
Abstract
Atrioventricular septal defect (AVSD) with shunting restricted to the ventricular level is a rare form of AVSD. To our knowledge, this shunting pattern has not been reported in AVSD with tetralogy of Fallot. We report a child with this unusual combination who underwent a successful single-stage repair at two years of age.
Introduction
The phenotypic feature of atrioventricular septal defects (AVSDs) is the commonality of the atrioventricular junction, with associated unwedging of the aortic outflow tract relative to the common junction. 1 In the most common variant, the bridging leaflets float within the septal defect, permitting shunting at both the atrial and ventricular levels. In some instances, the interventricular component of the defect extends toward the outlets of the ventricular mass, with malalignment of the outlet septum resulting in subpulmonary outflow obstruction, thus producing the combination with tetralogy of Fallot. Attachment of the bridging leaflets to either the crest of the ventricular septum or the leading edge of the atrial septum can restrict the potential for shunting to the atrial or ventricular levels, respectively. We describe here a child with the combination of AVSD and tetralogy in whom shunting was restricted to the ventricular level and discuss the surgical management. As far as we know, exclusively ventricular shunting has not previously been reported in this setting.
Case Report
A two-year-old boy was referred to us with a history suggestive of cyanotic spells, motor developmental delay, and suboptimal weight gain. His baseline saturation was 70%. Ultrasonic interrogation revealed usual arrangement of the abdominal organs. The systemic and pulmonary venous connections were normal. There was a small defect across the oval fossa but no evidence of a persistent primary atrial foramen (Figure 1 and Video 1). There was, nonetheless, a common atrioventricular junction, guarded by a common atrioventricular valve which was of “Rastelli type C” morphology; the superior bridging leaflet being attached to a papillary muscle supported by the right ventricular free wall (Video 2). The ventricular mass showed right-handed topology. There was a large ventricular component of the septal defect extending from the crux of the heart to the subaortic area. The crest of the muscular ventricular septum was overridden by the aortic trunk (Figure 2), with severe narrowing of the pulmonary outflow tract due to malalignment of the muscular outlet septum, along with additional narrowing at the level of the pulmonary valve (Video 3). The aortic arch was left-sided, with normal branching of the brachiocephalic arteries. There was no focal narrowing of the right and left pulmonary arteries.
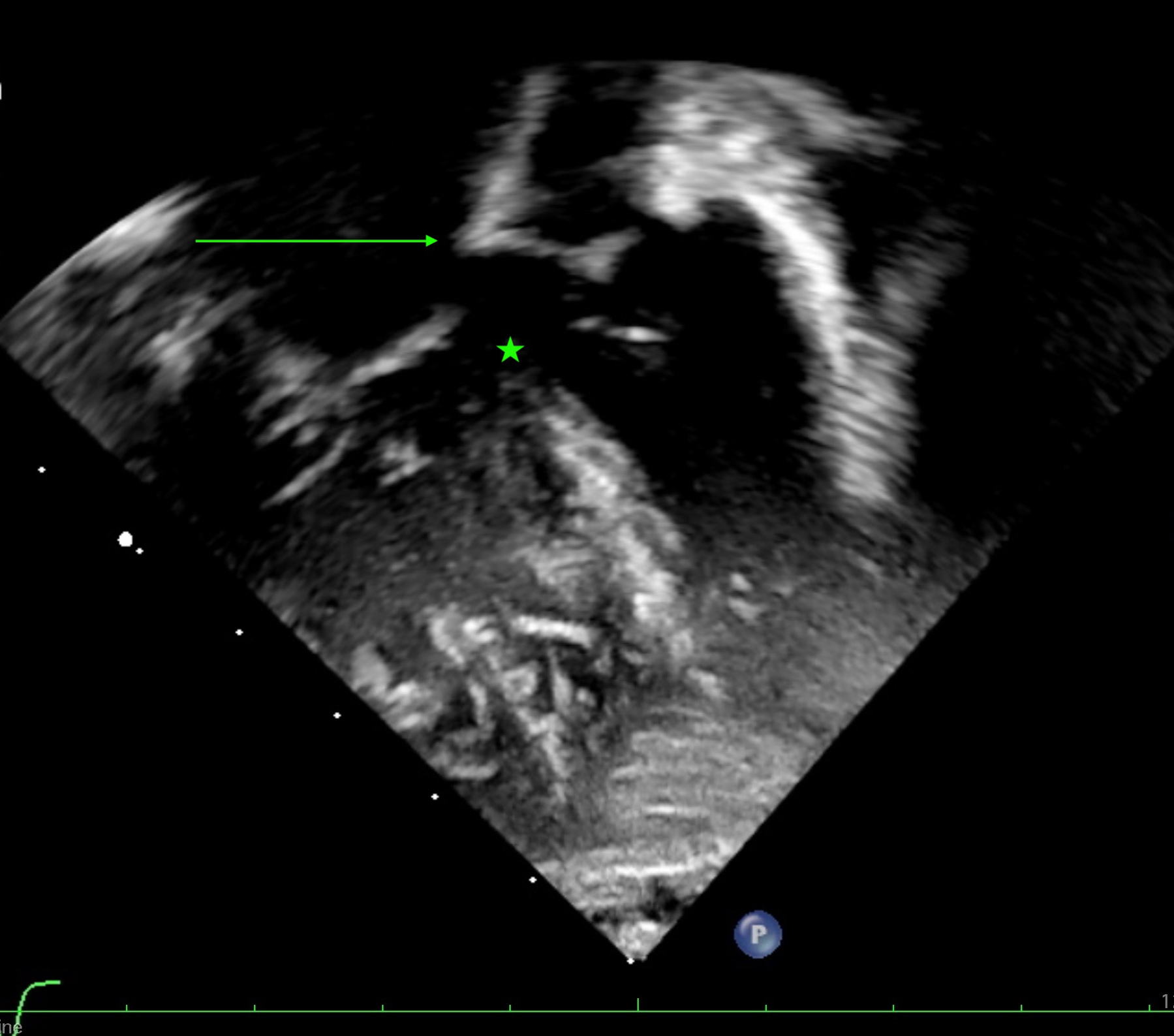
Echocardiographic image from a modified apical 4-chamber view. The atrioventricular leaflets are attached to the leading edge of the atrial septum with no primary atrial foramen (arrow). There is a large ventricular component of the septal defect (star).
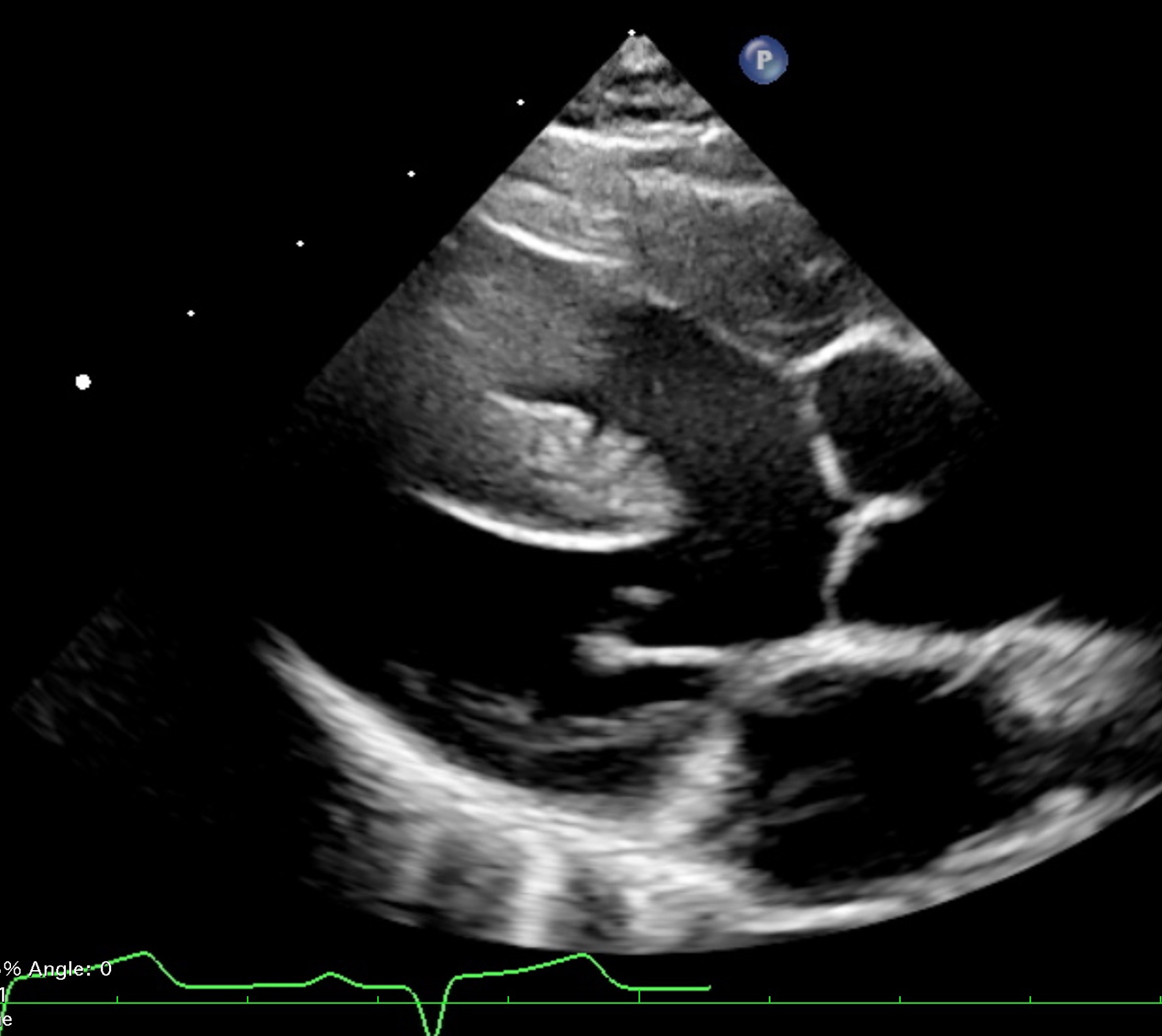
Echocardiographic image from a parasternal long axis view demonstrating the aortic trunk overriding the muscular ventricular septum.
