
Abstract
Prenatal diagnosis of pericardial mass, with associated large pericardial effusion, resected postnatally and diagnosed to be ectopic hepatic tissue on pathology.
Case Report
A singleton fetus was referred for fetal echocardiography at 25 weeks of gestation for investigation of a pericardial effusion noted on obstetrical ultrasound. Fetal echocardiogram showed a left posterior–inferior parietal pericardial mass with associated pericardial effusion (Figure 1). The mass was round, well-circumscribed, and avascular. Although it did not grow rapidly and remained of homogenous texture, the mass was thought to likely represent a teratoma. The effusion became progressively larger on serial follow-up studies without significant hemodynamic compromise as demonstrated by normal Doppler interrogation of umbilical vessels and ductus venosus. There were no signs of hydrops fetalis. However, there was significant lung compression and this raised concerns that this would adversely affect the transition from fetal to postnatal life. A cesarean section was planned at 37 weeks and 4 days of gestation. This was preceded by an uncomplicated fetal pericardiocentesis on the same day to stabilize the patient before birth and during transition to post-fetal life. Postnatally, the patient was monitored in the neonatal intensive care unit, where he remained clinically stable with normal hemodynamics and breathing spontaneously on room air. Postnatal transthoracic echocardiograms confirmed the presence of a pericardial mass and a large pericardial effusion causing dextroversion of the cardiac apex. The intracardiac anatomy and ventricular function were normal. Patent foramen ovale and ductus arteriosus shunting left to right were noted. Multidisciplinary evaluation raised