
Abstract
Objective
Primary repair in the first six months of life is routine for tetralogy of Fallot, complete atrioventricular septal defect, and ventricular septal defect in high-income countries. The objective of this analysis was to understand the utilization and outcomes of palliative and reparative procedures in high versus middle-income countries.
Methods
The World Database of Pediatric and Congenital Heart Surgery identified patients who underwent surgery for: tetralogy of Fallot, complete atrioventricular septal defect, and ventricular septal defect. Patients were categorized as undergoing primary repair, repair after prior palliation, or palliation only. Country economic status was categorized as lower middle, upper middle, and high, defined by the World Bank. Multiple logistic regression models were utilized to identify independent predictors of hospital mortality.
Results
Economic categories included high (n = 571, 5.3%), upper middle (n = 5,342, 50%), and lower middle (n = 4,793, 49.7%). The proportion of patients and median age with primary repair were: tetralogy of Fallot, 88.6%, 17.7 months; complete atrioventricular septal defect, 83.4%, 7.7 months; and ventricular septal defect, 97.1%, ten months. Age at repair was younger in high income countries (P < .0001). Overall mortality after repair was lowest in high income countries. Risk factors for hospital mortality included prematurity, genetic syndromes, and urgent or emergent operations (all P < .05).
Conclusions
Primary repair was selected in >90% of patients, but definitive repair was delayed in lower and upper middle income countries compared with high-income countries. Repair after prior palliation versus primary repair was not a risk factor for hospital mortality. Initial palliation continues to have a small but important role in the management of these three specific congenital heart defects.
Introduction
According to the World Health Organization, noncommunicable diseases account for 17 million premature deaths globally, with 82% occurring in low- and middle-income countries and 37% due to cardiovascular disease. 1 The impact of congenital heart disease (CHD) on these grim statistics is less well defined. Certain lower income countries have seen a dramatic increase in not only the overall birth rate but also increases in the number of children born with CHD.2–4 In higher income countries, primary repair (PR) in the first six months of life is routine for tetralogy of Fallot (TOF), complete atrioventricular septal defect (CAVSD), and ventricular septal defects (VSD). In lower income countries, socioeconomic and geographic constraints may prohibit timely diagnosis and early intervention for these defects leading to later presentation and potentially higher preoperative illness severity. 5 This can obviate the possibility for PR for these diagnoses and lead to palliation with a shunt or pulmonary artery band (PAB) as the initial approach. In higher income countries, the outcomes for low to moderate complexity procedures have continued to improve over recent decades and associated mortality is now as low as 1% to 2%.6,7 This contrasts with lower income countries where these same procedures have reported mortality up to 6%.8–10 Initial palliation likely still has applicability in these high-risk patients in the developing world.
The World Database for Pediatric and Congenital Heart Surgery (WDPCHS) began accepting and tracking heart operations on January 1, 2017. In doing so, it became one of the first global platforms for the exchange of experience and knowledge for children with CHD. Since the WDPCHS began accepting surgical cases, almost 38,000 procedures from 39 participating centers across 22 countries have been collected with many of the submissions coming from Chinese and Indian congenital heart surgery programs. 11 In the current study, the WDPCHS has been utilized to analyze and compare the overall hospital mortality for patients with TOF, CAVSD, and VSD who underwent definitive or palliative repair between lower middle, upper middle, and high-income countries. We aimed to assess differential mortality between the lower middle, upper middle, and high-income countries for infants and children undergoing surgery for these three specific congenital heart defects, both as a composite cohort and for specific cardiac operations. We hypothesized that lower middle-income countries are more likely to utilize two-stage repair of common malformations with likely worse outcomes than developed countries.
Material and Methods
The WDPCHS is a global registry under the auspices of the World Society for Pediatric and Congenital Heart Surgery. Participating centers are asked to submit all pediatric cardiac surgical cases into the database, which collects information on preoperative demographics, diagnosis, risk factors, and surgical procedures. Complications and mortality during the hospitalization (up to 90 days) are submitted for specified operations. The database content is modeled after the Society of Thoracic Surgeons Congenital Heart Surgery Database. Data are collected through a web-based data entry system and are housed in a secure server environment managed by Kirklin Solutions, Inc., the Data Center for the WDPCHS.
The WDPCHS was utilized to identify patients who underwent palliative and definitive operations for: TOF, CAVSD, and VSD from January 1, 2017, to January 1, 2022. Patients were categorized as undergoing PR, repair after prior palliation (RPP), or palliation only (PO) during the timeframe of the data collection. The country's economic status was categorized as lower middle, upper middle, and high, as defined by the World Bank (Gross National Income [GNI] per Capita). The World Bank classifies low-income economies as those with a GNI per capita, calculated using the World Bank Atlas method, of $1085 or less in 2021; lower middle-income economies are those with a GNI per capita between $1086 and $4255; upper middle-income economies are those with a GNI per capita between $4256 and $13,205; high-income economies are those with a GNI per capita of $13,205 or more (datahelpdesk.worldbank.org). Centers that submitted procedures were separated into high-income, upper middle-income, and lower middle-income groups by the GNI per capita categorization. Currently, there are no low-income countries that submit data to the database. Information collected on specific procedures included demographic characteristics, premature birth, age at time of surgery, noncardiac congenital abnormalities, genetic abnormalities, syndromes, complications, and hospital mortality via prepopulated data entry forms. Terms and definitions for a specific congenital heart defect were defined by the International Pediatric and Congenital Cardiac Code. Procedures, preoperative risk factors, and syndrome are defined in appendices found on the WDPCHS website (www.uab.edu/medicine/wdps/). Mortality was defined as a death following the primary operation during the same hospitalization or within 90 days of operation if still an inpatient. Any procedure with greater than 15% missingness was excluded. Individuals with ages <216 months (<18 years) were included in the analysis. Individual patient consent was waived if approved by individual centers.
