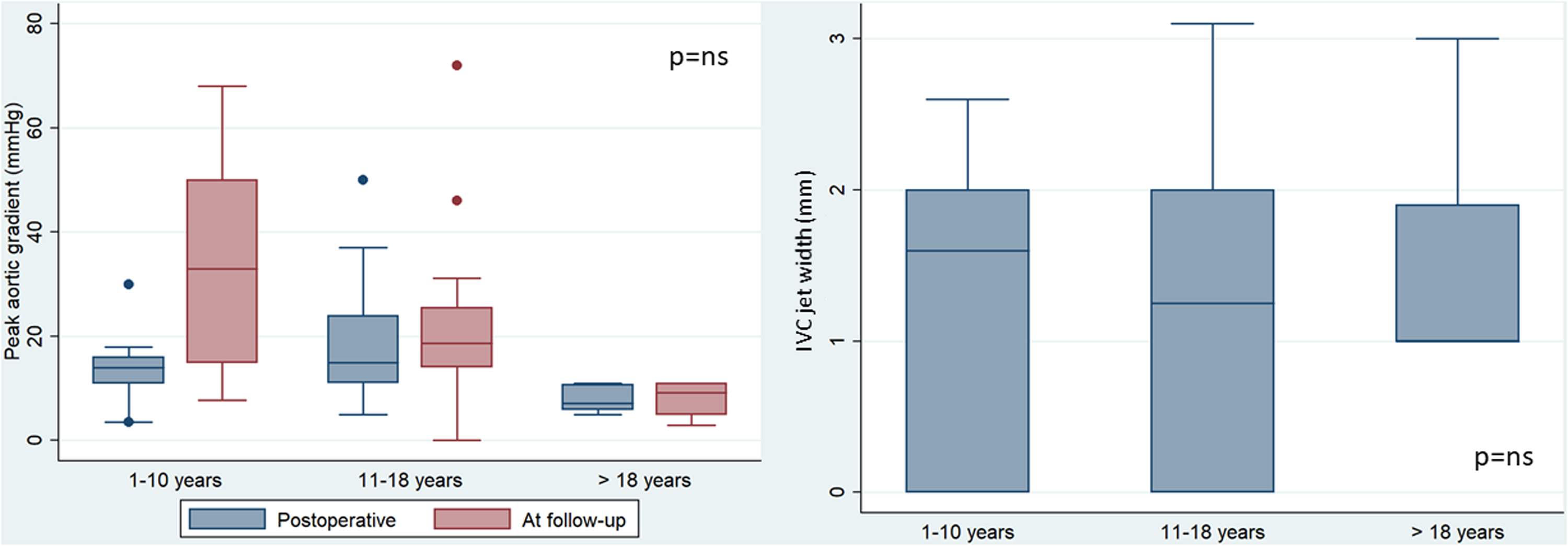
Influence of age group on aortic valve peak gradient and indexed vena contracta (IVC) jet width.
In relation to the initial defect, prevalent AVS was associated with a significantly higher AV peak gradient at follow-up (P = .04). However, no significant difference was found in the IVC between prevalent AVS and prevalent AVI as initial defects. Furthermore, the analysis of the indication for rheumatic versus nonrheumatic etiology did not show any significant difference in terms of outcome measures (redo operation, P = .32, AV peak gradient, P = .34, and IVC, P = .15) between patients with rheumatic disease and the rest of the cohort.
Regarding the type of material used for leaflet construction, autologous pericardium was associated with a significantly better performance compared with heterologous materials. This was reflected in both the peak AV gradient (P = .003) and IVC (P = .006) at follow-up (Figure 4).
