
Abstract
Surgical repair of right aortic arch and aberrant left subclavian artery has traditionally involved ligamentum division. Such patients can have stenosis at the origin of the aberrant subclavian artery either at the time of presentation or later. The more recently popularized repair involving resection of Kommerell diverticulum with transfer of the subclavian artery to the left carotid artery allows resection of the stenotic segment and serves as an effective treatment for subclavian stenosis as well. We present three cases of early repair of this arch anomaly with associated subclavian stenosis repaired successfully in that manner.
Introduction
Vascular rings present with a frequency as high as seven in 10,000 live births. 1 Contemporary fetal detection and use of computed tomography (CT) have led to increased early detection of these lesions and earlier repair in many centers. 2 Right aortic arch with aberrant left subclavian artery (RAA-ALSA) is a common form of vascular ring (15%-25%), and different surgical techniques have been proposed to repair the lesion. 3 Isolated division of the ligamentum arteriosum or division with resection of the Kommerell diverticulum (KD) and translocation of the aberrant left subclavian artery to the left carotid artery have been utilized. 4 There have been reports of patients who underwent division of the ligamentum arteriosum alone and were found to have recurrence of symptoms secondary to aneurysmal compression by the KD or a sling-like effect from the aberrant subclavian artery which led to additional interventions. Additionally, there seems to be an important incidence (80%) of a stenotic origin of the aberrant left subclavian