
Abstract
Keywords
Background
In 2015, the United Nations (UN) adopted the Sustainable Development Goals (SDG) with a specific focus to end preventable deaths in children under-5 and reduce premature mortality from noncommunicable diseases by one-third through prevention and treatment by 2030. 1 Despite much progress, the world has struggled to reach this goal with 5.3 million children dying before their fifth birthday as of 2018. Per the UN report, Sub-Saharan Africa continues to have the highest rate of under-5 mortality with one in five children dying before the age of five, which is 16 times higher than the average in high-income countries (HIC). 1 Although advances in technology and access to care have led to dramatic decreases in pneumonia, diarrhea, and measles; efforts to reduce mortality due to congenital defects, such as cardiac, continue to be slow. 2
The Global Burden of Diseases, Injuries and Factors Study estimated the global prevalence of congenital heart disease (CHD) to be 1.8 per 100,000 live births and the cause of over 260,000 total deaths, including more than 180,00 infants under the age of one. Over the last 30 years, infant mortality related to congenital heart defects has decreased by 60% in high sociodemographic index countries, but only minimally in low-resource countries. 3 The initial goal of cardiac surgery was to correct CHD and valve dysfunction as a result of rheumatic heart disease (RHD). However, compiled survey results of 13 low- and middle-income countries (LMIC) and three HICs suggest that an epidemiological transition from CHD to later occurring degenerative heart disease occurs with improved economic status. 4 It is estimated that 4% of childhood deaths in the year 2030 will be due to congenital anomalies 2 with congenital heart defects as the largest preventable cause. 5 This suggests that surgical capacity building is a relevant and important area of focus to address SDG 3 to ensure healthy lives and promote well-being at all ages.
Nurses play an integral part in the postoperative management of pediatric cardiac surgery patients. Research has shown that higher levels of pediatric critical care nursing experience and education are instrumental in decreasing patient deaths and improving postoperative outcomes.6–8 However, a review of the literature shows a paucity of training in cardiac critical care developed for nurses in LMIC. In addition, nursing education provides an opportunity for women to advance their careers, increasing gender equality in medicine. Women make up most of the health sector workforce, including 90% of nursing personnel, but they are underrepresented at the senior management level. 1 In the All-Party Parliamentary Group on Global Health's report entitled Triple Impact: How developing nursing will improve health, promote gender equality and support economic growth, they identify one of the main obstacles for nurses is access to high-quality education, training, and continued professional development. 9 As a result, nurses leave their communities, which disadvantages the most resource-limited environments.
In 2020, the under-5 mortality rate was over 48.7 per 1,000 children in Ethiopia with just under 70,000 nursing personnel in the country. 10 While there are limited data on the overall disease burden of heart disease in children in Ethiopia, a 2017 cross-sectional study of six referral hospitals in Ethiopia, found the most common cardiac pathology was RHD followed by CHD. Of the patients with congenital heart defects, 35% had ventricular septal defects, 21% had atrial septal defects, 18% had patent ductus arteriosus, and 7% had tetralogy of Fallot. 11 The anatomic lesions of CHD are consistent across populations; however, critical lesions and those lesions which are associated with death in the neonatal period are underrepresented in this cohort. This is similar across multiple low-resource countries working to improve outcomes in CHD.3,4
The Federal Democratic Republic of Ethiopia Ministry published a Health Sector Transformation Plan in 2015 analyzing the overall health system and outlining strategic plans for the future. In their analysis, they acknowledged weaknesses in the distribution of skilled human resources, suboptimal service availability and readiness at health facilities, and suboptimal quality of care as problems within the Ethiopian healthcare system. They also recognized the importance of training skilled healthcare workers to increase capacity. 12 As a result of this identified need and interested nurses at the Children's Cardiac Center of Ethiopia, we implemented a Pediatric Cardiac Critical Care Curriculum and evaluated the impact on nursing knowledge. Our goal was to increase nursing knowledge and improve clinical outcomes for pediatric patients undergoing cardiac surgery.
Methods
We conducted a prospective cohort study to evaluate the effectiveness of a cardiac critical care curriculum on the knowledge of nurses working at the Children's Cardiac Center of Ethiopia. The Children's Cardiac Center of Ethiopia is a nongovernmental organization that was established in 2009 by pediatric cardiologist Dr Belay Abegz.