concerns for recurrent pericardial effusion, prompting consideration for urgent excision and effusion drainage for diagnostic and therapeutic purposes on the fourth day of life. Repeat echocardiography following excision at one, three, and ten months revealed no recurrence of tumor or pericardial effusion.
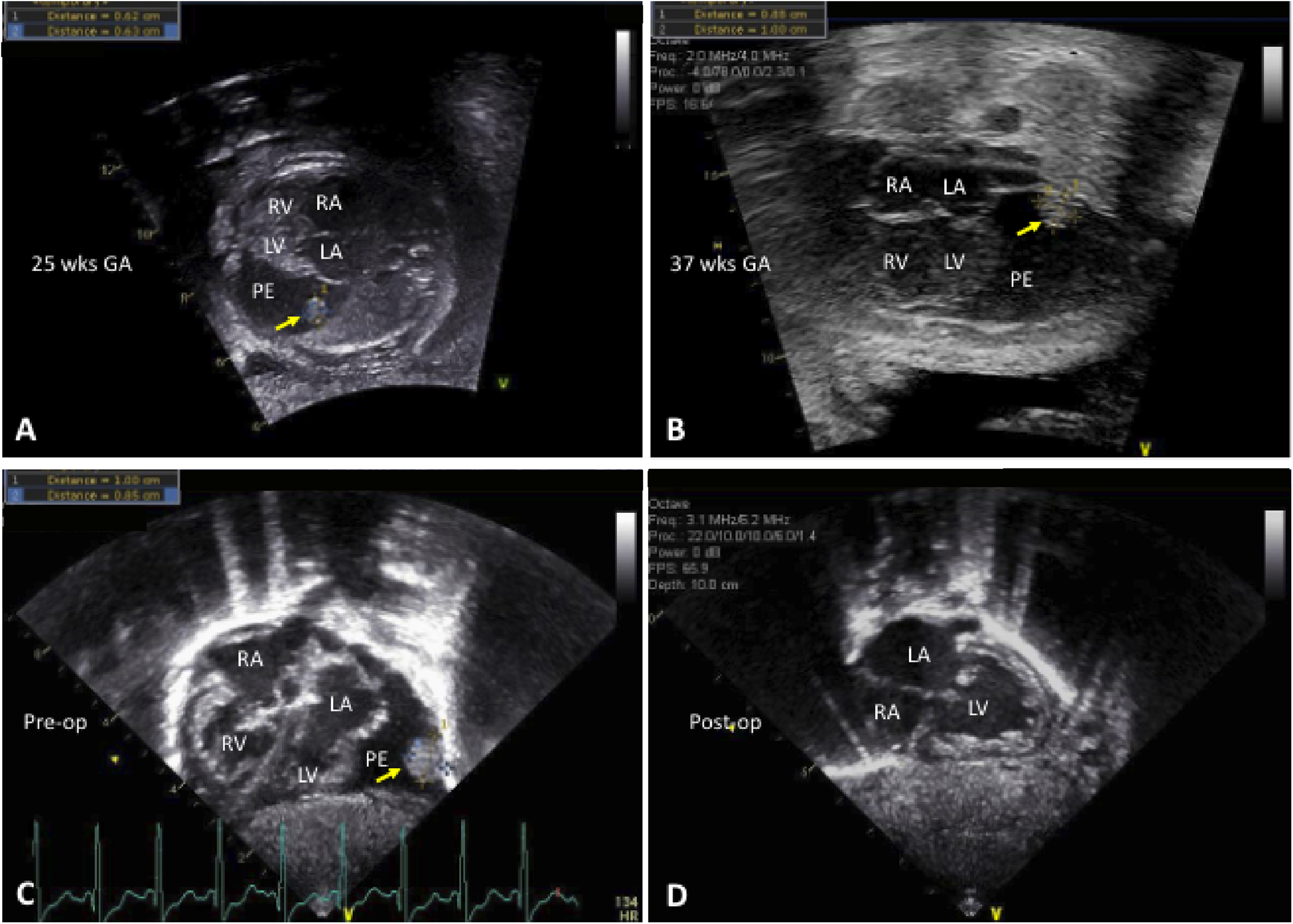
Panel A: Fetal echocardiogram at 25 weeks of gestational age. Panel B: Fetal echocardiogram at 37 weeks. Panel C: Postnatal echocardiogram immediately after birth. Panel D: Postnatal echocardiogram after mass resection and drainage of pericardial effusion. LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; PE, pericardial effusion. Thick arrow points to mass.
Technique
Midline sternotomy was employed with cardiopulmonary bypass circuit on standby. The pericardium was opened in the midline and approximately 50 mL of brown pericardial fluid was drained and sent for testing. The pericardium was examined in its entirety identifying a spherical pedunculated mass attached to the posterior–inferior parietal layer of the pericardium on the left side (Figure 2). The mass was resected by removing a ring of pericardium around the narrow stalk using sharp dissection without injury of the left phrenic nerve (Video). The patent ductus arteriosus was ligated. The patient tolerated the procedure well and was extubated on the first postoperative day. On histological examination, the mass is entirely composed of hepatic tissue with well-formed portal tracts and central veins (Figure 3).
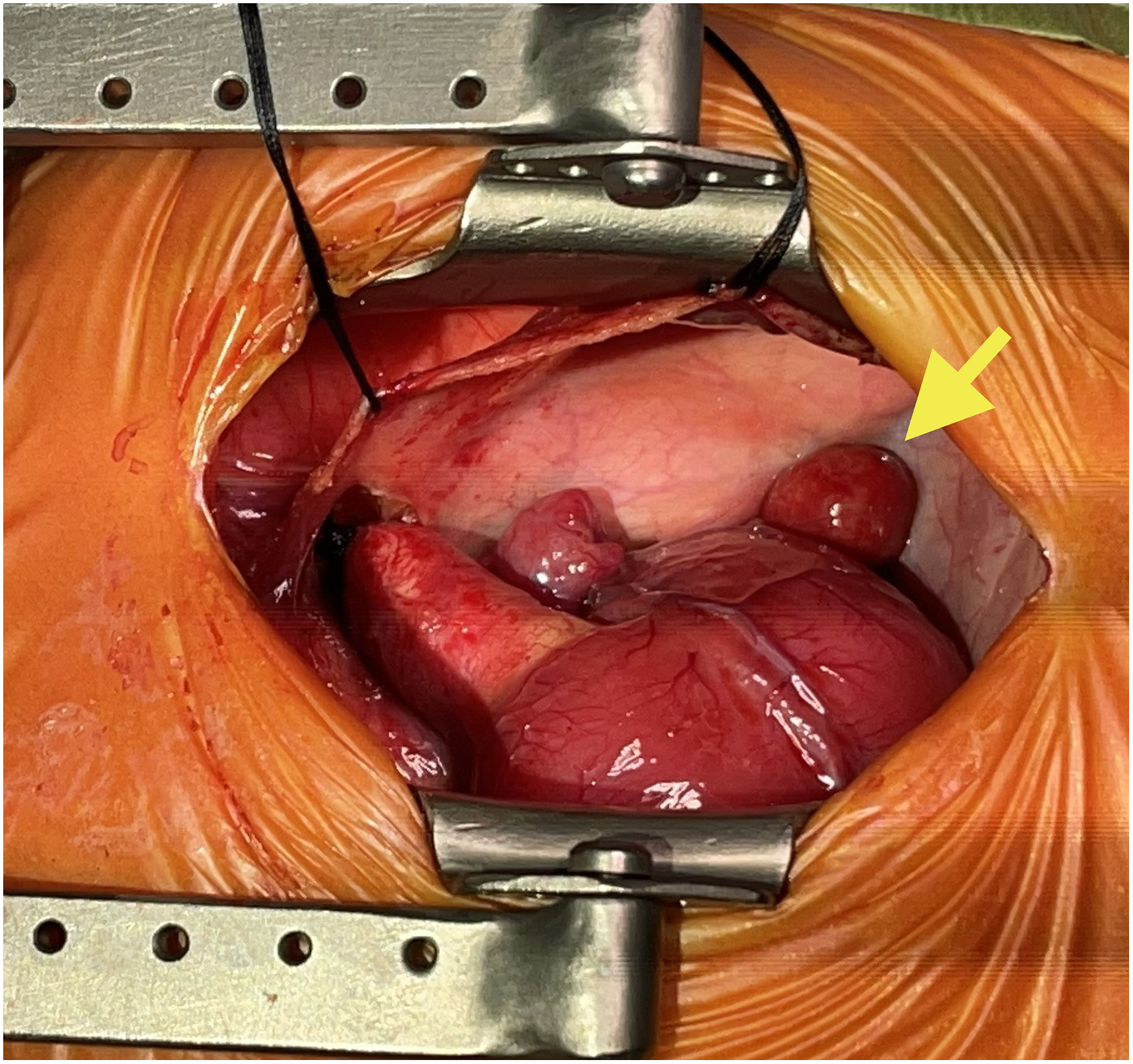
Intraoperative view of the intrapericardial ectopic hepatic tissue (arrow) from the right side of patient.
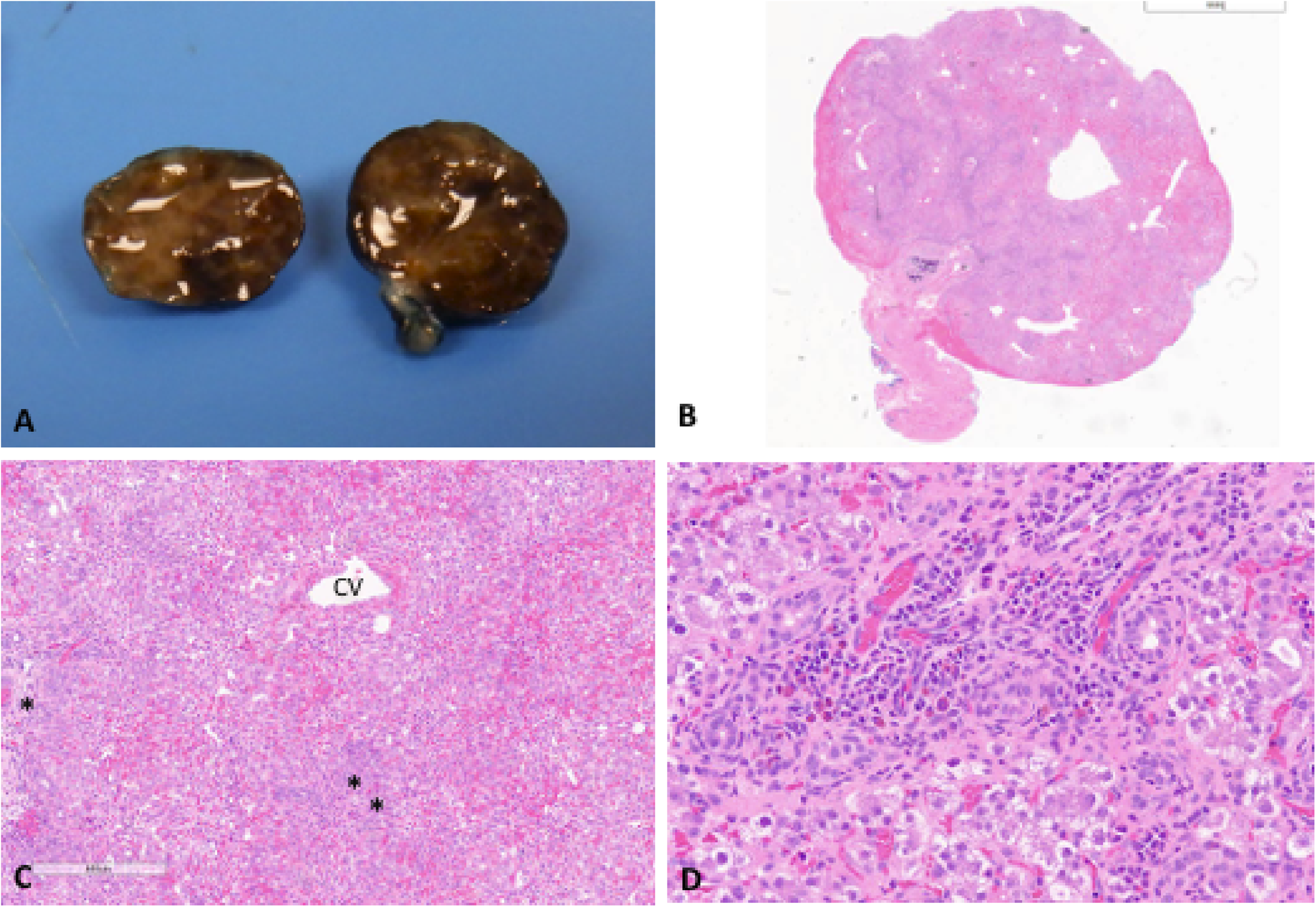