artery at presentation or presenting later, after ligamentum division.4–6 We present three cases of RAA-ALSA with left subclavian artery stenosis that underwent successful surgical repair including resection of the KD and stenotic segment of the subclavian artery with transfer of the subclavian artery to the carotid artery.
Case 1
A full-term boy was diagnosed prenatally with a vascular ring, with right aortic arch with aberrant left subclavian artery confirmed on postnatal echocardiogram. CT scan at two weeks of age demonstrated RAA-ALSA with a large KD (Figure 1). Diverticulum measured 4.1 × 3.3 mm on the proximal end while the origin of a subclavian artery from the diverticulum measured 2.3 × 2.4 mm. The infant was asymptomatic with no stridor or appreciated difficulties with feeding and showed appropriate weight gain.
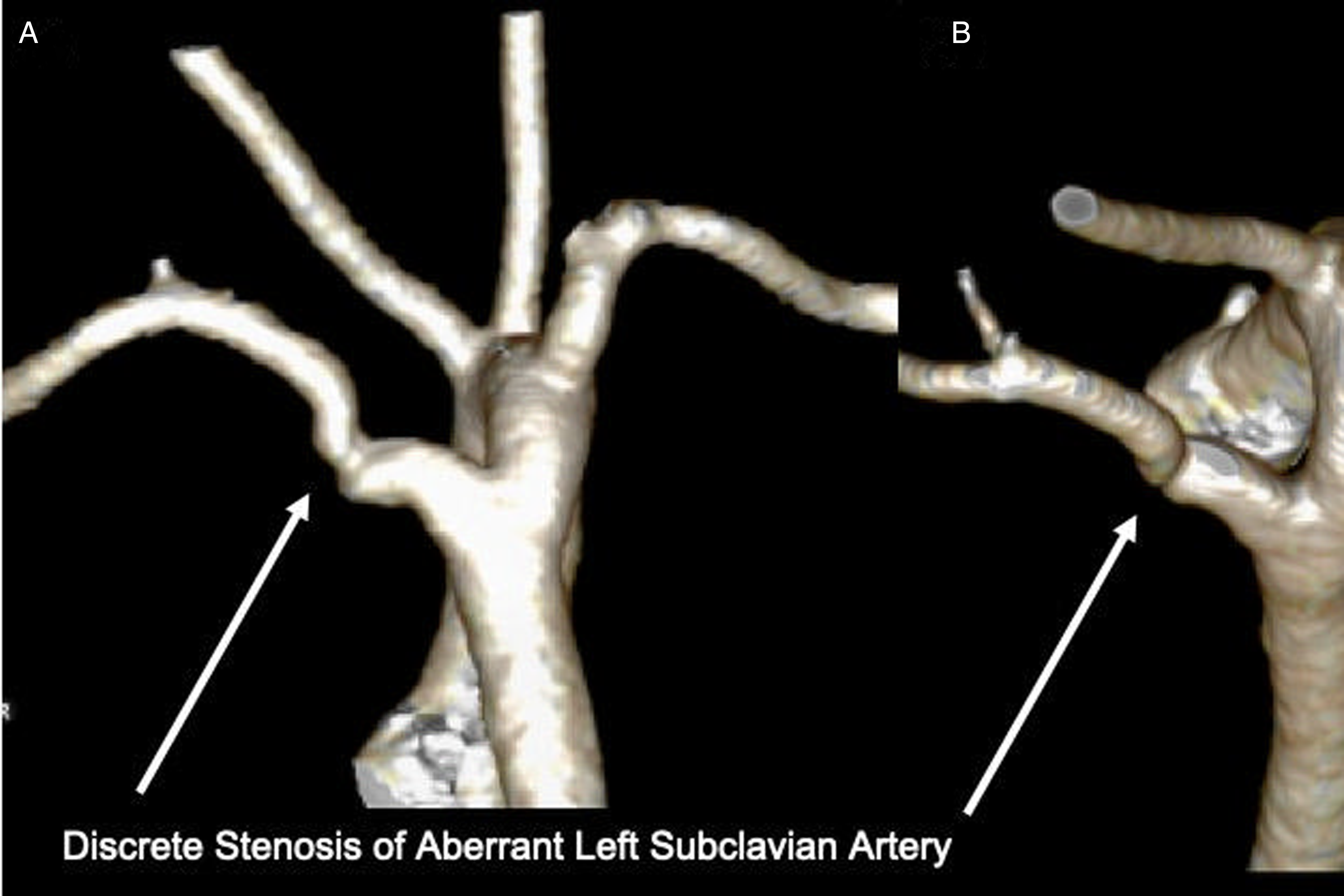
Preoperative 3D computed tomography (CT) images for case 1. Posterior (A) and Posterior–Superior view (B) of 3D reconstructed CT images that demonstrated a right aortic arch with a discrete narrowing of the aberrant left subclavian artery at two weeks of age prior to surgery.
Repair was performed at three months of age with ligamentum division and KD resection via left thoracotomy. The stenotic origin of the left subclavian artery was resected, and the artery anastomosed end to side to the left carotid artery under systemic heparinization. The postoperative course was uncomplicated. Postoperative echocardiogram demonstrated laminar flow into the left subclavian artery. Follow-up CT scan performed a few months later for questionable persistent feeding difficulty showed a widely patent left subclavian artery with no vascular compression of esophagus or airway (Figure 2).
