
Abstract
Background
This study examined preoperative, intraoperative, and postoperative data to identify factors that are associated with prolonged mechanical ventilation (PMV) and prolonged intensive care unit length of stay (ICU LOS) in tetralogy of Fallot (TOF) patients undergoing repair surgery.
Methods
A retrospective study was carried out after approval from the institutional review board. All patients (age 0-52 years) who underwent TOF repair from January 2016 to September 2022 were included. Prolonged mechanical ventilation was defined as >24 h of ventilation, while prolonged ICU LOS was defined as ICU stay >3 days.
Results
A total of 922 patients were included, among whom 288 (31.2%) were intubated for >24 h and 222 (24.1%) stayed in ICU for >3 days. Younger age (odds ratio [OR] = 2, 95% confidence interval [CI] 1.2-3.3, P = .007), lower weight (OR = 2.1, 95% CI 1.2-3.5, P = .003), and residual lesion (OR = 3.27, 95% CI 1.2-8.7, P = .017) were associated with PMV. Moreover, independent risk factors for prolonged ICU LOS are similar to PMV risk factors, including younger age (OR = 2.3, 95% CI 1.28-4.12, P = .005), lower weight (OR = 2.83, 95% CI 1.58-5, P < .001), underweight status (OR = 1.7, 95% CI 1.12-2.57, P = .012), and residual lesion (OR = 3.79, 95% CI 1.43-10.05, P = .007). Both aortic cross-clamp and cardiopulmonary bypass times did not exhibit clinically significant risk factors toward PMV and prolonged ICU LOS.
Conclusions
The risk factors for PMV and prolonged ICU LOS were residual lesion, younger age, and lower weight. Nutritional status contributed to the risk of prolonged ICU LOS, but not PMV. Consideration of these factors may provide optimal care to improve the outcome following TOF corrective surgery.
Keywords
Introduction
Tetralogy of Fallot (TOF) is the most common form of cyanotic congenital heart disease with an incidence of three per 10,000 live births, accounting for 5% to 7% of all congenital heart defects. 1 It is characterized by ventricular septal defect (VSD), overriding aorta, right ventricular hypertrophy (RVH), and obstruction of the right ventricular outflow tract (RVOT). 2 Since the first surgery for TOF by Alfred Blalock, Helen B. Taussig, and Vivien Thomas in 1944, the development of surgical methods for treating patients with TOF has significantly progressed.3,4 Advances in surgical techniques, anesthesia, and postoperative management have led to significantly decreased morbidity and mortality rates. 5 However, the morbidity and mortality rate in developing countries is still relatively high, with a reported incidence of 6.9% to 15.3%. 6 Duration of mechanical ventilation (MV) and length of stay in the intensive care unit (ICU LOS) have become important indicators closely related to recovery and outcomes after TOF repair. 7 Risk factors associated with prolonged mechanical ventilation (PMV) and ICU LOS have been documented before but with a smaller number of patients.8‐10 In Indonesia, there has never been a study describing risk factors for morbidity. 11 Early identification of factors associated with PMV and prolonged ICU LOS is essential in developing methods to improve health care efficiency and to reduce resources used as well as to minimize treatment costs in these patients. Thus, this retrospective investigation aims to identify potential perioperative risk factors associated with increased duration of MV and ICU LOS in patients who underwent surgical repair of TOF in a large, single center population.
Materials and Methods
Patient Population
All patients with a diagnosis of TOF who underwent repair between January 2016 and September 2022 were identified from the hospital database. A total of 922 patients with complete medical records were included in the study. The protocol of this retrospective study was approved by the Institutional Review Board of the National Cardiovascular Center Harapan Kita. Due to the design of our study, the need for informed consent was waived. Patients with incomplete medical record data were excluded from this study.
Data Collection
We chose variables to analyze based on their potential importance and effect on postoperative cardiac care according to previous literature. All data were retrieved from the inpatient medical records. The ethical consideration of this retrospective study has been reviewed and approved by the institutional review board of the National Cardiovascular Center Harapan Kita with unique number ID LB.02.01/VII/039/KEP039/2022.
The preoperative data that we collected included demographic information such as age at the time of surgery, gender, weight, diagnosis of the patients, and history of Down syndrome. Additionally, we calculated the weight-for-age status using the available data regarding date of birth, date of surgery, gender, and absolute weight during admission. Based on the Indonesian Pediatric Society guidelines, the measurement of weight-for-age status was based on the World Health Organization (WHO) growth chart for children < 5 years of age, followed by the Center for Disease Control and Prevention (CDC) growth chart for children > 5 years of age.