Continuous data were presented as mean (± standard deviation) or median (interquartile range) where appropriate. Categorical data were presented as frequency (percent). Comparisons were evaluated using Student t test for continuous variables or Wilcoxon Rank Sum. Chi-square or Fisher exact tests were used to compare categorical variables. The statistical significance was assessed using an alpha level of .05. Risk factors for hospital mortality were examined using multiple logistic regression, incorporating covariates describing type of surgery, income group, preoperative factors, and demographics. All statistical analyses were performed using SAS 9.4. The Institutional Review Board (IRB) of Augusta University approved the study protocol 1670755 on December 17, 2020, and publication of data. Patient written consent for the publication of the study data was waived by the IRB as this study represented no more than minimal risk.
Results
Patient Characteristics and Income Categories
The overall cohort of 11,018 surgeries included 10,355 PR (93.9%), 351 RPP (3.2%), and 312 with PO (2.8%) (Tables 1 and 2). The distribution of procedure groups differed by malformation. Among patients with VSD, 7125 of 7336, (97.1%) had PR, 112 of 7336 (1.5%) RPP, and 99 of 7336 (1.3%) PO. Among patients with a diagnosis of TOF, 2699 of 3045 (88.6%) had PR, 187 of 3045 (6.1%) RPP, and 159 of 3045 (5.2%) PO. Among those with CAVSD, 531 of 637 (83.4%) had PR, 52 of 637 (8.2%) RPP, and 54 of 637 (8.5%) PO. In the PR group, VSD was the most common diagnosis (7125 of 10,355, 68.8%), whereas TOF was the most common diagnosis (187 of 351, 53.3%) in the RPP group (Table 1). In the PO group, TOF was the most common diagnosis (159 of 312, 50.9%), followed by VSD (99 of 312, 31.7%) and CAVSD (54 of 312, 17.3%) (Table 2). In the PR