
Abstract
Coronary artery complications following the arterial switch operation (ASO) for transposition of the great arteries have become increasingly relevant as those affected are exposed to the comorbidities of later years. A scoping review was undertaken to explore the incidence, clinical features, and management of the long-term coronary complications after the ASO. The selection criteria yielded 73 articles They recorded few long-term coronary artery complications following the ASO, which were difficult to recognize as most affected patients’ symptoms were absent or nonspecific. In patients with suspected coronary artery involvement, coronary angiography or computed tomography provided confirmation, with significant stenosis generally managed by percutaneous trans-catheter interventions.
Keywords
Introduction
Transposition of the great arteries (TGA) is a common cause of cyanosis in the newborn.1–3 It is a serious congenital abnormality which if left untreated has a significant morbidity and mortality arising from increasing hypoxia as the systemic and pulmonary circulations function side by side in parallel rather than in series. 4 However, if diagnosed in a timely fashion and managed appropriately, the immediate and long-term outlooks are excellent. 5 Many patients in skilled hands are diagnosed prenatally by a morphological scan at 20 to 22 weeks. 6
In Australia, the incidence of TGA is 0.3 to 0.6 per 1,000 live births, accounting for 4% to 5% of all congenital heart disease (CHD). 3 Prenatal diagnosis via detailed fetal echocardiogram has improved over the years,6–8 allowing for planned perinatal care at specialist centers. As part of the immediate management, neonates generally require a balloon atrial septostomy to improve systemic oxygenation. 9 This catheter intervention is followed by an arterial switch operation (ASO) ideally within the first two weeks of life to preempt left ventricular atrophy following the drop in the pulmonary vascular resistance. 10 With major improvements in surgical techniques, the ASO currently has a low operative mortality of 2%. 11 It has excellent long-term outcomes compared with the atrial switch operation 12 as the left ventricle assumes its role as the systemic ventricle. In addition, unlike the atrial diversion procedure, there is less atrial manipulation resulting in fewer atrial arrhythmias. 13
A crucial part of the ASO involves the translocation of the coronary arteries from the previous aortic root to the pulmonary root, which becomes the neoaortic root. The translocation can lead to mechanical kinking, distortion, compression, and scarring of the coronary arteries, which can also be damaged during the surgery. 14 Over the years, surgeons have mastered the technique, with successful outcomes even for those newborns with TGA and intramural coronary arteries. 15 However, later complications of the coronary arteries may develop and include local stenosis and occlusions, still without clear recommendations as their early diagnosis and subsequent management. 16
The medium and long-term complications of the coronary artery translocation in the ASO is less well documented, and become especially important in the light of an increasing population of successfully treated aging patients who are at risk of developing atherosclerotic (atheromatous) cardiovascular disease. 17 This review aims to identify and synthesize the reported findings of the prevalence, clinical presentation, investigations, and management of coronary artery complications following the ASO. It will not comment on other complications of the ASO which include dilation of the aortic root, development of neoaortic valve incompetence, and the now less frequent pulmonary artery stenosis, currently being addressed at the Royal Children's Hospital, Melbourne, which is studying the long-term ASO survivors.
Materials and Methods
A scoping review was undertaken based on the principles of Arksey and O’Malley, 18 and which followed the scoping review checklist of the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). 19 This methodology involved four steps: identifying the research question, systematically searching for relevant studies, screening and selecting studies which met the inclusion criteria, and summarizing their findings. Ethics approval was not deemed necessary as only published data were reviewed.
Research question: What do we know about the medium and long-term coronary artery complications following the ASO for TGA?
Systematic search: A systematic search was done during the months of April and May 2024 using two databases: PubMed/Medline and Embase. All identified studies were transferred to EndNote for analysis.
Selection of studies: Studies were selected by the following inclusion criteria:
Studies that reported patient populations that underwent the ASO for TGA Studies that addressed coronary artery complications such as coronary artery–related lesions including stenosis, occlusions, and/or involved interventions, the development of ischemia, including the morbidity and mortality that occurred 30 days or later following the ASO. Articles for which a full text was not available or not reported in the English language Case reports, commentaries, editorials, and preprints
These exclusion criteria were applied:
The first screening involved removing duplicate articles. Next was scanning the titles and abstracts to see if they fit with the inclusion criteria. Once selected, the article's full text was reviewed, and a summary was extracted and analyzed19 (See Figure. 1).