Twenty-five cardiac critical care nurses volunteered to participate in our curriculum. All nurses who participated worked in the cardiac critical care unit at the Children's Cardiac Center of Ethiopia. Nurses from other departments were not included in this cohort. Nurses completed a 15-h “Cardiac Core” curriculum adapted specifically for low-resource settings over the course of three months (July 2020 to October 2020). The curriculum was delivered via a remote didactic education platform and recorded in the cloud for nurses to review and to allow for asynchronous learning. Lectures were devoted to four specific domains: anatomy and physiology, pharmacology, transitional physiology, and both preoperative management and optimization, and postoperative management. The remote didactic education sessions were given by a multidisciplinary group of experts including nurses, cardiac nurse practitioners, respiratory therapists, pharmacists, and physicians across multiple disciplines including critical care, cardiac critical care, and cardiology from the University of Maryland Medical Center Cardiac Intensive Care Unit (CICU) and Heart Center. Each lecture was approximately 90 min, with two lectures given once per week for five weeks, inclusive of a review session. A dedicated nurse course director was available during all lectures for questions and review. An Ethiopian nurse was identified as the point of contact and facilitated bidirectional communication.
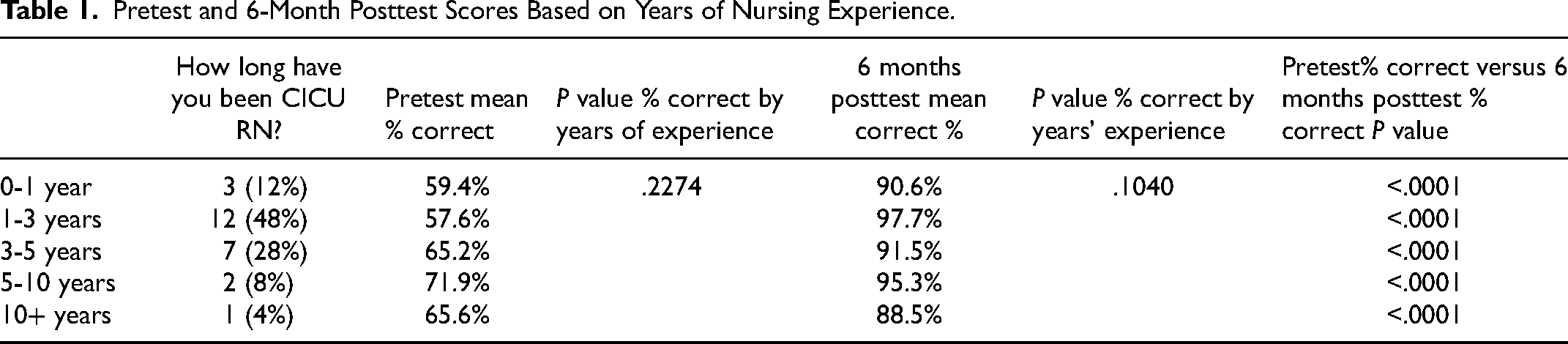
Our primary outcome measures were (1) the effect of the curriculum on improving nursing knowledge, and (2) assessing knowledge retention over time. Participants were asked to complete a multiple-choice test to assess their baseline cardiac knowledge prior to participating in the curriculum (pretest), followed by subsequent tests after completing the educational curriculum (posttests) at a number of intervals including: immediately after completion, one-month, three-month, six-month, and 12-months after completion. We used this pre- and posttest model to measure baseline nursing understanding, knowledge acquisition after completion of the curriculum, and knowledge retention. The pre- and posttest had different but matched questions. The questions on each posttest were identical. Nursing subjects completed a demographic survey that included years of nursing experience in general and specifically in the CICU (Table 1). In addition, subjects completed a feedback survey to assess their subjective experiences with the curriculum and to share general feedback.
Pretest and 6-Month Posttest Scores Based on Years of Nursing Experience.
Descriptive statistics were performed to describe demographic data including years and type of nursing experience. Questions were grouped into four specific categories related to the curriculum for analysis: (1) Pharmacology, (2) Anatomy/Physiology, (3) Preoperative Management, and (4) Postoperative/Transition Management. Chi-square testing was performed to compare test scores (percentage correct) between the different categories and over time. Analyses were performed using SAS 9.4.
Results
A total of 25 nurses completed the pretest and participated in the curriculum. All 25 nurses completed the immediate posttest as well as the posttests at one month, three months, and six months after the curriculum. Twenty-one of the subjects (84%) also completed the 12-month posttests. The majority of nurses had between one and three years of cardiac critical care experience (Table 1). Of our participants, 72% (n = 18) had worked with an international team previously, but only 24% (n = 6) had participated in a critical care curriculum. In addition, 44% (n = 11) had used remote didactic education before, 80% (n = 20) had smartphones, and 60% (n = 15) had a stable internet connection at home.