For intraoperative data, the following were collected and analyzed: cardiopulmonary bypass (CPB) time, aortic cross-clamp (AOX) time, and presence of significant residual lesions on transesophageal echocardiogram. In this study, we defined residual lesion as an intended or unintended postoperative structural heart abnormality, which includes abnormalities that either exist before or occur during the surgery. This definition also adheres accordingly to that in the previous study. 12 Types of residual lesions consist of pulmonary stenosis (PS), pulmonary regurgitation (PR), and VSD. Assessment reports of the severity of all residual lesions (especially PS and PR) were determined by pediatric cardiologists along with the gradient results based on the guidelines published by the American Society of Echocardiography 2009. 13 For surgical techniques, our center has established a trans-tricuspid approach for the repair of VSD malalignment in TOF patients. Augmentation of RVOT could be done by using either transannular patch (TAP) repair or valve-sparing repair.
Postoperative data consisted of ICU LOS, duration of MV, 1-h lactate levels following ICU admission, and postoperative adverse events (such as arrhythmia, tachyarrhythmia, junctional ectopic tachycardia, and atrial fibrillation, mentioned in Table 1).
Patient Demographics and Characteristics Data.
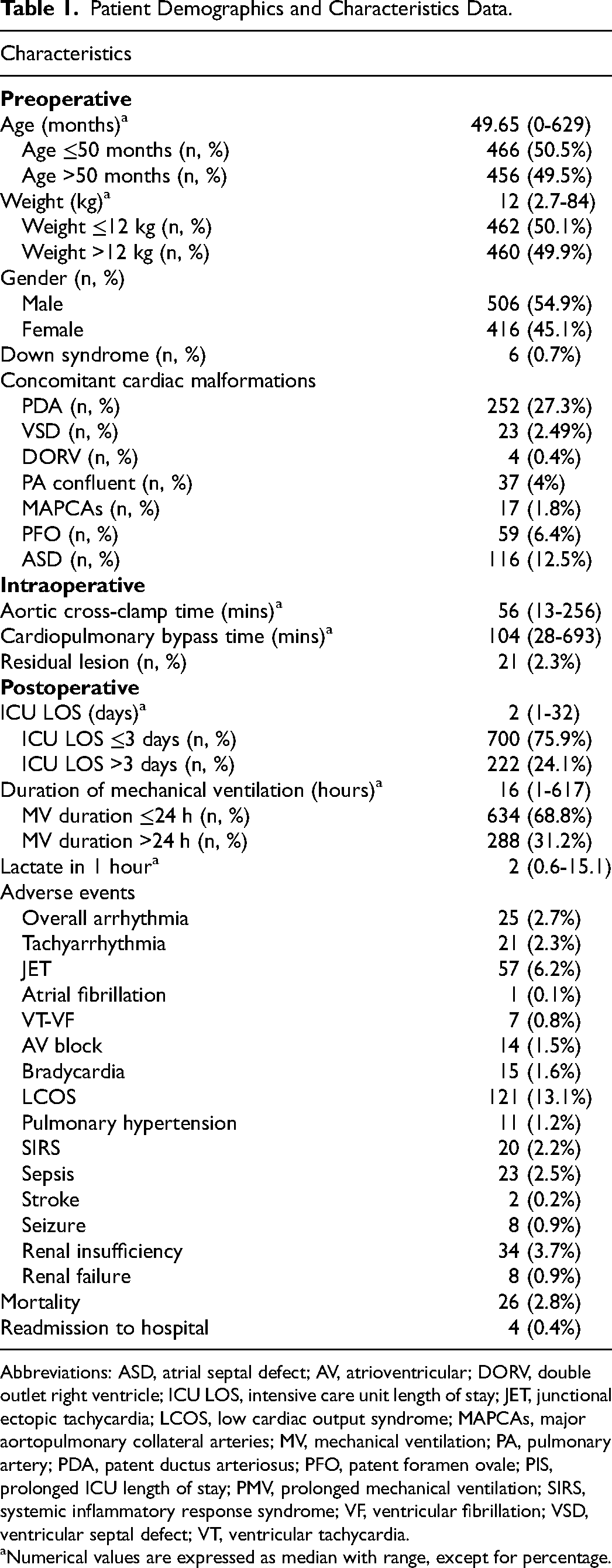
Abbreviations: ASD, atrial septal defect; AV, atrioventricular; DORV, double outlet right ventricle; ICU LOS, intensive care unit length of stay; JET, junctional ectopic tachycardia; LCOS, low cardiac output syndrome; MAPCAs, major aortopulmonary collateral arteries; MV, mechanical ventilation; PA, pulmonary artery; PDA, patent ductus arteriosus; PFO, patent foramen ovale; PIS, prolonged ICU length of stay; PMV, prolonged mechanical ventilation; SIRS, systemic inflammatory response syndrome; VF, ventricular fibrillation; VSD, ventricular septal defect; VT, ventricular tachycardia.
