
Abstract
There are fewer than 100 reported cases of congenital left main coronary artery atresia. In this report, we present an adolescent male presenting with exertional syncope in the setting of this rare coronary defect, and review important diagnostic and therapeutic considerations imperative to obtain a favorable outcome.
Introduction
Coronary artery anomalies have an incidence of 1.3% in the general population and are often discovered incidentally. 1 Potentially serious coronary anomalies are further postulated to have an incidence of 0.26%. 1 Congenital left main coronary artery atresia (CLMCAA) represents an extremely rare coronary anomaly, with fewer than 100 cases reported in the literature. 2 Associated cardiac anomalies in the pediatric population have been noted in 44% of cases, most commonly consisting of mitral valve prolapse and supravalvular aortic stenosis. 2 In this report, we present the case of an adolescent male diagnosed with CLMCAA and review important diagnostic and surgical considerations.
Case Presentation
A 13-year-old male with a history of attention deficit hyperactivity disorder and obesity presented with syncope. Prior to the episode, he had gone to the gym for the first time to lift weights, during which he complained of chest tightness. He later went swimming where he again noticed nausea and chest tightness. Upon getting out of the pool, he experienced dizziness and nausea and proceeded to have syncope. Bystander cardiopulmonary resuscitation was initiated, and he awoke after approximately 2 min. On presentation, he was afebrile with a temperature of 97.9 °F, blood pressure 110/49 mmHg, heart rate 66 bpm, respirations 17, SPO2 95%. He appeared fatigued. Cardiovascular examination revealed a normal rate, regular rhythm, normal S1 and S2, no murmurs or gallops. Lungs were clear to auscultation with unlabored breathing. Initial labs revealed AST 406 (ref. 10-40 U/L), ALT 203 (ref. 3-36 U/L), Troponin-I of 64, later peaking at 199 (ref. <57 ng/L), CK 13,480 (ref. 65-225 U/L), and lactate 2.4 (ref. 0.5-2.2 mmol/L). Electrocardiogram revealed normal sinus rhythm without evidence of left