We found that years of nursing experience significantly impacted pretest scores (P = .03) (Table 1). After completing the curriculum, subjects at each level of nursing experience significantly improved their posttest score (all P ≤ .0011), but there was no longer a significant difference based on years of experience (P = .3298). Interestingly, years of cardiac intensive care unit nursing experience did not significantly impact pretest or posttest scores, although subjects at each level of experience showed significant improvement in knowledge (P < .0001 for all).
The percent of correct answers improved significantly from pretest to immediate posttest in all of the four categories: (1) pharmacology (from 35.4% correct to 84%, P < .0001); (2) anatomy and physiology (61.5%-98.5%, P < .0001); (3) preoperative care (71.6%-97.7%, P < .0001); and (4) postoperative care (72.8%-96.8% P < .0001). Repeat posttest scores at one month, three months, six months, and 12 months continued to be significantly improved from the pretest (P < .0001 for pretest vs each posttest interval), and demonstrated continued high percent of correct scores, indicating excellent knowledge retention over time (Table 2, Figure 1).
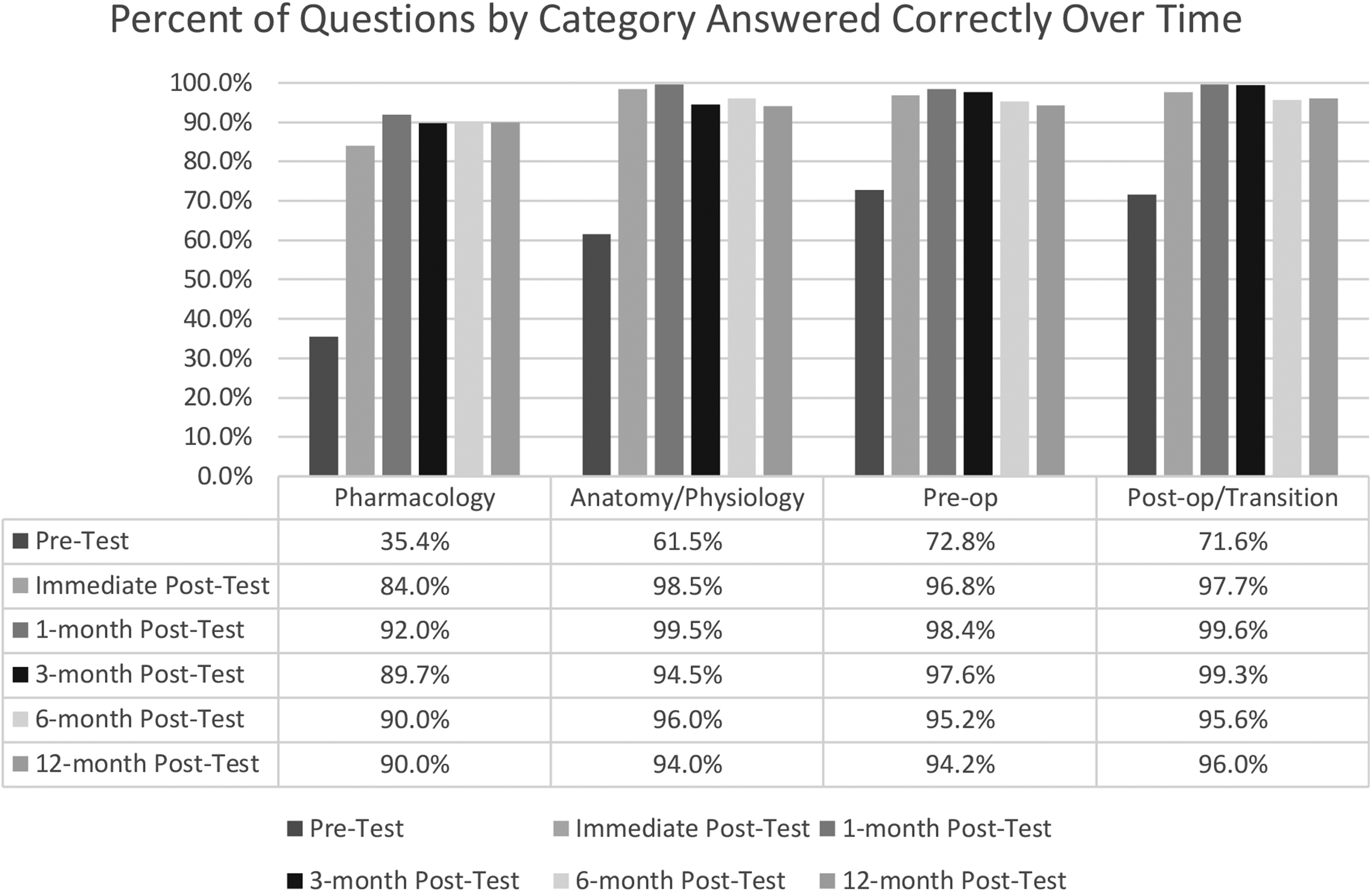
Percent of questions by category answered correctly over time: Percent of questions answered correctly by nurses completing “Cardiac Core Curriculum” at the pre- and immediate post-test and 1-, 3-, 6-, and 12-months post curriculum.