Numerical values are expressed as median with range, except for percentage.
According to previous studies and our collected data, we described the duration of MV more than 24 h and ICU LOS more than 3 days as “prolonged.”14‐17 In our institution, the extubation criteria are fully awakened state, no neurological deficit, no massive bleeding with minimal vasopressor and inotropes usage (norepinephrine < 0.1 µg/kg/min or epinephrine <0.05 µg/kg/min), serum lactate below 2.5 mmol/L, normal blood gas analysis accomplished within less than 50% fraction of inspired oxygen (FiO2), normal chest x-ray, and adequate tidal volume respiration using pressure support ventilation of 8 cmH2O and positive end-expiratory pressure (PEEP) of 5 cmH2O.
Our institutional criteria of ICU discharge comprises stable condition (heart rate-to-age and blood pressure-to-age are found within 90%-95% percentile) and noticeable clinical improvement with only noninvasive ventilatory support at a maximum of 50% inspired oxygen, a maximum of two vasopressors usage (epinephrine <0.05 µg/kg/min OR dobutamine < 5 µg/kg/min AND milrinone 0.375 µg/kg/min), infused prostaglandin rate < 10 ng/kg/min or diuretics during weaning process, or ventilator-independent condition after insertion of tracheostomy cannula.
Statistical Analysis
The normal distribution of the variables was evaluated using visual (histogram and probability graphs) and analytical (Kolmogorov-Smirnov test and Shapiro-Wilk test) methods. A descriptive analysis was performed using frequency tables for the categorical variables. Mean and standard deviations were used to describe the normally distributed variables. Medians and ranges were used to describe the variables with a non-normal distribution. To assess differences between groups, the Mann-Whitney test or independent t test for continuous data and χ2 or Fisher exact test for categorical data were used in bivariate analysis. Variables with a P value <.25 in the bivariate analysis were included in the multivariable logistic regression analysis. Multivariable logistic regression analysis was performed to determine independent risk factors of prolonged ICU LOS and prolonged duration of MV. A P value of <.05 was considered statistically significant. All analyses were performed using IBM Statistical Package for the Social Sciences (SPSS) software (version 26.0).
Results
Over the six-year study period, 951 patients with a diagnosis of TOF underwent primary repair in our institution. Of those, 29 were excluded due to incomplete medical record data, leaving a total of 922 patients that were included in this study. Table 1 shows the demographic and characteristic data of the study population. The median age at the time of surgery was 49.65 months (range: 0-629 months). Additionally, the median weight was 12 kg (range: 2.7-84 kg), and the median weight-for-age percentile was <1 (range: <1->99). There were 506 males (54.9%) and 416 females (45.1%) in the study population. Six patients (0.7%) had Down syndrome, while the other 21 patients (2.3%) had residual lesions. The most frequent concomitant cardiac malformations were patent ductus arteriosus in 252 (27.3%), atrial septal defect in 116 (12.5%), and persistent foramen ovale in 59 (6.4%). The median CPB time was 104 min (range: 28-693 min), the median AOX time was 56 min (range: 13-256 min), the median MV duration was 16 h (range: 1-617 h), and the median ICU LOS was two days (range: 1-32 days). During the postoperative period, the median lactate level at 1 h after ICU admission was 2 mmol/L (range: 0.6-15.1 mmol/L). In this study, the most common adverse event was low cardiac output syndrome with an incidence of 13.1% (121 patients) then followed by a 6.2% (57 patients) incidence of JET. Table 2 compares the preoperative and intraoperative characteristics of patients with PMV (>24 h) and prolonged ICU LOS (>3 days) with the patients with duration of MV ≤24 h and ICU LOS ≤3 days.
Bivariate Analysis.