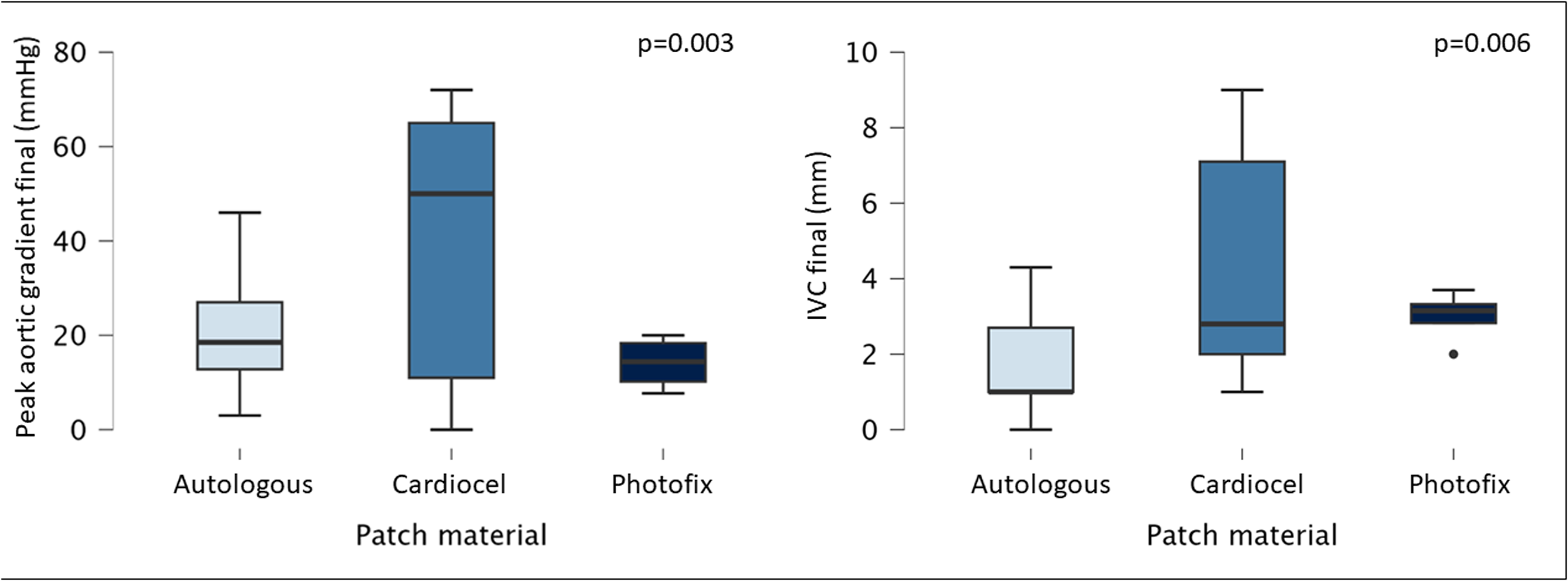
Influence of material used for aortic valve neocuspidization on aortic valve peak gradient and indexed vena contracta jet width (IVC in figure below).
Outcome Analysis
Composite outcome (redo/death) did not show a statistically significant relationship with surgical complexity (P = .28, Figure 5). A significant increase in the AV annulus diameter was