Pretest and Posttest Scores by Category.

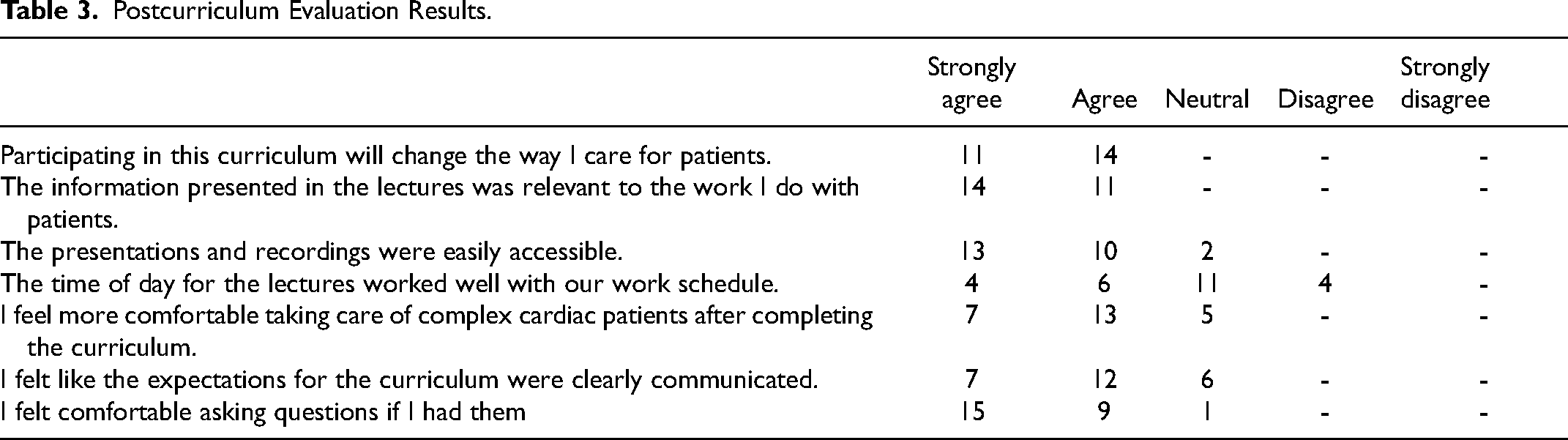
Nursing feedback on the curriculum was generally positive as shown in Table 3. All of the nurse participants (n = 25) agreed or strongly agreed that participating in this curriculum will change the way they care for patients and that the information presented in the lectures was relevant to the work they do with patients (Table 3). When asked if they felt more comfortable taking care of complex cardiac patients after completing the curriculum, 25% strongly agreed, 54.2% agreed, and 20.8% felt neutral about this statement. When nurses were asked about lecture accessibility, 54.2% strongly agreed, 37.5% agreed, and 8.3% felt neutral that the lectures were easy to access. Over 16% strongly agreed, 20.8% agreed, 45.8% felt neutral, and 16.7% disagreed that lecture time was convenient. Seventy-five percent of nurses strongly agreed or agreed that expectations about curriculum were clear, while 25% felt neutral. Over 95% of nurses strongly agreed or agreed that they felt comfortable asking questions, while 4% felt neutral about asking questions. Most importantly, 100% of nurses would recommend that other nurses participate in this curriculum.
Postcurriculum Evaluation Results.