Data extraction: A data extraction table was set up in an Excel 2010 spreadsheet with the following information included from each study: authors, year of publication, study location, objectives, methodology, participants, and findings. A summary of the findings are included within the body of the paper and in the tables.
Results
The initial search of two databases yielded a total of 205 articles. Duplicate articles were discarded (n = 30). Further articles were excluded after the title and abstract were studied (n = 115). Following review of the references, 13 additional articles were included, resulting in a total of 73 articles to be analyzed (Figure 2). Table S1 provides a summary of the 73 studies—the references, objectives, methods, participants, and results. A summary of the main findings is provided in Table 1.
Summary of Main Findings.
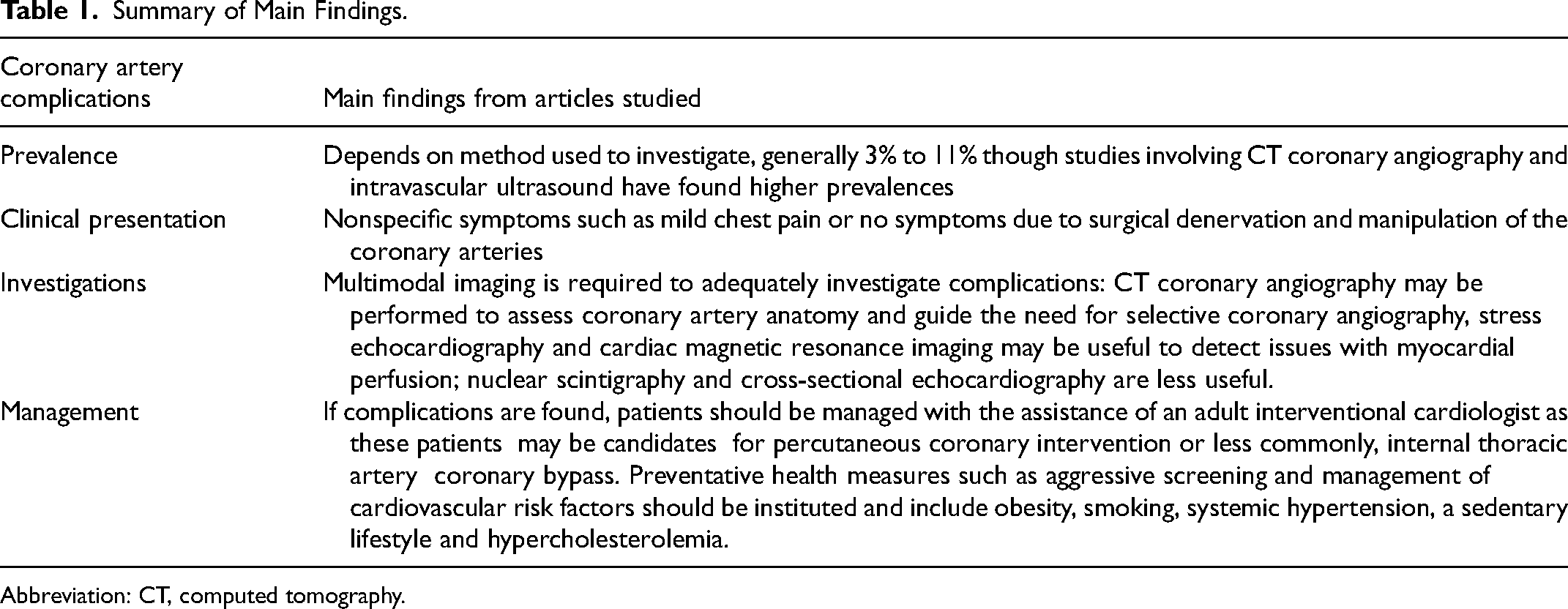
Abbreviation: CT, computed tomography.