Panel A: Macroscopic image showing homogeneous brown mass with fibrous pedicle. Panel B: Low power full-thickness section of mass (H&E). Panel C: Medium power image demonstrating well-formed portal tracts and central veins. Panel D: Periportal extramedullary hematopoiesis, feather degeneration, and presence of intracellular bile. CV, central vein. Asterisk denotes portal tracts.
Discussion
Ectopic hepatic tissue is exceedingly rare, characterized by the presence of hepatic tissue outside the native liver. It is usually found near the gallbladder or other intra-abdominal organs but has been reported in the thoracic region, often attached by a pedicle. 1 It is believed to occur secondary to aberrant migration of the liver during embryologic development. The hepatic diverticulum is derived from the primitive foregut and grows into the mesenchyme of the septum transversum which also gives rise to the central portion of the diaphragm. Aberrant growth into the thoracic cavity may sequester hepatic tissue after closure of the diaphragm. It is generally asymptomatic and discovered incidentally. Histologically, it recapitulates normal hepatic architecture but may be associated with obstructive changes and/or inflammation, likely secondary to its lack of connection to the normal biliary tree and hepatic vascular supply. Ectopic hepatic tissue is associated with a risk of malignant transformation into hepatocellular carcinoma; thus ensuring negative margins during excision and careful pathologic review of the ectopic tissue are paramount. 2
There are approximately 120 documented cases of ectopic hepatic tissue, but to our knowledge, none have been discovered in the pericardium of a neonate and only one previous report of an intrapericardial ectopic hepatic tissue was reported on the autopsy of a 75-year-old man. 3 In our case, the