group, the majority of the cohort were males (5783 of 10,355, 55.8%) while the opposite was true in the RPP group (186 of 351, 53.0% females) (Table 1). The basic characteristics of the PO cohort are displayed in Table 2. Distribution of economic categories of patients who underwent repair included high (571 of 10,706, 5.3%), upper middle (5342 of 10,706, 50%), and lower middle (4,793 of 10,706, 49.7%) (Table 1).
Basic Characteristics of Patients With Repair.
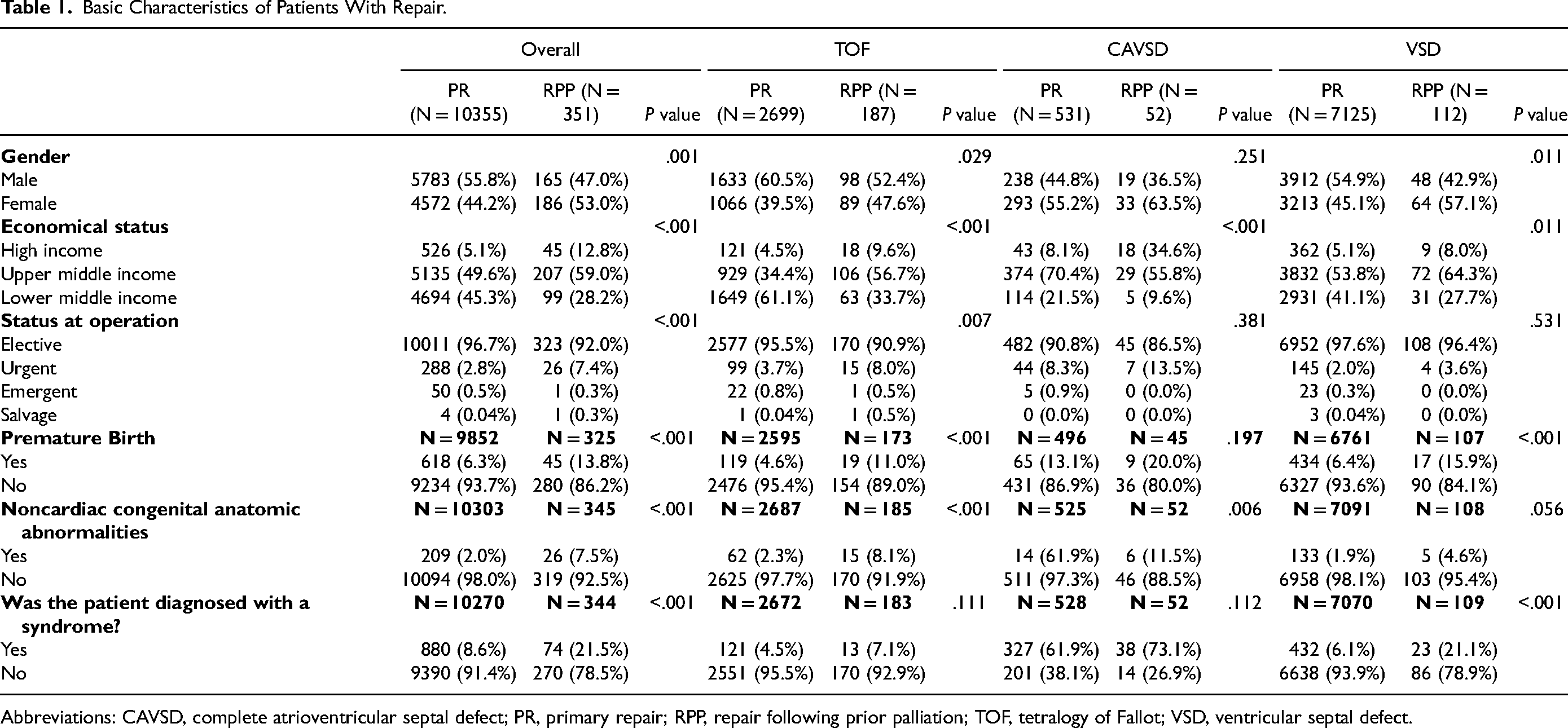
Abbreviations: CAVSD, complete atrioventricular septal defect; PR, primary repair; RPP, repair following prior palliation; TOF, tetralogy of Fallot; VSD, ventricular septal defect.
Basic Characteristics Among Palliation Only Procedures.
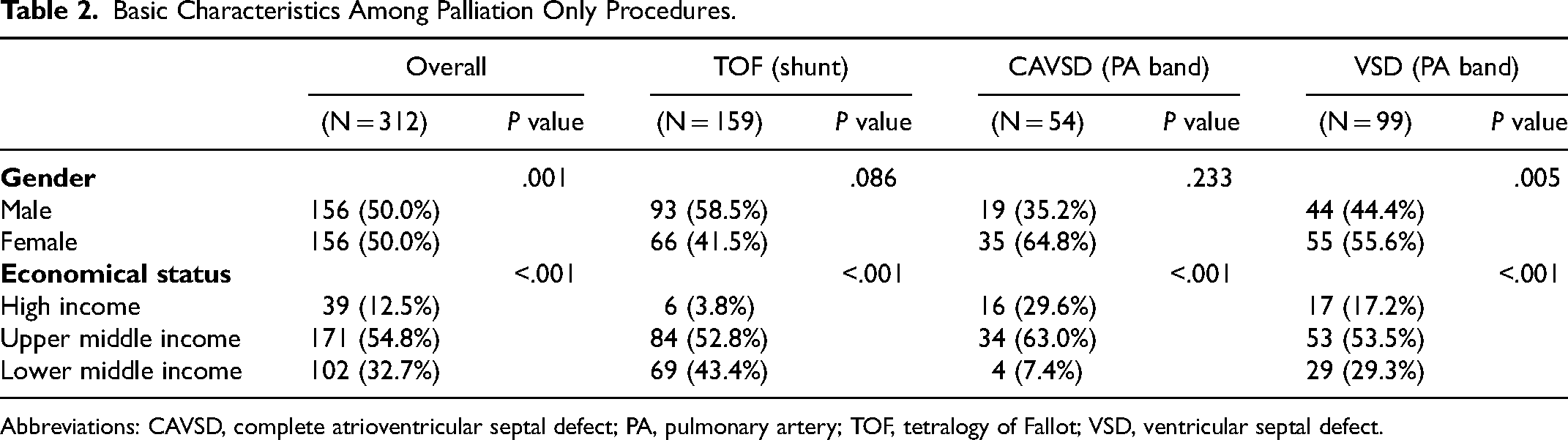
Abbreviations: CAVSD, complete atrioventricular septal defect; PA, pulmonary artery; TOF, tetralogy of Fallot; VSD, ventricular septal defect.
Comparison Between PR, RPP, and PO Cohorts
The age at PR, RPP, and PO across diagnoses and income levels are displayed in Table 3. Coupled with the marked delay in age at PR in both levels of middle-income compared with high-income countries, the likelihood of PR progressively decreased with increasing economic levels (Table 4). Among patients undergoing repair, the overall proportion undergoing RPP was 7.9% in high-income countries, 3.9% in upper middle-income countries, and 2.1% in lower middle-income countries (P < 0.001) (Table 1). Factors associated with PR included elective surgery and repair in a lower middle-income country (Table 4). Factors associated with staged repair (RPP) in this experience included higher economic levels, prematurity, associated noncardiac anomalies, and urgent or emergent operation (Table 5).
Age at Surgery by Diagnosis, Repair, and Income Classification.