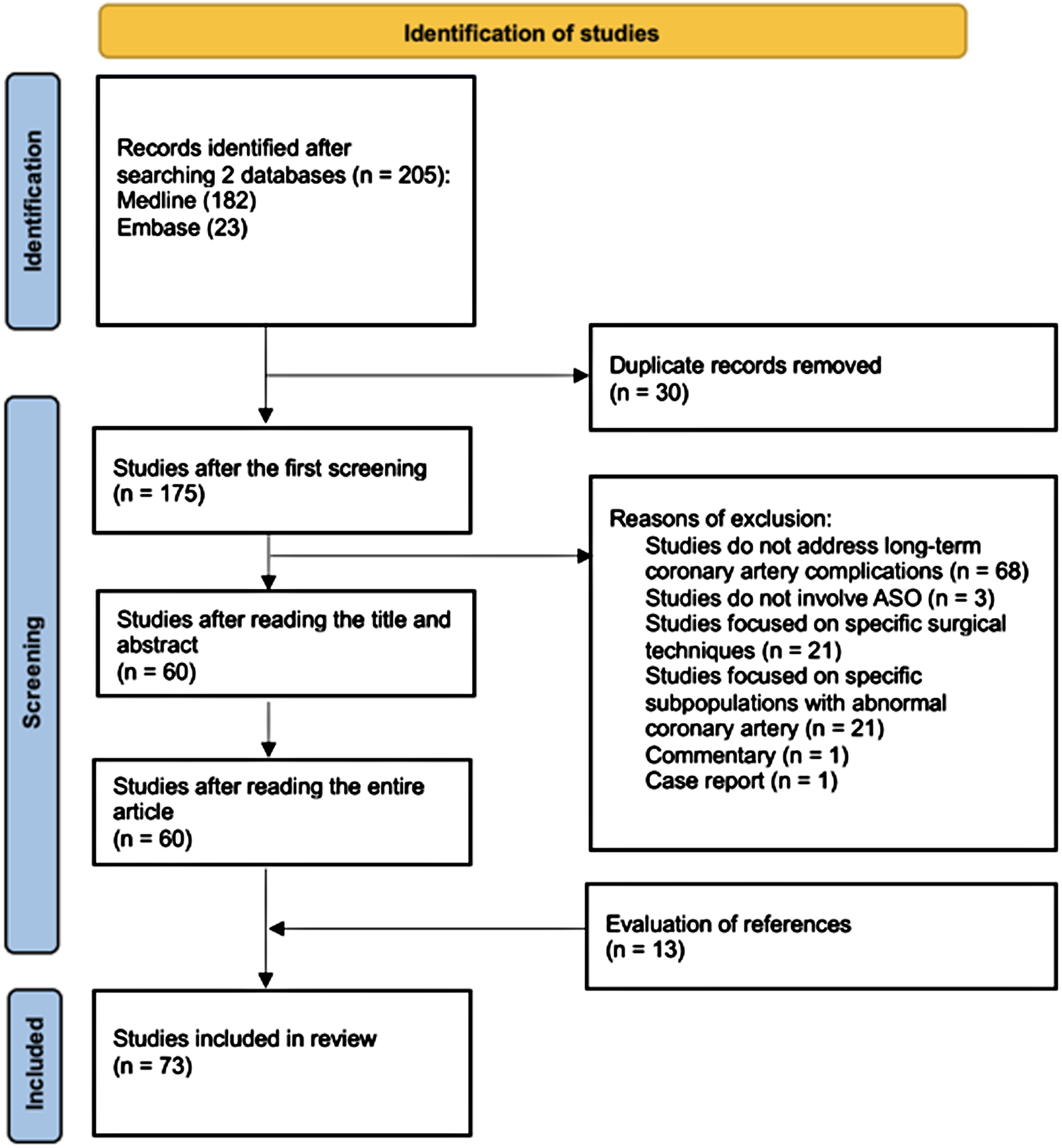
Study flowchart. Adapted from Page et al19.