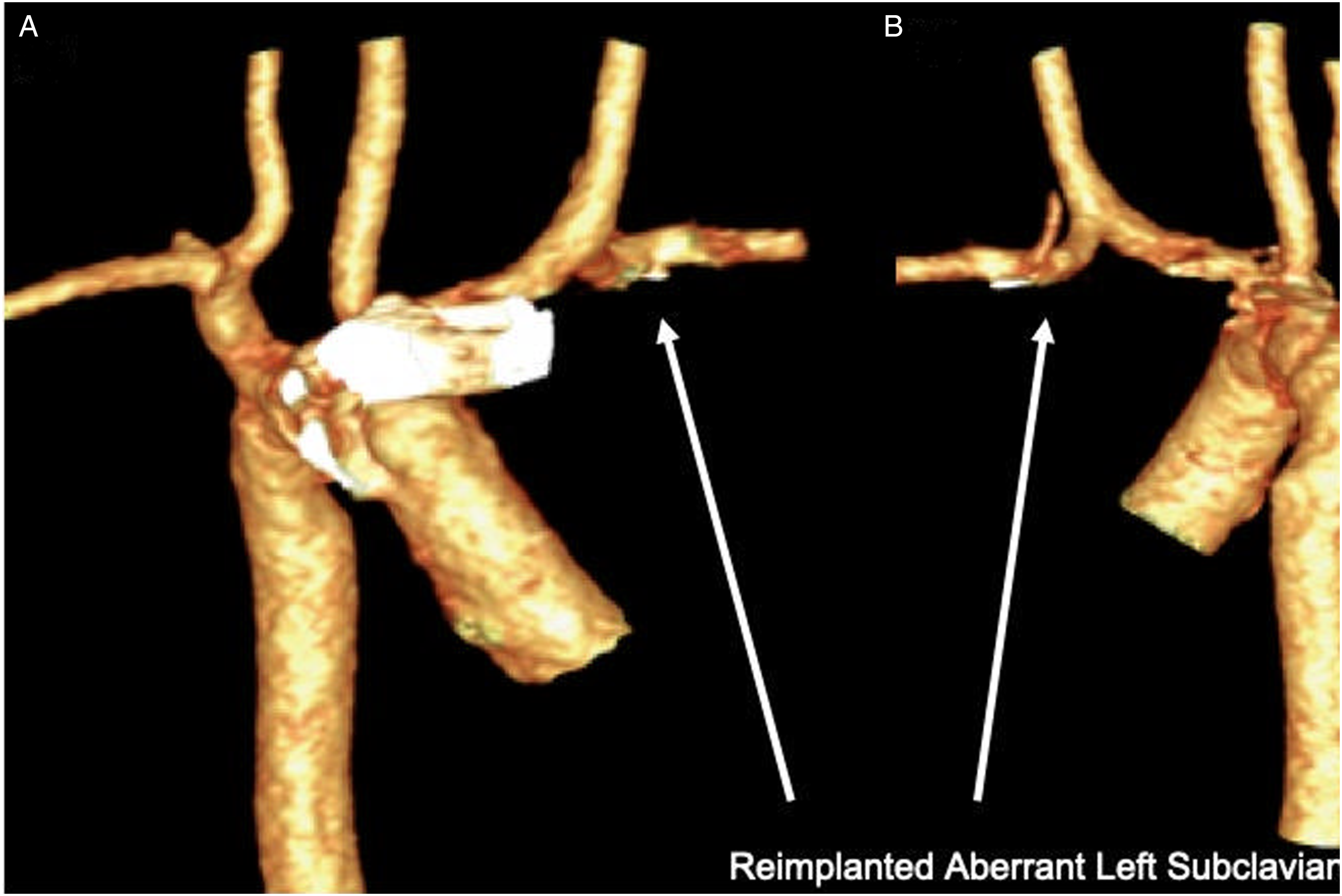
Postoperative 3D computed tomography (CT) images for case 1. Anterior view (A) and Posterior view (B) of 3D reconstructed CT images demonstrated widely patent reimplanted left subclavian artery to the left carotid artery.
Case 2
A full-term male neonate was found to have RAA-ALSA. Cardiac CT at one month of age showed the same along with evidence of a discrete narrowing between the diverticulum and proximal left subclavian artery (Figure 3). At two months of age, he had stridor and underwent repair as above. Intraoperatively, the left subclavian artery was noted to be nearly closed at its origin from the KD. This segment was resected, and the artery was translocated to the left carotid artery. Echocardiogram two weeks postoperatively demonstrated a widely patent left subclavian artery with no blood pressure gradient between the upper extremities, and the patient also had resolution of respiratory symptoms.
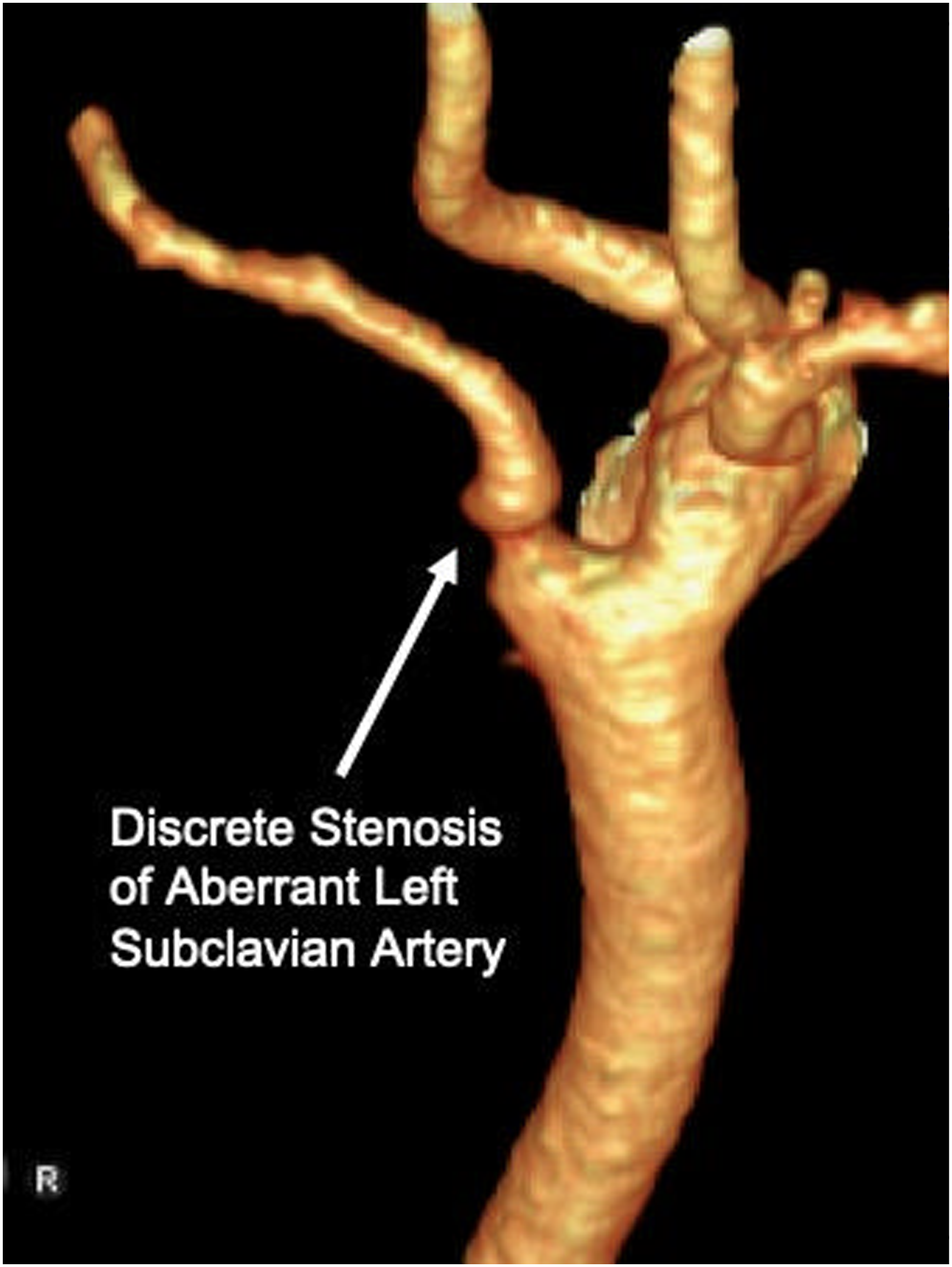
Preoperative 3D computed tomography (CT) images for case 2. Posterior view of 3D reconstructed CT image that demonstrated a right aortic arch with a discrete narrowing of the aberrant left subclavian artery at one month of age prior to surgery.
Case 3
A full-term newborn with prenatal concern for a vascular ring was born via cesarean section. He had no respiratory or feeding difficulty and postnatal CT at four months of age confirmed an RAA-ALSA with narrowing at the junction of diverticulum (5 × 5 mm) and aberrant left subclavian artery origin (2.5 × 2.5 mm). He underwent a surgical repair as above and was discharged home on postoperative day 1.