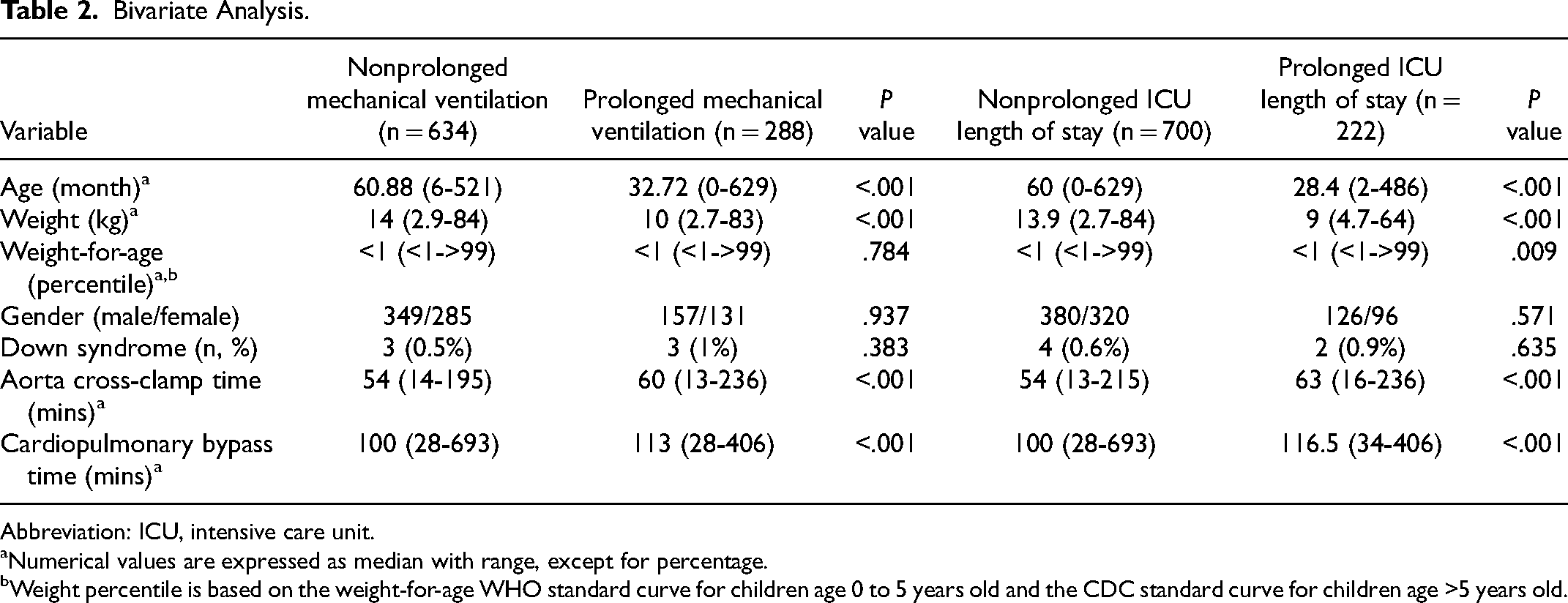
Abbreviation: ICU, intensive care unit.
Numerical values are expressed as median with range, except for percentage.
Weight percentile is based on the weight-for-age WHO standard curve for children age 0 to 5 years old and the CDC standard curve for children age >5 years old.
Patients with PMV who underwent surgical repair were younger (median: 32.72 months, range: 0-629 months) compared with patients without PMV (median: 60.88 months, range: 6-521 months, P < .001). There was also a significant difference in terms of weight in patients with PMV (median 10 kg, range: 2.7-83 kg) compared with the patients without PMV (median 14 kg, range: 2.9-84 kg, P < .001). Additionally, there was a significantly higher incidence of total residual lesions in the patients with PMV compared with those with a duration of MV ≤24 h (1.5% vs 0.7%, P = .001). Patients with PS-only and PR-only residual lesions were significantly more prevalent (0.4% vs 0.1%, P = .018, both lesions displayed the same value, respectively) in the PMV group (shown in Table 3). Table 3 also showed that severe PS and PR accounted for the statistically significant number of patients with both types of residual lesions in the PMV group (P value severe PS = .01, P value severe PR = .036). A number of patients with mixed residual lesions were found to be similar between PMV and non-PMV group (P = .319), predominantly consisting of mixed PS and PR. A similar pattern of VSD as a residual lesion was also discovered in both groups. Aortic cross-clamp and CPB time were different in the PMV group (median: 60 min, range: 13-236 min; median: 113 min, range: 28-406 min) compared with the non-PMV group (median: 54 min, range: 14-195 min; median: 100 min, range: 28-693 min). On multivariable analysis, age before 50 months, absolute weight below 12 kg, and presence of residual lesions were shown to be significant predictors of duration of MV as demonstrated in Table 4.