Medium to Long-Term Coronary Artery Complications
The prevalence of late coronary artery abnormalities in large cohort retrospective studies is found to be between 3% and 11%. 20 This prevalence may be an underestimate as most patients do not routinely undergo diagnostic coronary angiography. Indeed, studies involving cardiac imaging of asymptomatic ASO patients found a much higher prevalence. One study observed that 43% of their patients who underwent coronary angiography had abnormal coronary findings. 21 A further study utilizing intravascular ultrasound noted 89% of their patients had some degree of intimal thickening in at least one major coronary artery. 22 This prevalence was significantly higher when compared with an intravascular ultrasound study of “normal hearts” where significant intimal thickening suggestive of atherosclerosis was found in only 17% of those under 20 years and 37% in those who were 20 to 29 years of age. 23 Additionally, studies comparing adults with CHD which included patients with TGA with those without CHD, have found the former group had a 1.6-fold increased risk of myocardial infarction, 24 and double the risk of comorbidities such as coronary artery disease. 25 These findings are especially important for the adults who have had an ASO as they age, where the shift toward acquired heart disease such as atherosclerotic cardiovascular disease becomes increasingly relevant. 17
Symptoms of Coronary Artery Involvement
Arterial switch operation patients with coronary artery complications often have nonspecific or no symptoms. 26 In part, these observations may be due to surgical denervation of the coronary arteries during their translocation in the ASO. 27 Studies have reported a significant proportion of patients who are asymptomatic but still found to have coronary artery obstruction via computed tomography (CT) or direct coronary angiography. 28 Others have noted patients with mild chest pain during exertion to be indicative of myocardial ischemia. 16 These observations add to the difficulty of diagnosing coronary artery obstruction and ischemic heart disease based on the history, supporting the need for routine coronary artery evaluation.