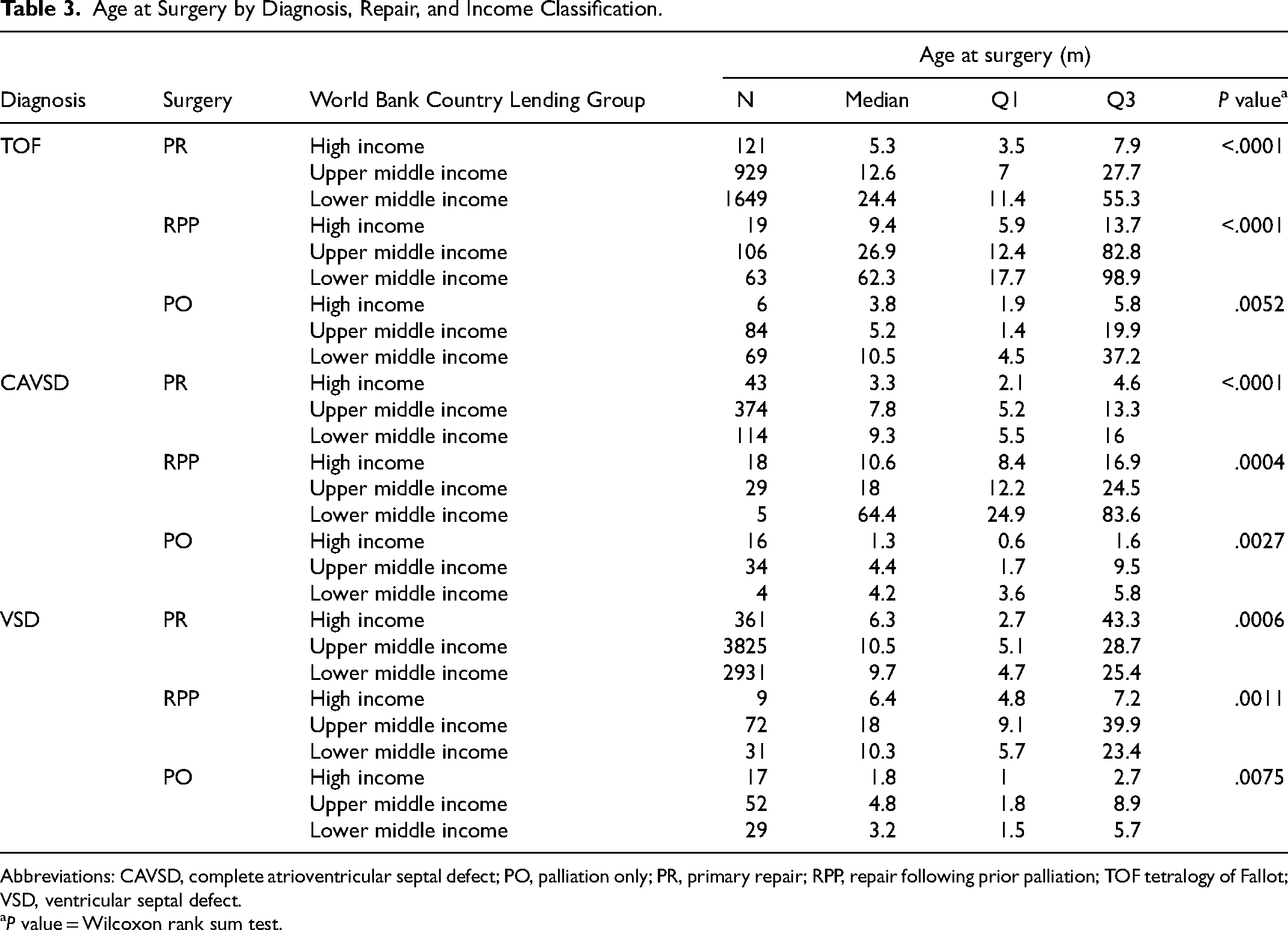
Abbreviations: CAVSD, complete atrioventricular septal defect; PO, palliation only; PR, primary repair; RPP, repair following prior palliation; TOF tetralogy of Fallot; VSD, ventricular septal defect.
P value = Wilcoxon rank sum test.
Predictors of Primary Repair Without Palliation (Multivariable Logistic Regression).