observed when comparing early postoperative measurements with those at late follow-up (P < .001) (Figure 6).
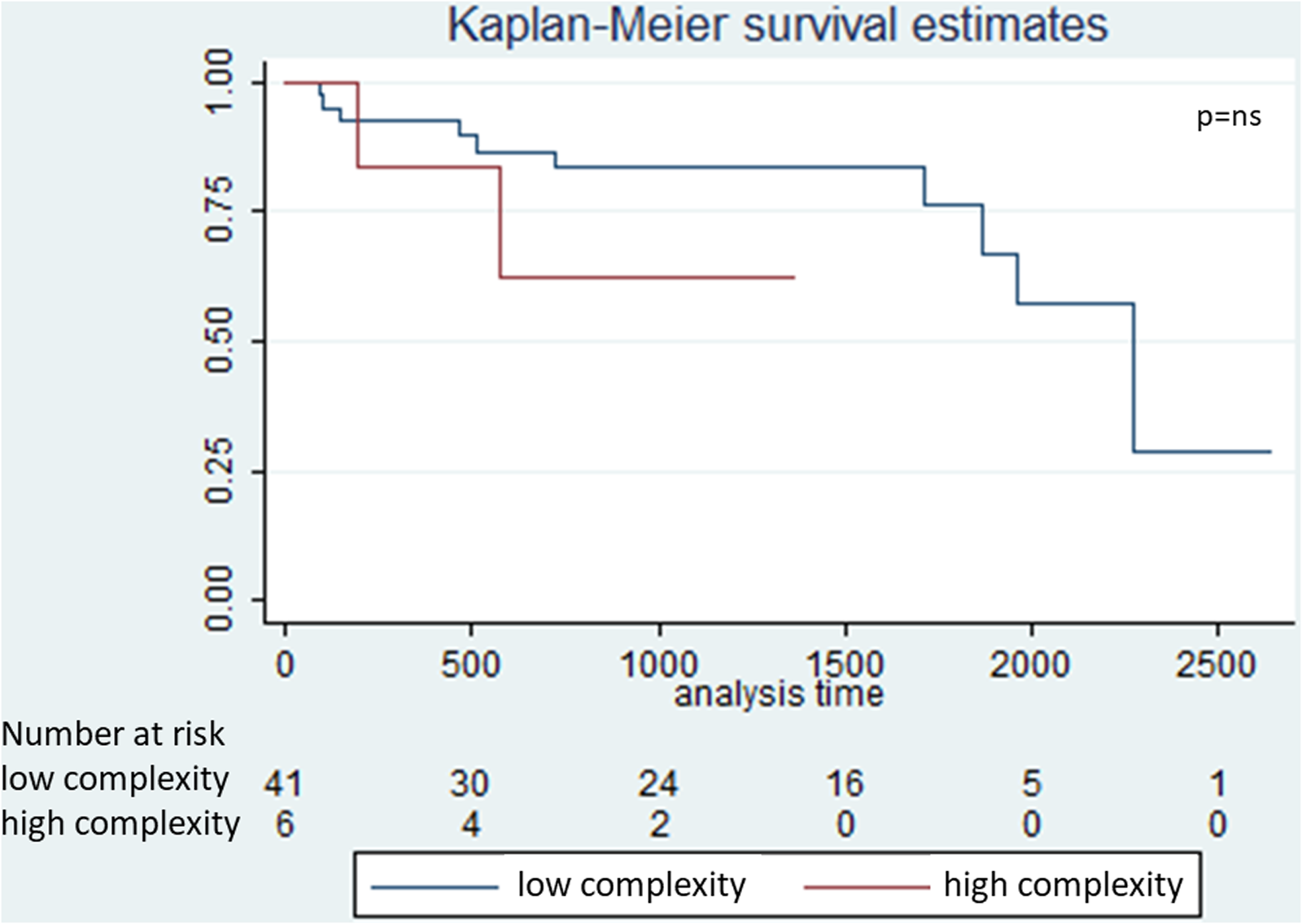
Influence of surgical complexity on composite outcome, redo/death.
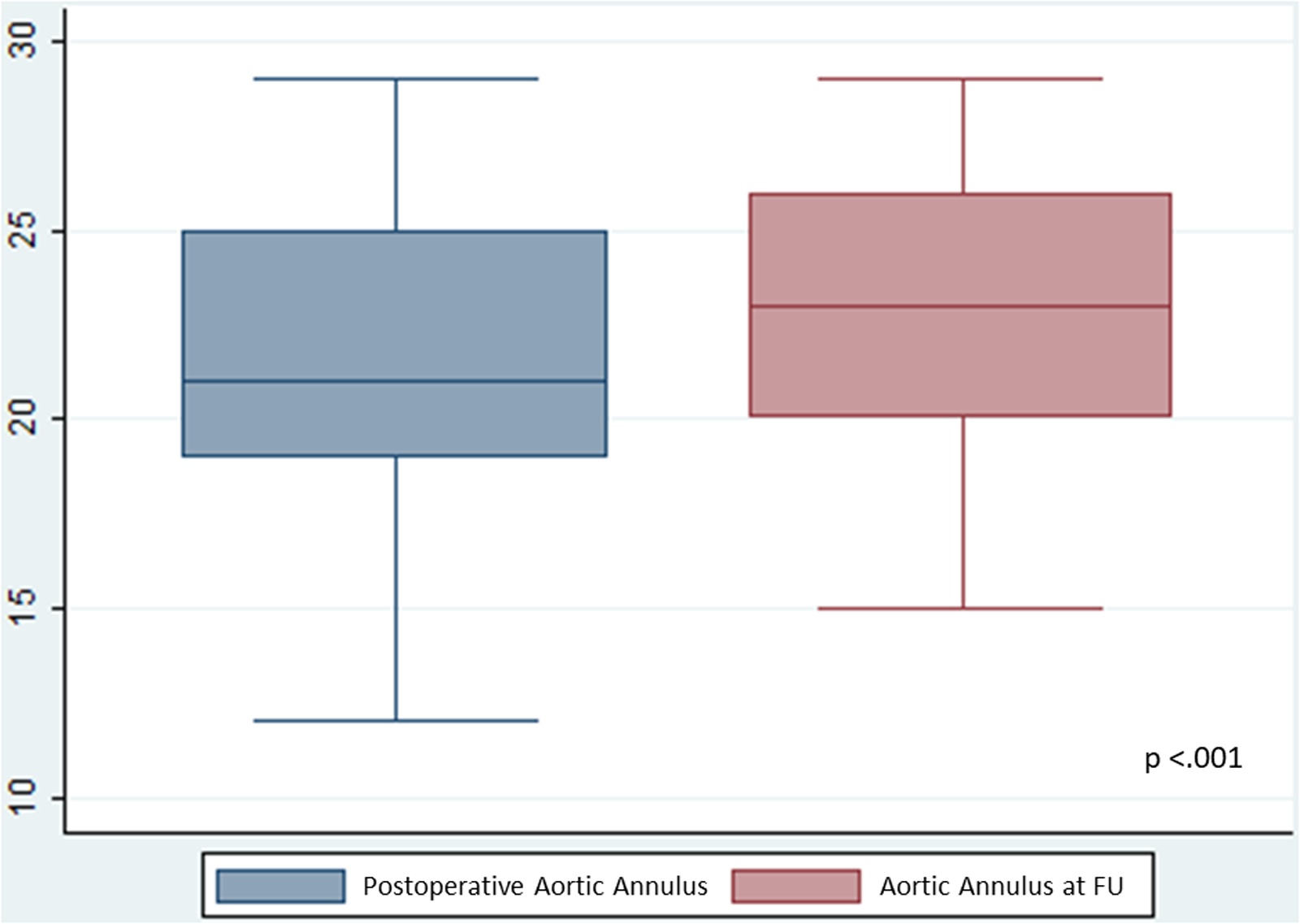
Development of aortic valve annulus at follow-up (FU).
Additionally, a highly significant inverse correlation was found between preoperative