Investigation of Coronary Artery Complications
Current American and European guidelines for the management of adult patients post ASO-TGA recommend that investigation and management of suspected coronary abnormalities should be symptom driven.29,30 However, symptoms as noted above are often nonspecific or absent. Various imaging modalities are used to investigate coronary artery complications and are summarized in Table 2.
Summary of Investigations for Coronary Artery Complications.
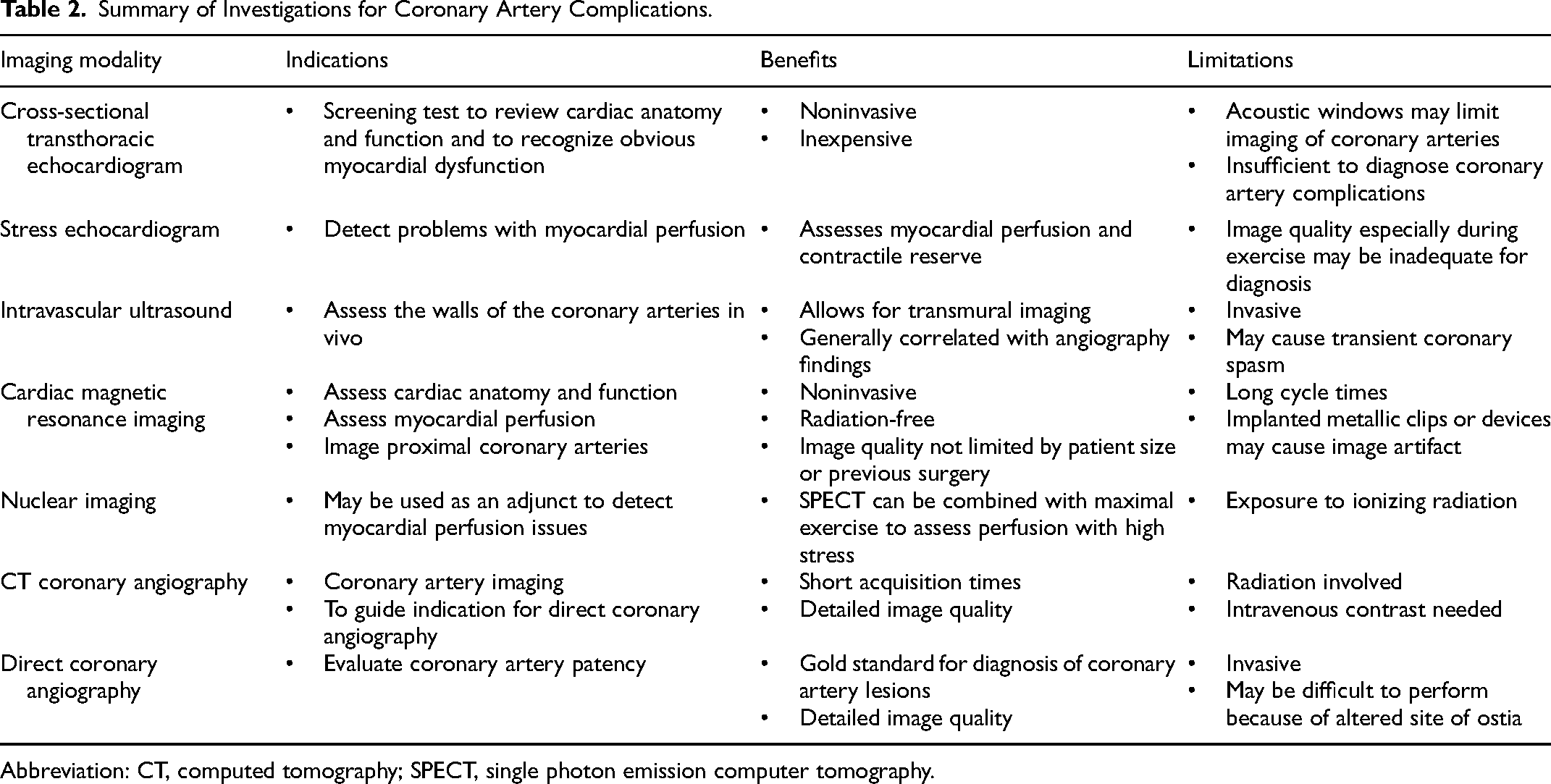
Abbreviation: CT, computed tomography; SPECT, single photon emission computer tomography.
Noninvasive investigations include a simple electrocardiogram (ECG), an exercise stress test, echocardiography extending to a stress echocardiogram, and myocardial nuclear perfusion scans. However, studies have documented that CT coronary angiography (CTCA) or direct coronary angiography yield more accurate results.31,32 Stress echocardiography results were found to concur with stress myocardial perfusion studies; 33 CTCA as well as direct coronary angiography.34,35 Out of the 73 papers reviewed, 50 investigated the prevalence of coronary artery lesions following the ASO and specified the imaging methods used. The majority of these studies utilized CTCA or direct coronary angiography as the confirmatory method of diagnosis. A third of these studies involved a combination of imaging methods. Very few studies utilized nuclear scintigraphy, cardiac magnetic resonance imaging, and/or coronary intravascular ultrasound as their only method of investigation. The overall consensus from these studies suggested echocardiograms and/or myocardial perfusion studies as routine investigations for coronary artery involvement followed by CTCA and/or direct coronary angiography in select patients as the gold diagnostic standard. 36 However, further study is required to provide clear guidelines as to which patients require coronary angiography. That is in addition to determining what tests should be done routinely as well as their timing in a generally asymptomatic population.