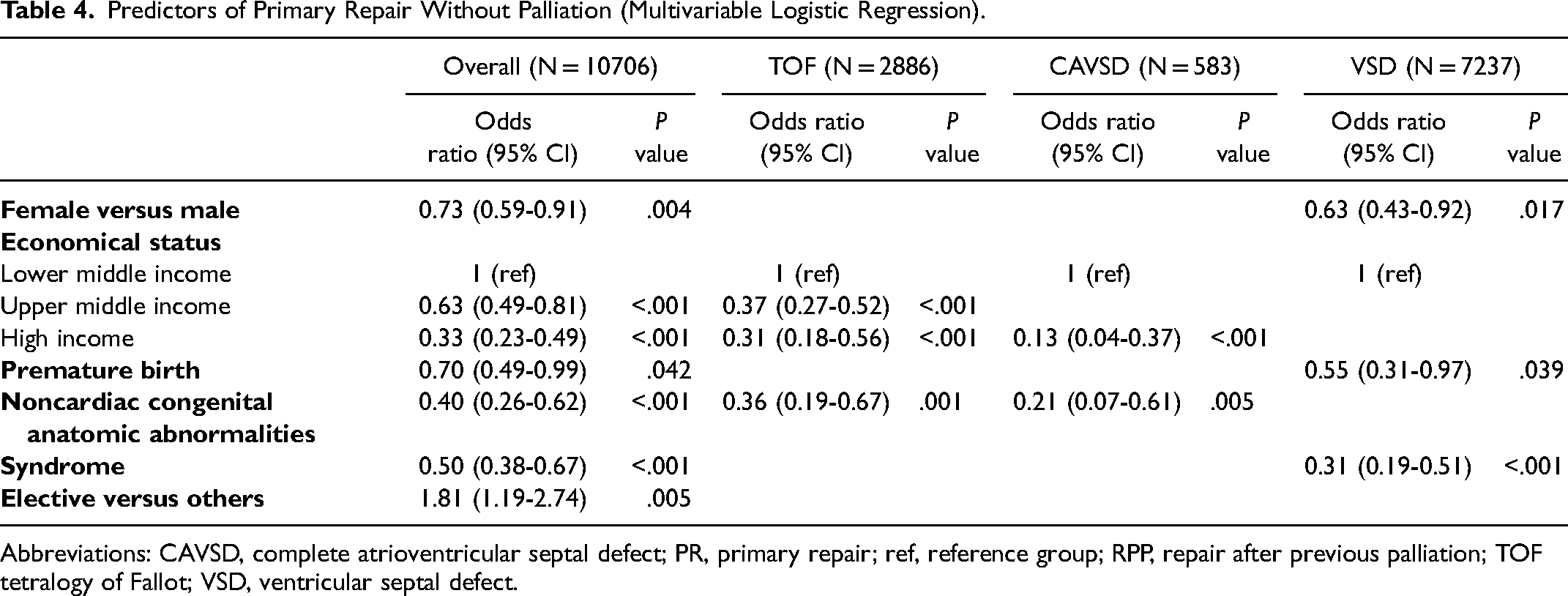
Abbreviations: CAVSD, complete atrioventricular septal defect; PR, primary repair; ref, reference group; RPP, repair after previous palliation; TOF tetralogy of Fallot; VSD, ventricular septal defect.
Predictors for Staged Repair (Multivariable Logistic Regression).
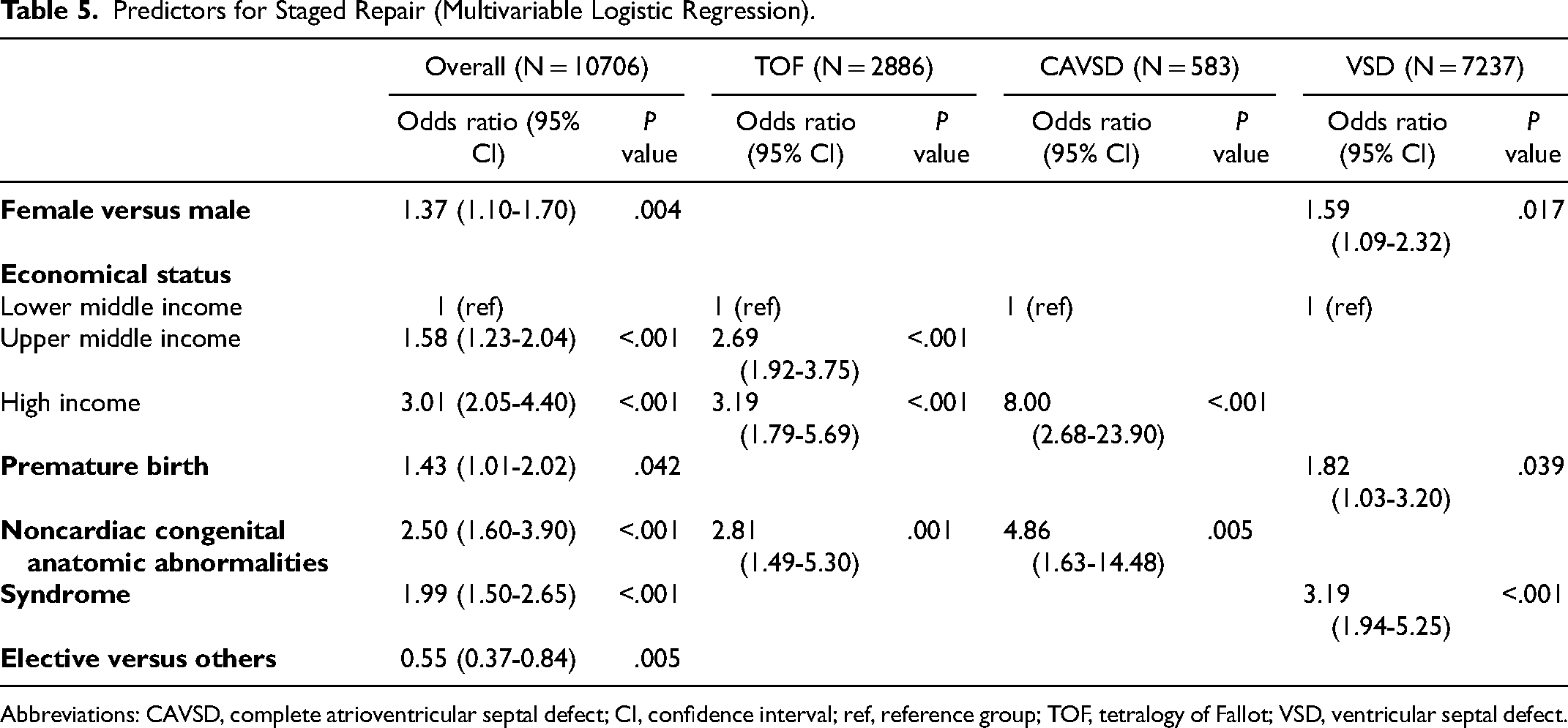
Abbreviations: CAVSD, complete atrioventricular septal defect; CI, confidence interval; ref, reference group; TOF, tetralogy of Fallot; VSD, ventricular septal defect.