Conclusions
Approximately one in 400 live births will require surgical repair of a cardiac defect. 4 Surgical intervention for CHD requires significant resources and an extensive healthcare infrastructure with staff trained to care for patients with these conditions. Research has shown that as the specialized surgical workforce increases, congenital heart surgery mortality decreases. 2 This is further supported by data from the United States suggesting that early intervention and skilled surgical repair have significantly increased survival in patients with d-transposition of the great arteries, complete atrioventricular septal defect, and hypoplastic left heart syndrome. 13 Unfortunately, many children in LMIC may present for evaluation later due to the inability to diagnose CHD prenatally, lack of critical congenital heart screenings, and limited availability of echocardiograms. 14 These patients frequently experience higher rates of complications than those who were identified earlier, highlighting the importance of a strong, well-trained interdisciplinary team.
Multiple groups have attempted to address the discrepancies in access to treatment for children with CHD in a variety of ways.15–17 A 2014 retrospective cross-sectional study surveying 21 countries, reported that there was one surgeon for every 25 million people in Sub-Saharan Africa, and the majority of cardiac surgeries were being performed by visiting teams via intermittent mission work. 15 While these types of interventions can address the short-term needs of a limited number of patients and lesions, the ability to equip the local teams with the knowledge, technical expertise, equipment, and staffing is limited and not sustainable. Thus, there has been a shift to develop more collaborative relationships between local and visiting teams and to focus on education as a route to sustainability, capacity building, and the creation and maintenance of local expertise.
There are multiple thoughts on what a long-term, sustainable partnership can look like. One study outlines important components of sustainable international collaboration and surgical planning including an infrastructure evaluation, patient assessments, and a team-based peer-modeling approach where visiting clinicians work in concert with local counterparts. 16 Another elaborates on three models used to develop programs for low-resource sites in need of improving the local capacity building to provide critical resources for the improvement of outcomes in low-resource settings in multiple domains. The domains discussed are human resources capital, supply chain management, training paradigms, and outcome assessments as well as basic preoperative optimization and postoperative care. These models include the intermittent visit model where international teams visit a hospital in an LMIC for 1 to 4 weeks through a year; resident senior surgeon model where a senior retired surgeon or surgeon dedicated to humanitarian work lives in an LMIC for multiple years; and the team in residence model where a team of specialists maintains residence in an LMIC for 1 to 2 years almost continuously. Mentorship and ongoing education are cornerstones to the models ultimate success in recognizing the importance of nursing education and empowerment. 17 Many of these models focus on the needs for surgery, while other studies advocate for a focus on cardiac critical care training to improve clinical outcomes of patients. 14
Our study shows that remote learning is a reasonable practice and strategy to support capacity building in global health. Our intervention demonstrates that remote learning via an online platform is not only effective at increasing nursing knowledge but it is also effective at ensuring that new knowledge is retained overtime. Several authors, including Shao et al, Kovacevic et al, and Schmidt et al, have written that internet-based education and simulation instruction are as effective as traditional models, especially given the wide acceptance of remote education as a tool for disseminating new knowledge, and that the learning effect persists over time.18–22 Further, our model is consistent with several best practices in internet-based learning access, bidirectional development of goals and objectives, balance between synchronous and asynchronous learning, and effective assessment tools. 23
With regard to access, remote didactic education was utilized because it requires little upfront cost and is low bandwidth. There was no cost for learners and they were able to access all resources via Wifi in the hospital or individual devices such as tablets and phones on 3G and 4G cellular signals. Goals and objectives were developed in a bidirectional, multidisciplinary manner such that all participants in the study understood—learners and teachers—the proposed outcome of the intervention and were aware of how the assessment of new knowledge would match the teaching elements. There was also a well-balanced strategy between asynchronous and synchronous learning. All materials, including recorded lectures, library of resources and materials, and print versions of all lectures were made available. This also included scheduled debrief and feedback sessions to evaluate teaching effectiveness, to ask questions and clarifications, and to engage in practical discussions of the implementation of new knowledge into clinical practice. Lastly, the assessment model of pretesting and posttesting ensured effective information delivery. In pretesting, both learners and teachers were aware of knowledge gaps before content delivery which allowed for a more transparent and proscriptive development of content. Whereas serial posttesting over time ensured that the expected drop-off in knowledge was not as severe.
