
Abstract
We report a case of a one-year-old boy with tetralogy of Fallot, who was preoperatively diagnosed to have an associated systemic venous anomaly. Computed tomography confirmed the absent superior vena cava, and the case was managed with an appropriate cannulation strategy. Preoperative diagnosis and thorough planning of this rather benign anomaly were imperative for the successful outcome of this case. Clinical and surgical implications of this anomaly are discussed in this report.
Introduction
Congenital anomalies of the superior vena cava (SVC) are fairly common and coexist with other congenital cardiac anomalies; the most common being bilateral SVC. Both bilateral SVC and isolated left SVC can occur in the otherwise normal heart or be associated with congenital heart disease. 1 If the left SVC drains into the right atrium, venous blood return into the heart is normal. For this reason, many of these SVC anomalies are asymptomatic and found incidentally. We report a unique case of absent SVC in a case of tetralogy of Fallot (TOF) and discuss the cardiopulmonary bypass strategies.
Case Report
A one-year-old boy (weight 8 kg; saturation 76%) who was cyanotic since two months of age presented to our institution. Transthoracic echocardiography showed TOF with suspicion of anomalous systemic venous return. Computed tomography (CT) identified absent bilateral SVCs. Both right and left brachiocephalic veins continued as the azygos and hemiazygos veins respectively. The veins, formed a common confluence below the diaphragm at T9 level and drained into the inferior vena cava (IVC) (Figures 1A and B and 2). Intracardiac diagnosis was TOF with an adequate pulmonary annulus and branch pulmonary arteries.
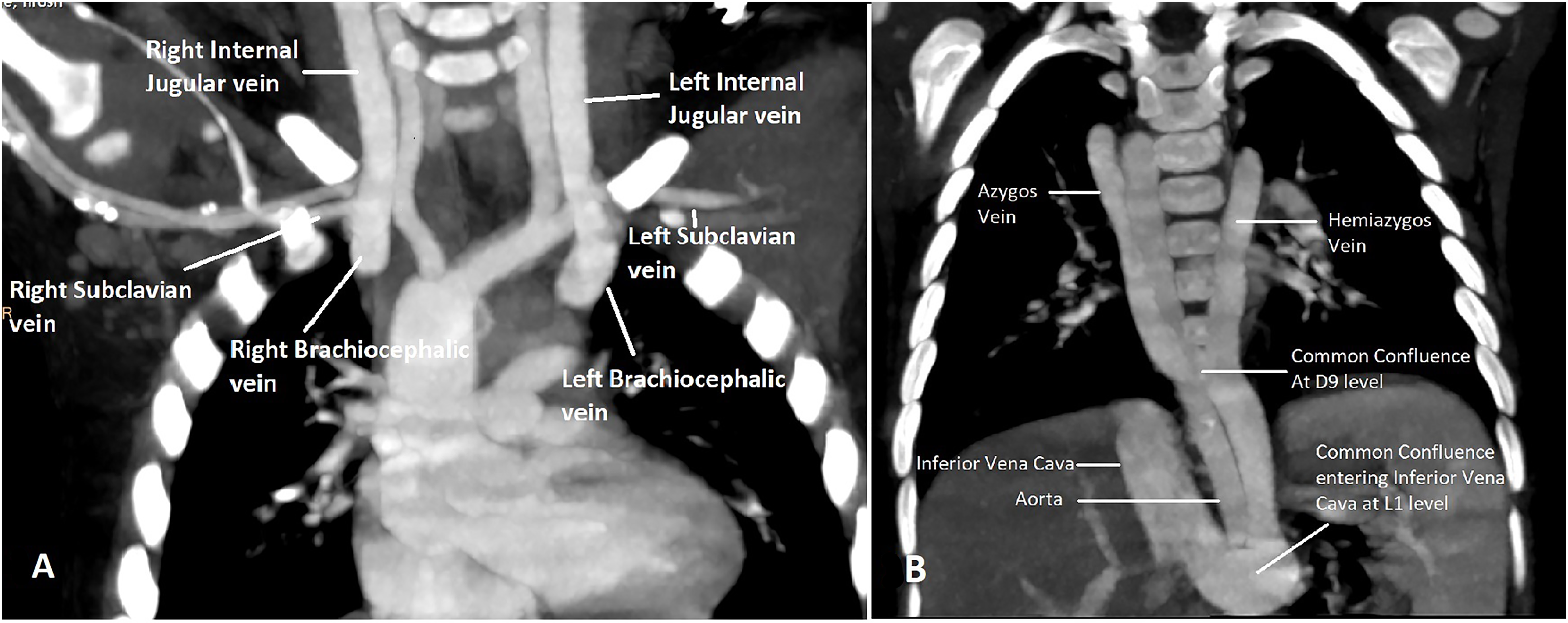
(A and B) Computed tomography (CT) image showing bilateral brachiocephalic veins draining through the azygos and hemiazygos veins and uniting to form a common confluence at T9 level, going vertically below the diaphragm (posterolateral to the left of the aorta) and uniting with the infrahepatic inferior vena cava above the renal vein at L1 level.