ventricular hypertrophy and without depolarization or repolarization abnormalities. Transthoracic echocardiogram was performed and showed normal left and right ventricular size and function without regional wall motion abnormalities. The right coronary artery was dilated with a normal origin. The left main coronary artery structures were not well visualized, raising concern for an anomalous left coronary artery from the pulmonary artery (Figure 1).
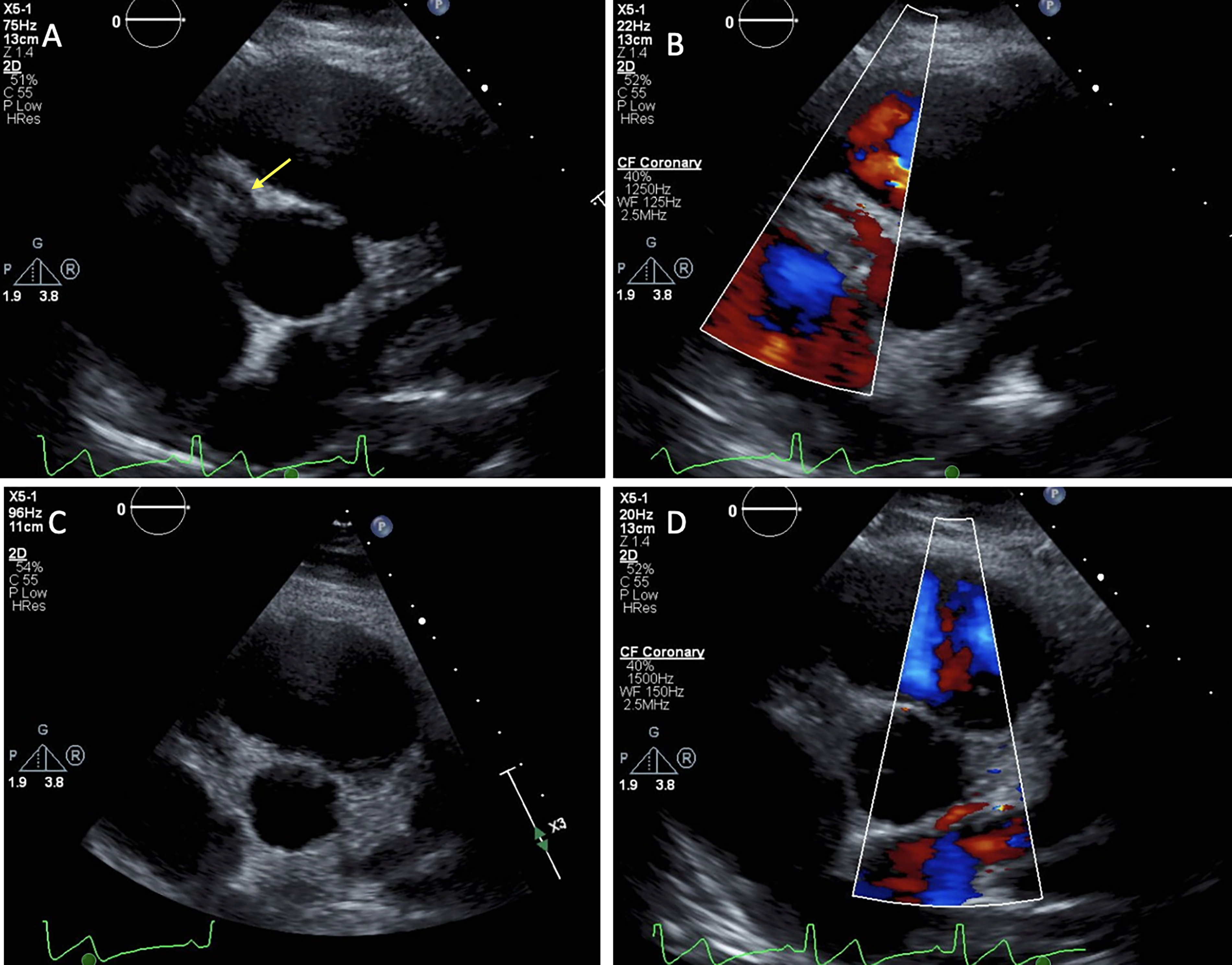
Echocardiogram. (A) The RCA is dilated and arises normally off of the right coronary cusp (Arrow). (B) Color flow Doppler demonstrates antegrade flow through the RCA. (C-D) No clear origin of the LCA is visualized by either 2D imaging or color flow Doppler. Abbreviations: LCA, left coronary artery; RCA, right coronary artery.
Given concern for an anomalous left coronary artery, cardiac computed tomographic angiography was obtained revealing absence of the proximal left main coronary artery. The left circumflex and left anterior descending coronary arteries opacified in the left atrioventricular groove. The right coronary artery arose from the right coronary cusp and appeared mildly enlarged, giving off an atypically large branch that coursed over the anterior right ventricular epicardial surface and then inferiorly at the inferior aspect of the right ventricle. It was unclear how the distal left coronary vasculature was receiving flow (Figure 2). Given suspected absence of the left main coronary artery, cardiac magnetic resonance imaging (MRI) was obtained to assess for myocardial scar. Overall there was normal left ventricular systolic function without segmental wall motion abnormalities. There was no evidence of delayed gadolinium enhancement or of subendocardial enhancement. The patient was referred for right and left heart catheterization to further define coronary anatomy and filling pressures. This confirmed CLMCAA at the ostium with prominent collateral connections from the dilated right coronary artery to the left coronary artery distribution. There was otherwise normal cardiac output and ventricular function (Figure 3).