Hospital Mortality
The median age at operation and hospital mortality for each of the three malformations is depicted in Table 6. The hospital mortality is further stratified by income level in Table 7. The hospital mortality is similar between PR and RPP for each malformation. However, the mortality following PO is higher in each group (Table 7). Risk factors for hospital mortality after repair include younger age (for TOF), prematurity, presence of genetic syndromes, and urgent or emergent operations (Table 8). In the overall group, high-income economic status was protective (Table 8). PR versus RPP was not a risk factor for any diagnostic group.
Age at Surgery and Mortality at Discharge by Diagnosis and Repair.
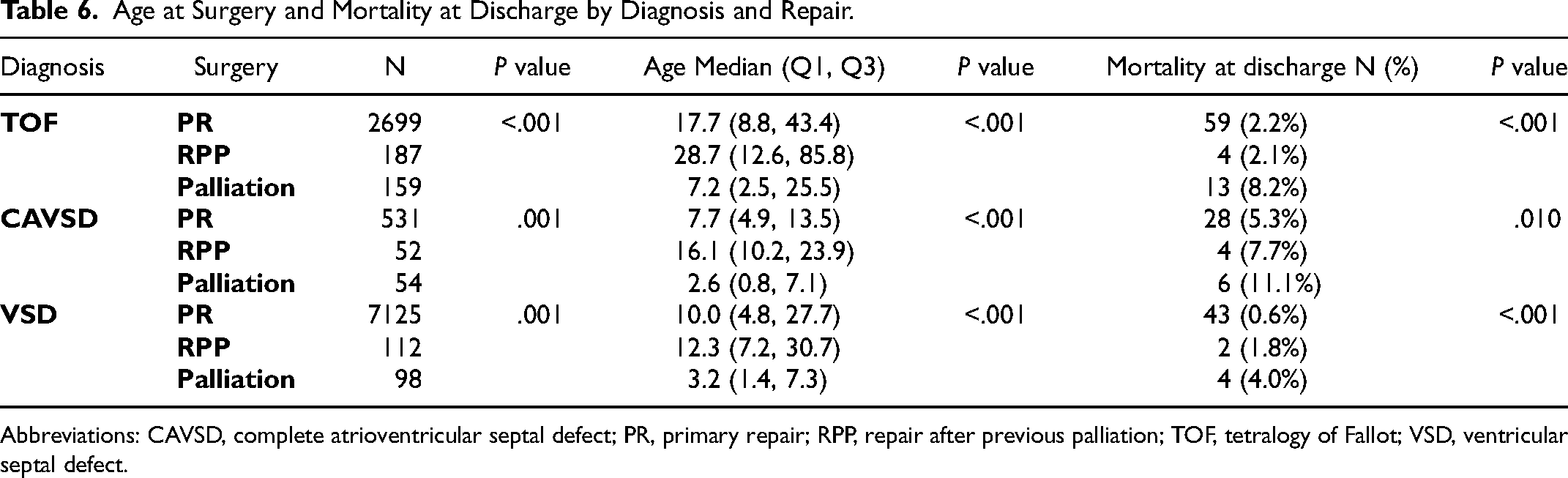
Abbreviations: CAVSD, complete atrioventricular septal defect; PR, primary repair; RPP, repair after previous palliation; TOF, tetralogy of Fallot; VSD, ventricular septal defect.
Mortality by Diagnosis, Repair, and Income Classification.