AV annular diameter and peak AV gradient at follow-up (P < .001), as well as a significant inverse correlation between preoperative AV annular diameter and IVC at follow-up (P = .022) (Figure 7).
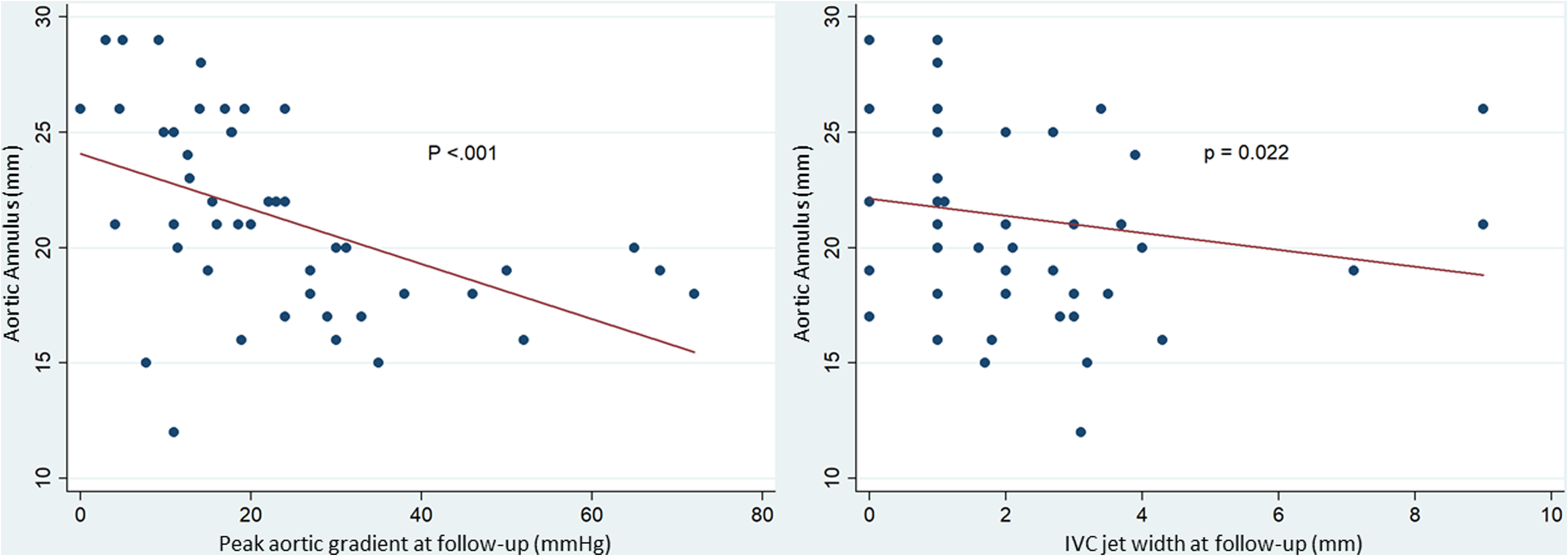
Relationship between aortic valve annular size and neo aortic valve performance (peak aortic valve gradient and indexed vena contracta [IVC] jet width).