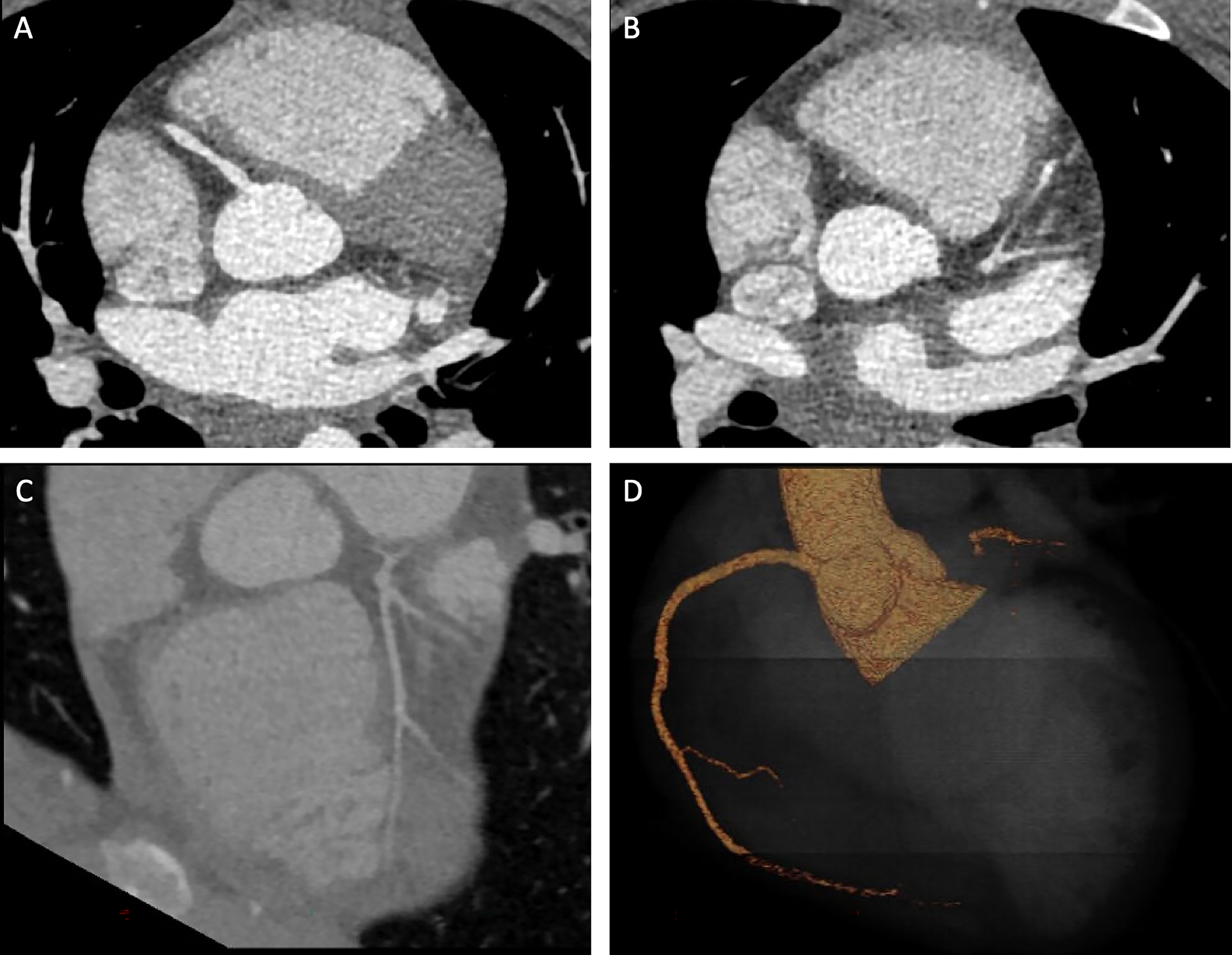
Coronary CT. (A) The right coronary artery arises from the right coronary cusp. (B-D) There is long-segment atresia of the left main coronary artery. The left circumflex and left anterior descending coronary arteries opacify in the left atrial ventricular groove. Abbreviation: CT, computed tomography.
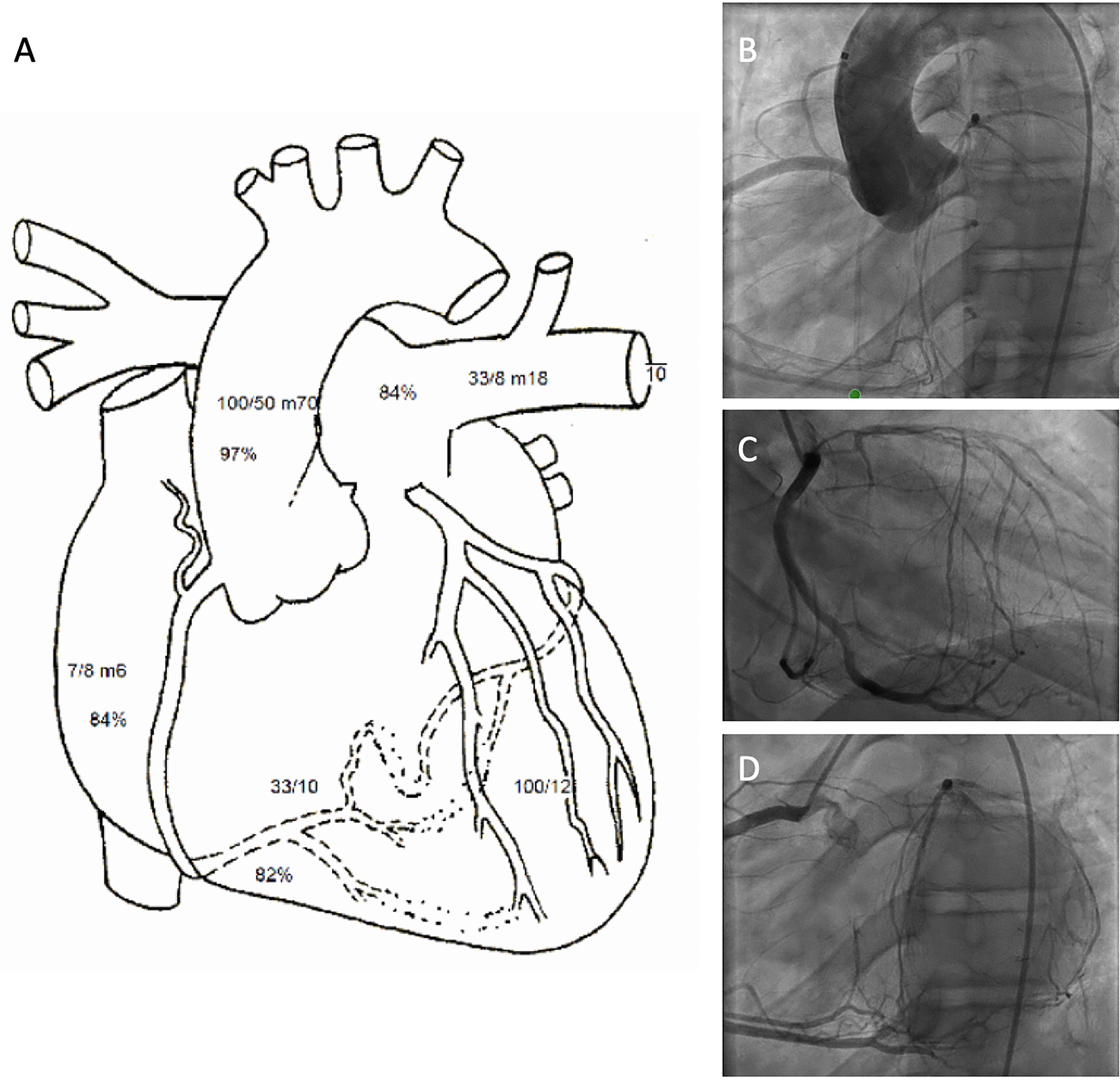
Cardiac catheterization. (A) Right heart catheterization exhibiting normal filling pressures and cardiac output. (B) Aortogram taken at LAO 30, CAU 0 projection exhibiting normal origin of the RCA and congenital left coronary ostial atresia. (C) Selective angiogram of the RCA in RAO 30, CRA 0 and (D) LAO 30, CAU 0 projections revealing a dilated RCA with prominent collateral connections to the LCA distribution. Abbreviations: CAU, cranial angulation; LAO, left anterior oblique; LCA, left coronary artery; RAO, right anterior oblique; RCA, right coronary artery.
After multidisciplinary review, it was felt that the patient’s exertional chest pain represented true angina, and there was high concern his syncope may have been a result of ischemic ventricular tachycardia. Given his high-risk clinical features, a revascularization strategy was recommended. Further review among the Heart Team included discussion regarding coronary reconstruction osteoplasty versus coronary artery bypass grafting. Given the long-segment atresia of the left main coronary segment, the decision was made to proceed with coronary artery bypass grafting using the left internal mammary artery to the left anterior descending coronary artery. There were no postoperative complications, and the patient was discharged home on postoperative day 6. His medical regimen included aspirin, atorvastatin, furosemide, and metoprolol succinate. At his two-month follow-up, the patient was doing well, without cardiopulmonary symptoms.