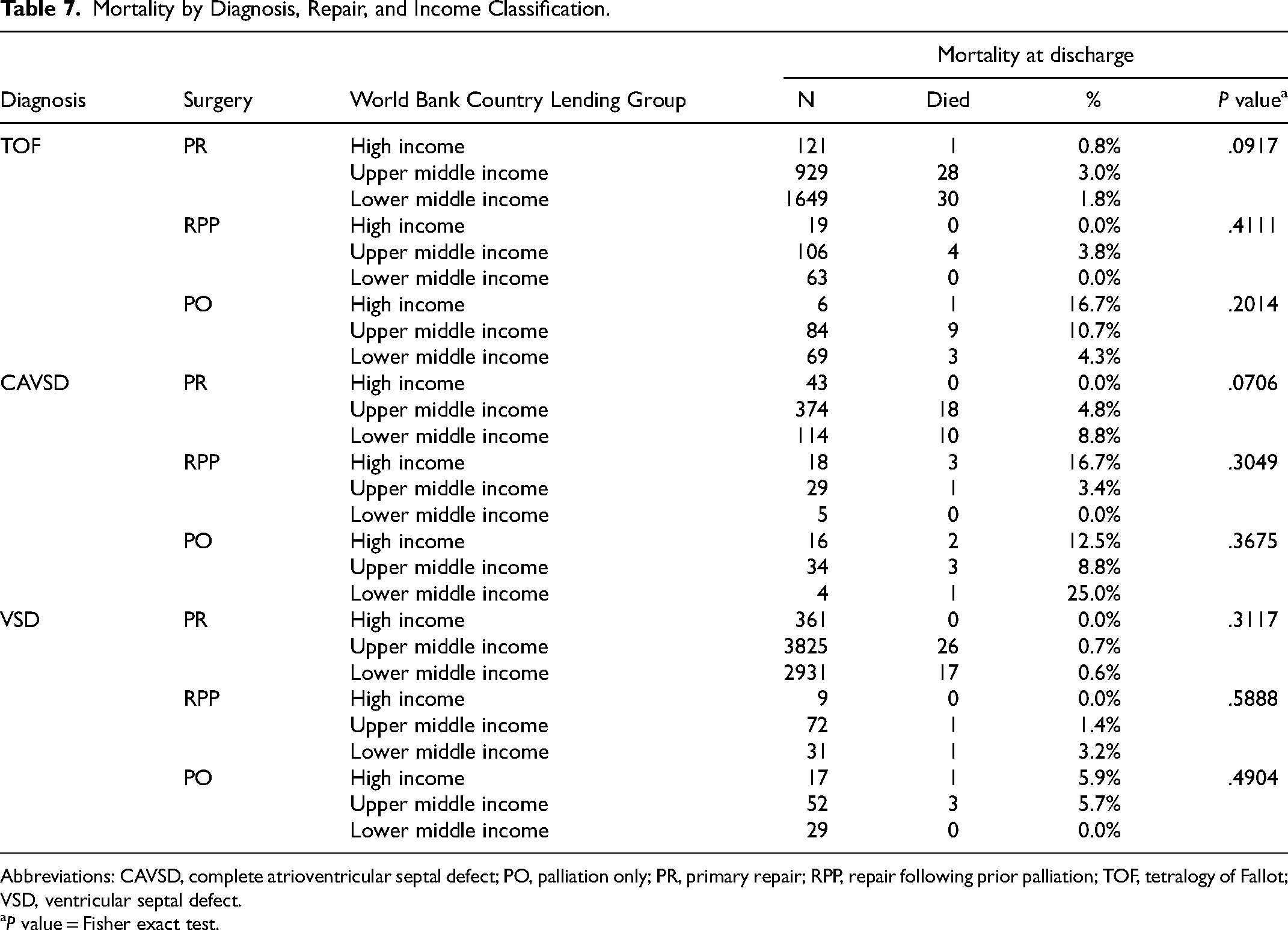
Abbreviations: CAVSD, complete atrioventricular septal defect; PO, palliation only; PR, primary repair; RPP, repair following prior palliation; TOF, tetralogy of Fallot; VSD, ventricular septal defect.
P value = Fisher exact test.
Risk Factors for Hospital Mortality After Repair (Multivariable Logistic Regression).
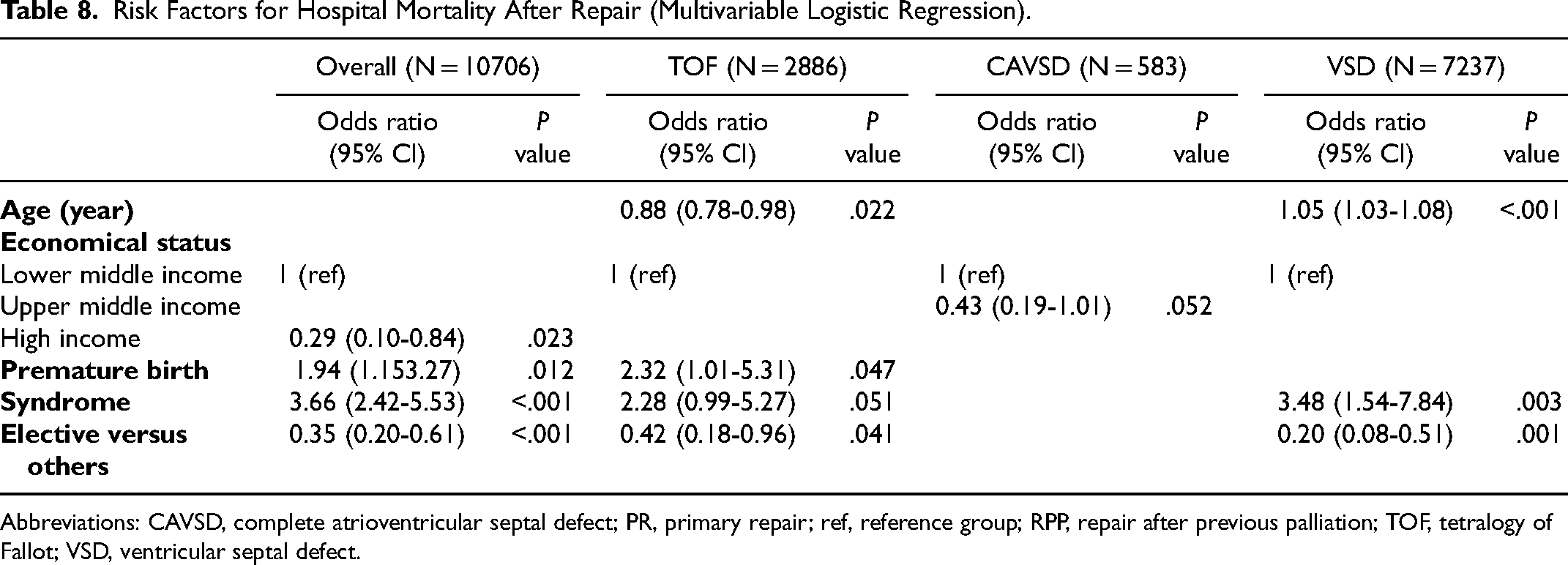
Abbreviations: CAVSD, complete atrioventricular septal defect; PR, primary repair; ref, reference group; RPP, repair after previous palliation; TOF, tetralogy of Fallot; VSD, ventricular septal defect.