Discussion
Subclavian artery stenosis at its origin from the KD is seen accompanying RAA-ALSA, early and late. One would suspect this to be ductal tissue constriction in etiology. While such stenosis can be dealt with when it develops, as earlier repairs are done more commonly, it may make sense to modify the primary repair to avoid need for reintervention. Our cases suggest that subclavian artery stenosis in RAA-ALSA may be more common than previously thought, and also add an additional reason to consider adding resection of KD and transfer to the carotid artery to the ligamentum division in the primary repair. Progression of untreated subclavian artery stenosis may potentially lead to subclavian artery steal syndrome,7,8 which may be prevented by repair at the initial operation. Our more recent institutional approach to RAA-ALSA has been to resect the KD and stenotic segment and to transfer to the carotid artery with excellent short-term outcome with no blood pressure gradient between two upper extremities in the immediate postoperative period, and imaging studies consistent with widely patent subclavian arteries. Future study with doppler ultrasound to assess the potential development of restenosis of the translocated subclavian artery would be helpful.
Conclusion
Right aortic arch with aberrant left subclavian artery with stenosis of the left subclavian artery can be safely repaired with resection of the stenotic segment along with the KD, and reimplantation of the left subclavian artery to the left common carotid artery.
Footnotes
Authors' Statement
Permission to publish the case report was granted by the parents of each patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.