Finally, the logistic regression analysis revealed an independent association between AVNeo performed as a reoperation with composite outcome, redo/death (Table 3).
Multivariable Regression Analysis of Clinically Significant Variables Associated With Redo Operation-Death Outcome.
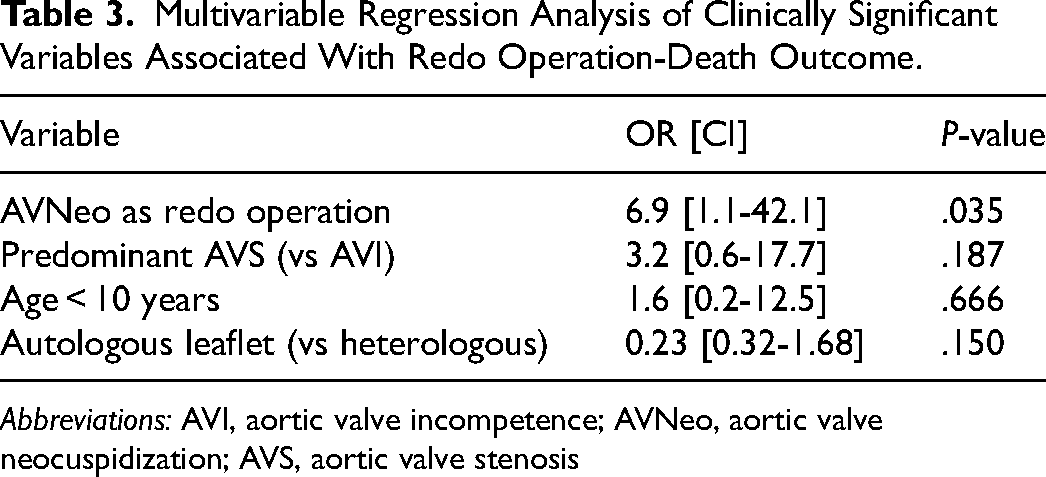
Abbreviations: AVI, aortic valve incompetence; AVNeo, aortic valve neocuspidization; AVS, aortic valve stenosis
Comment
AVNeo, particularly through the Ozaki procedure, represents a promising and innovative surgical approach for managing aortic valve (AV) disease in children, adolescents, and young adults.4–8
Despite its potential advantages, such as minimal invasiveness, reproducibility, and favorable acute hemodynamic outcomes, the technique remains underutilized in many centers worldwide. This is mainly due to the limited number of large patient series with sufficient follow-up. In this context, we believe it is crucial to report the outcomes from a consecutive series of patients operated on in 90% of cases by the same first operator (AC) who, however, was the second operator in the remaining 10% of cases over an 8-year period at a single center, with an in-depth analysis of the variables involved.
When stratifying patients by age groups and analyzing the outcomes, it became evident that AVNeo offers a low-risk treatment for AV disease at all ages, whether the condition is isolated or accompanied by other cardiac lesions of varying severity. The follow-up results of this study demonstrate that AVNeo function is durable, with a low incidence of recurrent stenosis or insufficiency, especially when autologous pericardium is used. Although pericardial substitutes yield excellent early results, they increase the risk of early secondary surgeries, particularly due to structural valve degeneration. This observation is consistent with adult case series, where the use of autologous pericardium was associated with low rates of structural valve degeneration.10,12 All cases of structural valve degeneration reported in our series occurred in patients treated with Cardiocel® and its characteristics were similar to those of pericardial bioprosthesis degeneration. The structural valve deterioration report was provided by the cardiologists of the outpatient service and the indication for reoperation was shared in a joint conference with the surgeons according to the same criteria used for bioprosthesis degeneration, in terms of stenosis, insufficiency or both. Regarding our experience with Photofix®, although apparently positive, it is limited to only 4 cases, mainly due to European Community certification issues which made the product available in Italy for only a short time. We believe that the unfavorable Boston Children's Hospital group's experience with Photofix® used for AVNeo should be taken into deep consideration 17 to underline once again the inadequacy of the heterologous pericardium in this procedure.