Our diagnosis was AVSD combined with tetralogy of Fallot, but unusually with shunting across the septal defect confined at the ventricular level. The patient underwent a single-stage repair. The defect in the oval foramen was enlarged to provide better visualization of the left component of the common atrioventricular valve. The ventricular shunt was closed with a pericardial patch. The zone of apposition between the left ventricular components of the bridging leaflets was approximated using multiple interrupted sutures. The enlarged atrial communication was then closed with a pericardial patch. The right ventricular outflow tract was opened below the pulmonary valve, permitting excision of the hypertrophied septoparietal trabeculations. The diameter of the pulmonary root was enlarged with a transannular patch. Recovery from the surgery was uneventful. At review one month after the surgery, the ventricular function was normal, and there were no residual shunts. On subsequent review one year after the surgical repair, there was mild incompetence on both sides of the repaired common atrioventricular valve.
Discussion
In recent years, it has become recognized that a wide spectrum of disorders can be united under the umbrella of the commonality of the atrioventricular junction, this being the phenotypic hallmark of AVSDs. 1 Rare variants include the associations with the common arterial trunk 2 and intact septal structures. 3 The association with tetralogy of Fallot is not so rare. 4 Usually, this combination is associated with extensive commitment of the superior bridging leaflet to the right ventricle, the Type C variant in the Rastelli classification. In previously described cases, the extensive shunting at the ventricular level anticipated with this morphology has also been associated with shunting at the atrial level through the “primum” defect.
It is also recognized, nonetheless, that on occasion individuals can have an AVSD, but with shunting confined at the ventricular level because of the attachment of the bridging leaflets to the leading edge of the primary atrial septum, thus obliterating the “primum” defect. In terms of the level of shunting, this is the rarest variant found with an AVSD. Adachi and colleagues found this variant in five hearts among the 86 hearts with AVSD held in the archives of the Royal Brompton Hospital. 5 They did not observe any superior extension of the ventricular communication in these specimens, suggesting that such superior extension may not be possible when the bridging leaflets are attached to the underside of the primary atrial septum. Our experience now shows that the combination does exist.
The combination of AVSD with tetralogy of Fallot is now well recognized as a distinct surgical entity, with repair having been performed from the 1980s. 6 This combination is usually associated with Trisomy 21, with some cohorts reporting trisomy in up to 95% of afflicted individuals. 7 Our child, however, did not have any clinical evidence of a chromosomal abnormality. In the twentieth century, surgical repair was often performed in a staged manner, beginning with construction of a systemic-to-pulmonary arterial shunt. With increasing surgical experience, and advancement of intensive care at the beginning of the twenty-first century, primary repair will now be the choice of most congenital cardiac surgeons, with anticipation of excellent outcomes. 8 Controversy remains, nonetheless, regarding the need for a transannular patch to enlarge the pulmonary outflow tract, and the necessity of maintaining pulmonary valvar competence. 9 Our repair using a transannular patch resulted in free pulmonary incompetence. The child, nonetheless, tolerated this very well, and the postoperative recovery was uneventful.
To the best of our knowledge, shunting restricted exclusively at the ventricular level has not previously been reported when AVSD has been associated with tetralogy of Fallot. Our experience suggests that the combination can still be repaired in a primary fashion with a good early postoperative outcome, even when there is severe pulmonary incompetence.
Footnotes
Authors’ Statement
Consent was obtained from the parents of the child to publish the clinical details of this case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.