Crosstab Analysis of Residual Lesions Associated With Prolonged MV and ICU LOS.a
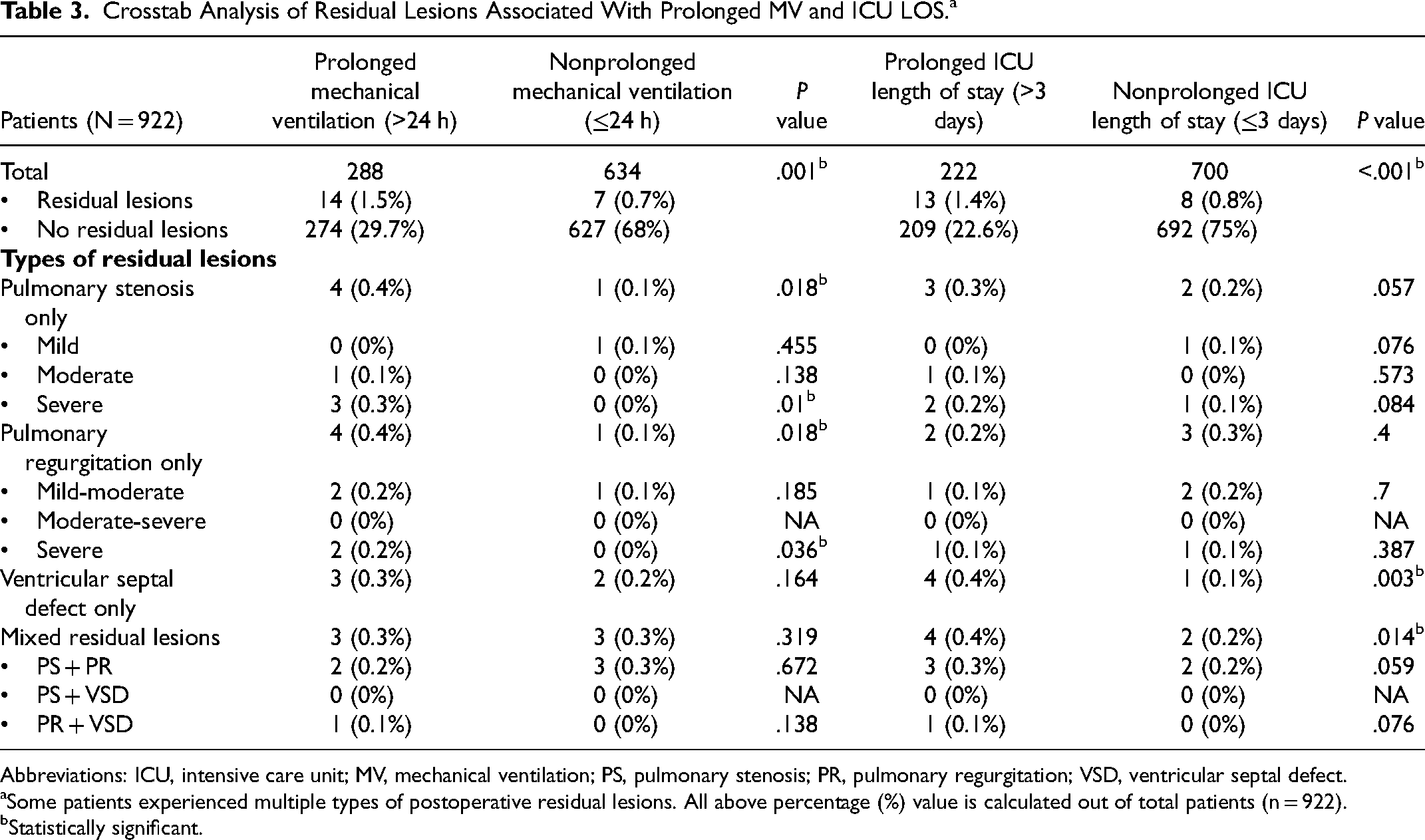
Abbreviations: ICU, intensive care unit; MV, mechanical ventilation; PS, pulmonary stenosis; PR, pulmonary regurgitation; VSD, ventricular septal defect.
Some patients experienced multiple types of postoperative residual lesions. All above percentage (%) value is calculated out of total patients (n = 922).