Comment
Age at Surgery
This study focuses on three operations which may have prior palliation: VSD, TOF, and CAVSD. In this retrospective analysis from the WDPCHS greater than 90% of the surgeries for TOF, CAVSD, and VSD were PRs. This is consistent with other studies that have shown PR is more common for these defects than palliation even in early infancy.12,13 One potential reason for this high probability of PR is the difference in age at PR. Across all three defects, the age at PR or RPP was older than that reported in other contemporary series (Table 3). 13 This suggests that “early primary repair” may not be well represented in the database; rather PR patients have, to some extent, selected themselves out to survive to elective older repair. In lower income countries, this is not surprising given that patients frequently present late due to geographic or socioeconomic constraints, which also limit the ability to perform multiple procedures.5,14,15 This likely explains the increased probability of a PR in the lower middle income countries when compared with the rest of the cohort. However, an alternative explanation is that the intense focus on early mortality in high-income countries including ranking systems leads to diversion of high-risk patients into a palliative track thereby reducing the mortality of the definitive repair procedure.
Mortality
The overall mortality for both the PR and RPP cohorts were low at 1.3% and 2.8%, respectively, and continue to improve from previous large retrospective reviews.8,9 This points to the continued improvement in the globalization of congenital cardiac surgery. Initiatives set out by the World Society for Pediatric and Congenital Heart Surgery over ten years ago to work toward improving patient care, training and education, research, and community service continue to have an impact. 16 It is hard to draw conclusions from these data regarding palliation as the first surgery since this cohort had increased risk factors for mortality, consistent with the high-risk diversion strategy noted above. The importance of reporting cumulative mortality for both the initial palliative procedure and subsequent RPP will be necessary in future analyses.
It was interesting to note that older age at time of PR or RPP was not a risk factor for mortality in TOF. This finding is consistent with other studies looking at repair of TOF in low-income countries 17 and is related in part to the frequent later presentation of these patients and the self-selection to elective older repair. The risk factors for death in repair of TOF (younger age, prematurity, and nonelective surgery) are consistent with other recent studies.12,17 Patients with CAVSD and VSD also did not have an increased risk of early mortality associated with RPP. This is in keeping with a recent single institution series that had a higher percentage of prior PAB (∼35%) but noted no increase in mortality. 13
The relatively higher risk of palliative operations highlights the difficulties in low-income countries when these patients present late, have other comorbidities, are in a poor nutritional state, and demonstrate failure to thrive.14,15 This poses significant challenges to the heart team at the outset of care and underscores the importance of ongoing education at the level of primary care pediatricians and other healthcare workers. 18
Limitations
Our study has inherent limitations related to the WDPCHS structure and available data. First, detailed identification and analysis of the preoperative anatomic and physiologic characteristics was not possible, impeding understanding of the rationale behind specific surgical management plans. Second, the WDPCHS does not provide longitudinal follow-up across multiple encounters as well as age at diagnosis and time to intervention, limiting insights into patient survival with staged approaches, interstage mortality, or the risk for reintervention after different operative approaches. Third, there can be heterogeneity in the resources available between low- and middle-income countries that may not be accurately reflected in the database. Finally, results are limited to short-term, in-hospital outcomes and 90-day mortality. Despite these limitations, our study provides an important update on the approach to three specific congenital heart defects and surgical outcomes in a large contemporary international cohort. These important limitations emphasize the desirability of collecting patient-based data going forward rather than procedure/encounter-based data which encourage diversion of high-risk patients and obscures conclusions that can be drawn regarding patient survival.
Conclusion
In lower and upper middle-income countries, definitive repair is often delayed. Early mortality after PR is similar to early mortality after a staged repair although the latter does not include palliative and interstage mortality. Early mortality for PR without palliation varies according to country income status. Initial palliation continues to have a small but important role in the management of these three specific congenital heart defects.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.