pericardial location of the tumor and its mechanical complication with a large pericardial effusion compressing the lungs and pushing the apex of the heart was important in the decision to remove the tumor and obtain a definite diagnosis. The diagnosis of ectopic hepatic tissue without surgery is difficult and not easily recognized in radiological studies given the rarity of this condition and thus the lack of awareness. 4 This is especially relevant in our patient given the associated pericardial effusion, making other diagnoses such as teratoma more likely. 5 Although rare, pericardial teratomas are the most common pericardial tumors diagnosed during fetal life. Retrospectively, the location, homogeneity, and slow growth of the mass in this case were atypical for teratoma. However, its avascular nature ruled out a hemangioma, the second most frequently encountered pericardial tumor in the fetus.
In this report, we present to our knowledge the first neonatal case reported of an ectopic hepatic tissue arising in the pericardium and associated with a large pericardial effusion, which was surgically excised.
Supplemental Material
Supplemental Material
sj-asf-2-pch-10.1177_21501351231201851 - Supplemental material for Intrapericardial Ectopic Hepatic Tissue Masquerading as a Fetal Pericardial Tumor
Supplemental material, sj-asf-2-pch-10.1177_21501351231201851 for Intrapericardial Ectopic Hepatic Tissue Masquerading as a Fetal Pericardial Tumor by Fadi Hage, Alqasem Al Mosa, Miriam Blumenkrantz, Richard Nicolas Brown, Tiscar Cavalle Garrido, and Pierre-Luc Bernier in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Authors’ Statement
Informed written consent was obtained from the parents for this publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.