Statistically significant.
Multivariable Analysis of Factors Associated With PMV.
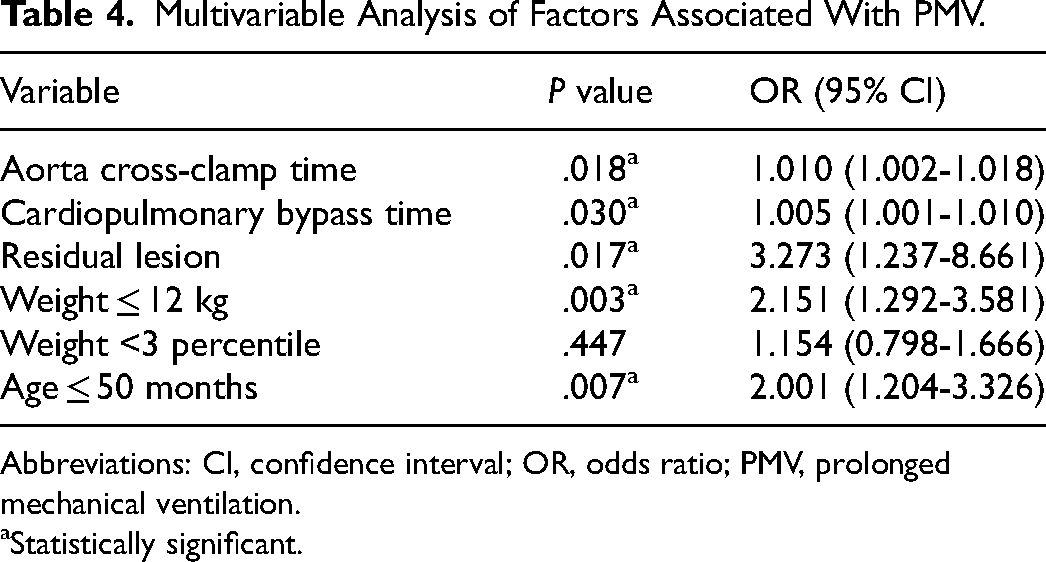
Abbreviations: CI, confidence interval; OR, odds ratio; PMV, prolonged mechanical ventilation.
Statistically significant.
Based on the definition of prolonged ICU LOS, a total of 222 patients (24%) had prolonged ICU LOS. These patients with prolonged ICU LOS underwent surgical repair at a younger age (median: 28.4 months, range: 2-486 months) compared with patients with ICU LOS ≤3 days (median: 60 months, range: 0-629 months, P < .001). Also, there was a significant difference in the weight of patients with prolonged ICU LOS (median 13.9 kg, range: 2.7-84 kg) compared with patients with ICU LOS ≤3 days (median 9 kg, range: 4.7-64 kg, P < .001). Additionally, there was a notably higher incidence of total residual lesions in the patients with prolonged ICU LOS (1.4% vs 0.8%, P < .001). Patients with prolonged ICU LOS have a greater total number of mixed residual lesions compared with those with non-prolonged ICU LOS (0.4% vs 0.2%, P = .014). The most frequent residual lesion in the mixed type was PS and PR. Moreover, VSD-only residual lesion was found to be significantly higher in the prolonged ICU LOS group (P = .003). Table 3 showed that PS-and PR-only residual lesion did not contribute to a higher risk of prolonged ICU LOS (P = .057 and .4, respectively). In addition, patients with prolonged ICU LOS also underwent a longer AOX and CPB time (median: 63 min, range: 16-236 min; median 116.5 min, range: 34-406 min) compared with patients with ICU LOS ≤3 days (median: 54 min, range: 13-215 min; median: 100 min, range: 28-693 min, P < .001, respectively). On multivariable analysis, age below 50 months, absolute weight less than 12 kg, underweight status, and presence of residual lesions emerged as significant predictors of prolonged ICU LOS as shown in Table 5.
Multivariable Analysis of Factors Associated With Prolonged ICU LOS.