The leading cause for reoperation11,12 in adult studies has been endocarditis, with the incidence reported up to 5.5%. 18 Our study demonstrated a similar rate, with 6% of patients (3 out of 48) requiring intervention for endocarditis diagnosed according to the ESC guidelines. 19 This incidence is higher than that reported in large studies of patients with biological prostheses, where endocarditis rates have ranged from 1.3% 20 to 4.4%. 21
This finding underscores the importance of educating patients on preventive measures, particularly regarding lifestyle choices after undergoing AVNeo. In one case from our series, endocarditis was directly linked to dental procedures performed without appropriate antibiotic prophylaxis. Notably, there were no endocarditis-related deaths, and AVNeo dysfunction was successfully managed through homograft aortic root replacement in 2 cases and biological SAVR in one case after adequate antibiotic treatment. Interestingly, AVNeo was performed with heterologous pericardium in one of the patients and autologous pericardium in the other 2, emphasizing that autologous tissue alone does not entirely prevent infectious complications following bacteremia.
Regarding the initial defect, our findings suggest that prevalent AVS is associated with a more significant increase in peak AV gradient at follow-up, while the progression of IVC appears to be unaffected by the type of defect.
Our analysis also did not reveal any significant relationship between the progression of AVNeo dysfunction and patient age groups. However, it is noteworthy that of reinterventions occurred in patients who were 10 years of age or younger (Group I), and 80% of those involved the use of pericardial substitutes. Although heterologous pericardium may contribute to this outcome, the relatively high incidence of reinterventions in this age group should not be overlooked. The highly significant inverse correlation between preoperative AV annular diameter and peak AV gradient at follow-up, as well as the significant inverse correlation between preoperative AV annular diameter and IVC at follow-up, further corroborate these findings, particularly in the pediatric cohort. Interestingly, our data also show a significant growth of the AV annulus, a phenomenon not observed in our earlier experience. 4
A separate mention should be made regarding our AVNeo findings in rheumatic disease, which were not dissimilar to those reported for other causes of AV disease. As already proposed in the literature,22 AVNeo in this particular patient setting could constitute a specific indication, especially due to the inadequacy of the Ross operation in which autograft failure is commonly seen in this clinical context. 23
The complexity of the associated surgical procedures did not significantly impact the composite outcome of redo surgeries or death, although the small number of complex associated procedures in our series may limit the interpretation of this finding. Finally, AVNeo as a reoperation was independently associated with a worse outcome, as demonstrated in our multivariable analysis.
Limitations
This is a single-center retrospective study without a control group. The limited and heterogeneous sample size of patients does not allow drawing statistically meaningful conclusions. The follow-up duration, although reasonable, remains limited, preventing definitive conclusions about the long-term outcomes of AVNeo. While our results refine and adjust our initial findings, extending the follow-up period would likely provide further insights and allow for a more focused analysis of the technique's performance.
Conclusion
The medium-term results of AVNeo are promising, particularly in adolescents and young adults, aligning with the favorable outcomes reported for older adults. However, AVNeo as a reoperation is associated with a worse outcome and should probably be considered exclusively in the absence of effective alternative strategies and only if high-quality autologous pericardium is available in adequate quantity. In pediatric patients, the indication for AVNeo should be carefully considered, ideally when no viable alternative options exist. Moreover, the use of materials other than pretreated autologous pericardium should be avoided whenever possible. Finally, it is crucial that both patients and clinicians remain vigilant about the primary prevention of bacterial endocarditis, particularly in cases of dental procedures or minor surgeries, even when autologous tissue is used for AV implantation.
Footnotes
Acronims and Abbreviations
Author Contribution
All authors contributed to the study conception and design. AP and MC involved in data curation and investigation. SBA and GR did supervision and validation. EC did investigation. VF involved in data collection. AC involved in writing—original draft (and writing—review and editing).
Data Availability
The data underlying this article are available in the article and in its online version.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.