In their 2020 report, the UN acknowledged the impact that COVID-19 could have on reversing the progress made to reduce maternal and child mortality. 1 The limitations imposed by the pandemic on travel, funding, and available resources highlighted the importance to reimagine international collaborations. While open-access online communities for sharing resources existed prior to the pandemic, the use of online communication platforms in medical education has increased during this time frame.25–27 Most of these efforts have focused on students or trainees in high-resource settings; and, the data are heterogeneous as compared to traditional teaching models with regard to the acquisition of new skills and behaviors and effect of patient care, 19 but are effective in gaining and maintaining new knowledge.18–20,23 Few have addressed the ongoing professional development of certified healthcare professionals—especially in pediatric critical care and pediatric cardiac critical care. This platform has the opportunity to address barriers in low-resource settings given limited staffing, limited access to continuing medical education, and limited access to resources. We also acknowledge that the limited online training readily available for cardiac critical care nurses is not specific to the LMIC context.
Our study is easily reproducible in a variety of different environments and allows learners to engage with a multitude of experts in various specialties irrespective of location. Previously cited models require experts to travel from one location to another, which can be very time intensive.16,17 Our intervention allows experts to connect with learners for 1 to 2 h over a virtual platform and provides the flexibility for them to return to their clinical duties after online training. This allows for increased exposure to a diverse group of specialists that may not have been included in global health trips traditionally. Furthermore, lectures are delivered in real time, which allows nurses to ask specific questions and engage in discussions about local challenges with topic experts, fostering a bidirectional partnership. In the setting of internet shortages or power loss, lectures are uploaded to the cloud for viewing at a time convenient for the learner.
Most importantly, it is a decolonial approach to global health in that one group is not occupying another's space and the focus is on enhancing local expertise. Our intervention was inspired by the interest of a surgeon and critical care nurses at the Children's Cardiac Center of Ethiopia to increase their knowledge with the hopes to increase clinical capacity and improve clinical outcomes. The curriculum was curated to the specific needs of the group and discussions were specific to the context and obstacles faced by the learners, who were working in the cardiac critical care unit simultaneously. In addition, it also encouraged the University of Maryland Children's Hospital Pediatric Critical Care team to think about different clinical situations and challenges which will positively impact their own clinical practice.
Our intervention was limited by multiple factors. It focused on a group of cardiac critical care nurses at one pediatric CICU in Ethiopia. Ideally, this intervention would be studied within multiple hospitals and in multiple locations to evaluate generalizability to other environments and this will be the focus of future research. In addition, we evaluated nursing knowledge measured using a pre- and posttest model. The posttests were not identical to our pretest and while questions were matched for topic, there may be some variability in how participants interpreted the wording of different questions. Although all participants were self-described as being fluent in English, it is important to recognize the impact of language selection on outcomes in education. Our ability to study the impact on our remote curriculum on clinical outcomes as well as our ability to conduct the proposed next step of simulation education and practice was limited by the restrictions placed on pediatric cardiac surgery during the COVID-19 pandemic as well as political upheaval in a country that limits access to the internet. In the future, we hope to evaluate the continuation of our curriculum on patient outcomes. We believe our educational intervention is a feasible, useful, and sustainable model that can and will be practiced even after the pandemic restrictions are lifted.
Supplemental Material
sj-pdf-1-pch-10.1177_21501351231186419 - Supplemental material for Remote Didactic Education Effectively Increases Cardiac Critical Care Nursing Staff Knowledge in Low-Resource Settings
Supplemental material, sj-pdf-1-pch-10.1177_21501351231186419 for Remote Didactic Education Effectively Increases Cardiac Critical Care Nursing Staff Knowledge in Low-Resource Settings by Tamara Kliot, Adrian Holloway, Katherine Spillman, Julianne Moss, Natalie Louise Davis, Abebech Ayalew, Adnan Bhutta and Yayehyirad Mekonnen Ejigu in World Journal for Pediatric and Congenital Heart Surgery
Supplemental Material
sj-pdf-2-pch-10.1177_21501351231186419 - Supplemental material for Remote Didactic Education Effectively Increases Cardiac Critical Care Nursing Staff Knowledge in Low-Resource Settings
Supplemental material, sj-pdf-2-pch-10.1177_21501351231186419 for Remote Didactic Education Effectively Increases Cardiac Critical Care Nursing Staff Knowledge in Low-Resource Settings by Tamara Kliot, Adrian Holloway, Katherine Spillman, Julianne Moss, Natalie Louise Davis, Abebech Ayalew, Adnan Bhutta and Yayehyirad Mekonnen Ejigu in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.