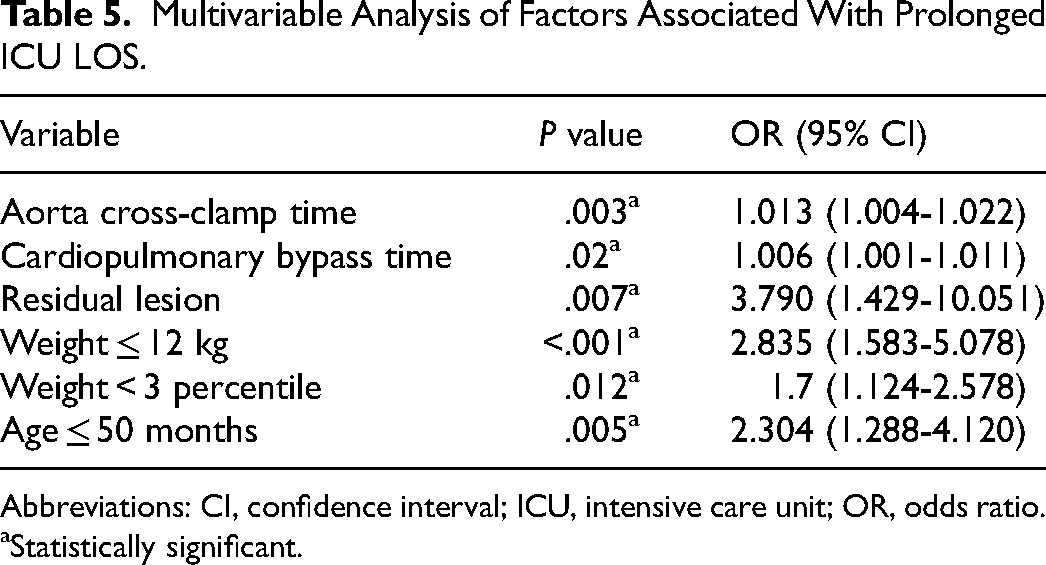
Abbreviations: CI, confidence interval; ICU, intensive care unit; OR, odds ratio.
Statistically significant.
Discussion
Prolonged MV and ICU LOS after TOF repair surgery in children is associated with high postoperative morbidity and mortality.14,18 The ICU LOS after TOF surgical repair in infants has been reported as six to seven days but less (median: two days) in this study.1,19 Based on the results, we identified several predictors for prolonged ICU LOS and PMV, such as age, nutritional status, weight, AOX time, CPB time, and residual lesion.
The presence of postoperative residual lesion has been considered one of the independent factors contributing to increased ICU LOS and risk of prolonged MV. Repair of RVOT using TAP through ventriculotomy was initially popular among pediatric cardiac surgeons in the 20th century. Yet, it yields higher risk and more severe PR, which is a risk factor for ventricular dilatation over time necessitating reintervention. As an alternative, the valve-sparing procedure allows the pulmonary annulus to grow and has been used on several TOF patients. However, this procedure carries the risk of residual PS. Based on the results in Table 3, PS-only lesion is more frequently found in patients with PMV, especially in severe cases. This finding, however, does not ignore the fact that PR-only lesion could also be found in a higher number of patients with PMV. Still, the intricate risk–benefit balance between those two aforementioned procedures, which may potentially form either lesion, must be carefully decided based on appropriate bias mitigation when assessing each patient. Significant residual lesions after congenital heart surgery have been found to be associated closely with prolonged ICU LOS and PMV in the Nathan et al study, 12 which conformed with our results showing that single PS- and PR-residual lesions increased the risk of PMV. The reasons why isolated PS and PR residual lesion may not significantly increase the ICU LOS are not entirely clear. However, it is important to note that the presence of other associated cardiac lesions or comorbidities may increase the risk of prolonged ICU stay regardless of the presence of isolated stenosis or regurgitation. The data stated that residual VSD has a higher risk of prolonged ICU LOS. It may be due to the potential complications associated with residual VSD, such as heart failure and arrhythmias. These complications can lead to hemodynamic instability, respiratory distress, and other medical conditions that require close monitoring and management in the ICU. On the other hand, residual VSD not having a significant effect on PMV could be because MV can be managed independently of the hemodynamic and respiratory effects associated with VSD. It is, therefore, primarily indicated for respiratory insufficiency, such as pulmonary edema, lung infections, or postoperative respiratory depression, which may or may not be directly related to VSD. 20 Mixed residual lesions do not exhibit significant differences in the prevalence of MV outcomes in both groups. This result is largely due to the type of mixed residual lesions consisting of mainly mild-to-moderate grade PS and PR.21,22 Additionally, studies evaluating the outcomes of 221 patients have suggested that the presence of these mixed residual lesions does not necessarily lead to PMV. 23 On the other hand, mixed residual lesions that include both PS and PR, especially related to grave complications such as hypoxia, arrhythmias, and hemodynamic instability, have been associated with prolonged ICU LOS. This finding conformed with a previous study evaluating the outcomes of 48 children that those who developed mixed residual lesions had significantly longer ICU lengths of stay than those without the mixed type of lesions. 24