Discussion
The etiology of CLMCAA is poorly understood; however, it is postulated to be due to one of five causes occurring during embryogenesis: absence of a coronary precursor, displacement of a coronary precursor, failure of the left coronary to canalize, fibrotic changes in the aortic media involving the left coronary ostium, or coronary obstruction by infection or thrombosis. 3 Previously described as a subtype of a single coronary artery, it is now recognized as a distinct entity in that the left anterior descending coronary artery and the left circumflex coronary artery are situated normally in the absence of a left coronary artery ostium and are filled via the right coronary artery through collaterals. 3 The clinical manifestations of this entity are variable and are often related to the degree of collateralization, with symptoms ranging from ischemic heart failure in infants to ischemic heart disease, syncope, and sudden cardiac death in adolescence and adulthood. 4
While best identified by cardiac computed tomographic angiography or coronary angiography, 4 the use of echocardiogram was critical for the present case. Within the pediatric population, echocardiography is often the first imaging modality obtained in evaluating for coronary artery anomalies. Benefits of this modality include its risk-free nature, excellent temporal and spatial resolution, and widespread availability while avoiding deep sedation or anesthesia as is often required in this population for cardiac catheterization or other advanced imaging. 5 Given the ease and safety of the echocardiographic evaluation, it is recommended to assess the coronary origins as part of the complete pediatric transthoracic echocardiogram. 5 In this case, the inability to visualize the left coronary ostium prompted further work-up with advanced imaging and ultimately cardiac catheterization to confirm the diagnosis.
The management strategy of this patient involved a multidisciplinary discussion among the adult and pediatric cardiology teams as well as the adult and congenital heart surgeons. Given the absence of regional wall motion abnormalities, myocardial scar, or subendocardial ischemia on MRI, a conservative strategy involving myocardial perfusion imaging was considered in order to avoid coronary artery bypass grafting. This treatment strategy has proven safe and effective previously for a different case. 6 However, in that other case, the chest pain was felt to be noncardiac in nature, and the patient had no symptoms of dyspnea, palpitations, syncope, or presyncope. For our patient, given the otherwise high-risk clinical features, it was felt that a “normal” myocardial perfusion study would not rule out balanced ischemia given the large territory involved; thus revascularization was believed to be the most beneficial treatment strategy.
The treatment of this lesion is surgical and the goal is to restore sufficient myocardial perfusion to the left-sided system. Surgical indications include symptomatic patients, ischemic changes on electrocardiogram or stress testing, left ventricular systolic dysfunction, severe mitral regurgitation, or small-sized collaterals. 2 Without surgical revascularization, myocardial demand progressively overwhelms the collateral circulation, leading to ischemic heart disease.2,5 In the most recent review, 85% of pediatric patients underwent surgical revascularization, with the surgical approach consisting predominantly of coronary artery bypass grafting (71%), with a smaller number of patients undergoing coronary reconstruction osteoplasty (29%). 2 Surgical outcomes were favorable, with 81% survival; however, medical management portended a poor prognosis, with a 43% mortality rate. From a surgical perspective, coronary reconstruction osteoplasty has been hypothesized to offer the benefit of restoring physiologic flow, avoiding the inherent retrograde perfusion required of a graft anastomosis. 2 Additionally, coronary reconstruction osteoplasty may provide more feasible anatomy for future percutaneous coronary intervention and further preserves the left internal mammary artery if coronary artery bypass grafting is needed for traditional atherosclerotic disease in the future. 2 For the present case, coronary reconstruction osteoplasty was not feasible due to a very underdeveloped left main coronary trunk with long-segment atresia, thus necessitating coronary artery bypass grafting. Alternatively, primary percutaneous coronary intervention for CLMCAA has been described in a single case through a retrograde approach. 7 Regardless of the treatment approach, the natural history of CLMCAA following revascularization is not well-understood, necessitating the importance of long-term follow-up.
Conclusions
Congenital left main coronary artery atresia represents a rare coronary anomaly and important cause of ischemic heart disease. Transthoracic echocardiogram is an essential part of the initial evaluation in the assessment of coronary anomalies in the pediatric population. Early surgical revascularization either by coronary reconstruction osteoplasty or coronary artery bypass grafting (if there is long-segment atresia) should be strongly considered in symptomatic patients, those with ischemic changes on electrocardiogram or stress testing, left ventricular systolic dysfunction, severe mitral regurgitation, or small-sized collaterals to prevent development and/or progression of ischemic heart disease and sudden cardiac death.
Footnotes
Authors’ Statement
Each of the patients in this case series and/or their parents were fully informed and gave written consent for publication of this report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Standards
The authors confirm consent for publication was granted by the patient and their respective parent(s) or guardian. The authors confirm they are in compliance with national and institutional ethical standards set forth by the University of North Carolina at Chapel Hill.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.