Management of Coronary Artery Complications
Coronary artery interventions
The input of an adult coronary interventional cardiologist is generally required in the management of medium to long-term coronary artery complications following the ASO. They have the experience in understanding the anatomy of the coronary arteries, the significance of any abnormality, and the outcome of the various revascularization procedures available. 26 Angiography will determine the severity of coronary artery stenosis and the presence or absence of collateral blood flow to determine if coronary intervention is necessary.28,37 Percutaneous coronary interventions can be performed in most cases with good results of up to 95% reduction in the degree of stenosis five years after intervention. 14 Coronary artery bypass surgery may occasionally be necessary in 2% to 9% of patients.38,39 In general overall, freedom from coronary artery intervention at 20 years after the ASO ranges from 75% to 99%, depending on the reporting center.5,40–42
Cardiovascular risk factors
The development of atherosclerotic cardiovascular disease increases with the increasing age of the ASO survivors. It is recommended that this at-risk population undergo more intense screening and management of modifiable cardiovascular risk factors, including diet, physical activity, tobacco smoking, hypertension, obesity, and dyslipidemia. 43 In particular, proactive prevention of the dyslipidemic atherogenic triad of elevated triglycerides, low high-density lipoprotein cholesterol, and high low-density lipoprotein cholesterol can help prevent the development and/or reduce the risk of atherosclerotic cardiovascular disease. 44 Should a statin be prescribed routinely for all ASO patients remains unclear.
Comment
This study used a structured scoping review methodology to ensure a systematic search of the literature. It involved the analysis of a large number of relevant articles with results from the first successful ASO in 1975 to the present. It attempted to synthesize emerging evidence pertaining to an evolving and now aging population of adult ASO-TGA survivors.
Limitations include a lack of randomized control studies involving TGA patients following ASO due to their relatively small numbers, further burdened by ethical considerations. 45 There is also limited research on the long-term outcomes of the ASO for TGA beyond 20 years as the numbers to date are few but continue to grow. 46
Our Current Practice
With the absence of clear guidelines, our patients, if well, have yearly clinical reviews with a routine ECG, an echocardiogram together with seeking out and managing cardiovascular risk factors such as obesity, hypertension, and hypercholesterolemia. Any suggestion of possible ischemic symptoms including nonspecific chest pain warrant a stress echocardiogram and/or exercise stress test, generally followed by a CTCA. If the latter shows any abnormalities, the advice of an adult interventional cardiologist is obtained to determine the need for percutaneous and/or surgical coronary artery intervention. Once ischemia develops, our approach to revascularization is in line with international guidelines for the management of atherosclerotic cardiovascular disease, which recommends coronary revascularization in the presence of significant ischemia. Treatment decisions are patient centered, with an individualized approach that considers features such as collateralization or absence of ischemia and patient preferences and goals.
Suggested Future Research
Further study remains paramount to decide what investigations are required, whether routinely or following the development of symptoms so as to guide the need for more invasive investigations such as a CTCA and/or selective coronary angiography. In addition should such affected patients be treated differently from the general adult population who develop coronary artery disease, and should there be a lower threshold for interventions and/or medication such as a statin and antihypertensive treatment? The answers to these questions will further aid the long-term management of our patients.
Conclusions
Medium to long-term coronary artery complications following the ASO for TGA may have significant health implications for the aging TGA population. This review found that such complications are infrequent, and difficult to diagnose clinically as many of the patients have nonspecific or no symptoms. A plethora of investigations are available but with limited guidelines as to what is best and whether one or more should be done routinely or in selected patients. The results of any interventions are also limited as the numbers affected are small. In addition, the full impact of atherosclerosis with increasing age of this at-risk population still needs to be determined—a study in progress.
Supplemental Material
sj-docx-1-pch-10.1177_21501351241311280 - Supplemental material for Long-Term Coronary Artery Complications Following the Arterial Switch Operation for Transposition of the Great Arteries—A Scoping Review
Supplemental material, sj-docx-1-pch-10.1177_21501351241311280 for Long-Term Coronary Artery Complications Following the Arterial Switch Operation for Transposition of the Great Arteries—A Scoping Review by Rachel S. Lim, Jeffrey Lefkovits and Samuel Menahem in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Abbreviations
Acknowledgments
Ms Poh Chua, librarian at the Royal Children's Hospital, Melbourne, assisted in the search strategy.
Authors’ Statement
RSL researched and summarized the studies arising from this review. She wrote up the first draft of this paper, addressed any issues arising from discussion between the authors, and revised this paper accordingly. JL reviewed the manuscript and made pertinent comments related to the investigations and management of coronary artery complications in the adult population, a major component of his practice. SM conceived the study and guided its development, design, and progress. He critically reviewed the multiple drafts and helped prepare the final submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.