In addition, our results showed that weight and age during operation are risk factors for PMV and prolonged ICU LOS after cardiac surgery, as mentioned in previous studies.4,7,18,25‐30 Another study of patients who underwent TOF surgical repair showed that ICU LOS and MV durations were prolonged in patients less than three months of age. 8 Neonatal and infantile age (especially younger than six months old) has been recognized as a significant predictor of PMV and prolonged ICU LOS.1,28,31 The contribution of the small thoracic cage to respiratory function, the relatively weak intercostal muscles, and the narrower airway in these age groups were shown to be the reasons for the risk of PMV resulting in prolonged ICU LOS. 31 Nevertheless, this finding does not indicate that postponing the timing of surgical repair would decrease overall morbidity or mortality. As noted in previous studies, definitive repair of TOF in patients older than 12 months has been shown to exhibit significant mortality. One of the reasons is that the abnormally stiffened diastolic expansion in the RVH is more prominent in older patients suffering from TOF, eventually impairing postoperative hemodynamic stability. 32 The timing of repair should be based on individual assessment within a multidisciplinary approach. 33 Lower absolute body weight was also a risk factor for PMV and prolonged ICU LOS, possibly associated with the aforementioned reason.30,34‐36
Being underweight in terms of nutritional status, as defined by less than three percentiles, served as a risk factor for prolonged ICU LOS but not PMV in this study. 37 The prevalence of being underweight is high in children with preexisting chronic disease, especially TOF, which therefore explained the low median data in the weight-for-age variable. Another study mentioned that being underweight is considered a prognostic factor in the ICU that requires implementation of an appropriate nutritional strategy, and thus its preadmission diagnosis must be taken into account. 38 The larger samples in our study may provide a different perspective compared to findings from other studies, suggesting that being underweight may have contributed to PMV and prolonged ICU LOS. For better identification and diagnosis of malnutrition related to underweight, using secondary anthropometric variables, such as middle upper arm circumference or body mass index to age, may render a more accurate prediction of risk factors related to nutritional status. 39
Shortened CPB and AOX time were found to be very likely trivial in minimizing the risk of prolonged MV and ICU LOS. Although both results mentioned statistically significant odds ratio toward MV (CPB, odds ratio [OR] = 1.005 95% confidence interval [CI] [1.002, 1.018]; AOX, OR = 1.01 95% CI [1.002, 1.018]) and ICU LOS (CPB, OR = 1.006 95% CI [1.001, 1.011]; AOX, OR = 1.013 95% CI [1.004-1.022]), the range of both confidence intervals is very near to the value of one. This implied that CPB and AOX time may exhibit minimal clinical effect on duration of MV and ICU LOS. 40 In one study, CPB and AOX times were not significant risk factors associated with PMV.29,41 Conversely, other studies have mentioned their close relation to early extubation and ICU LOS. 25 Inconclusive results from multiple previous studies may reinforce the finding that both variables exhibited as irrelevant clinical predictors to prolonged MV and ICU LOS in this study.
Limitations
This retrospective study has several limitations. First, it is a retrospective, single center study where human factors during surgical intervention and postoperative management cannot be clearly identified. Secondly, the analysis of the predictors of PMV and prolonged ICU LOS may be performed in different ways. The risk factors associated with PMV and ICU LOS could vary across different centers. Besides, the presence of conflicting data shows that complex systemic and cardiopulmonary interactions contribute to this issue and it is impossible to have a universal list of risk factors for this multifactorial phenomenon. Moreover, the population that we studied in Indonesia has specific considerations due to the relatively late presentation of CHD and undernutrition status.
Conclusion
In this study, we found that the presence of residual lesion, age, and weight are risk factors for prolonged MV and ICU LOS. Anthropometric status (stated in weight-for-age percentile), however, is considered an independent predictor of prolonged ICU LOS but not of PMV. These factors should be taken into consideration when deciding time of surgery and in providing postoperative care in the ICU. Lastly, taking these factors into consideration may allow an optimal outcome following TOF corrective surgery.
Footnotes
Abbreviations
Acknowledgments
This work was supported by Universitas Gajah Mada [grant no. 3550/UN1.P.III/DitLit/PT.01.05/2022].
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.