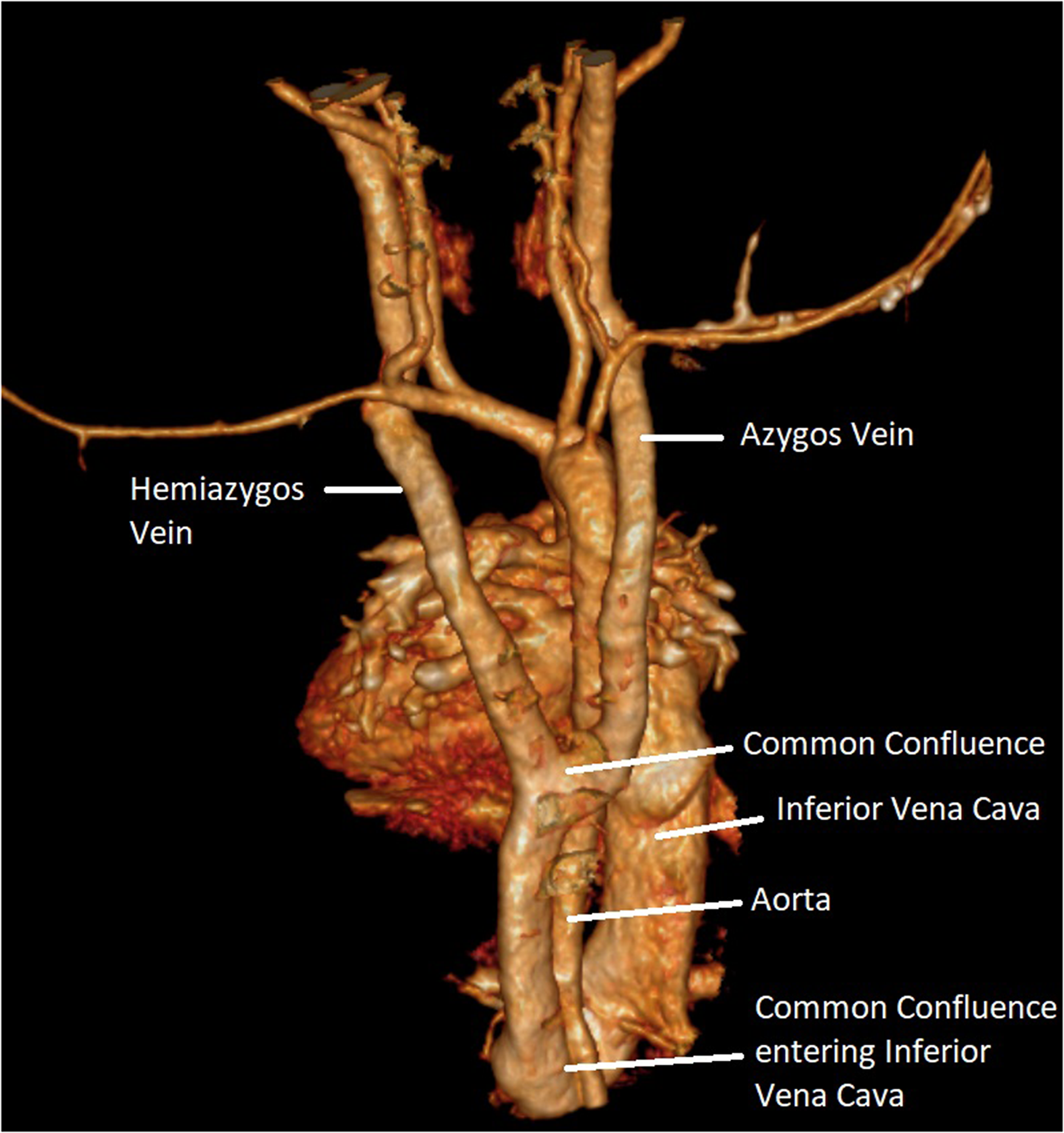
3D reconstructed computed tomography (CT) image showing the same patient in Figure 1 from the posterior view.
He was taken to the operating room for intracardiac repair via median sternotomy. Standard cardiopulmonary bypass was initiated via aortic cannulation and single straight IVC cannula (24F) for venous drainage with moderate hypothermia. Ventricular septal defect closure and right ventricular outflow tract resection were done via the transatrial approach. The pulmonary valve was preserved, and the main pulmonary artery was augmented with an autologous pericardial patch. The patient was weaned from cardiopulmonary bypass uneventfully. Cardiopulmonary bypass and aortic cross clamp times were 60 and 43 min, respectively. Postoperative transesophageal echocardiography did not show any residual lesions, and the patient made an uneventful recovery.
Comment
The total absence of SVC is an extremely rare anomaly, often found with other congenital cardiac anomalies and/or conduction abnormalities. 2 Because it is usually asymptomatic, the incidence in the general population may be higher than detected. In the syndrome of bilateral absence of SVC, the left and right anterior cardinal systems involute, resulting in the persistent communication between the posterior cardinal vein and the supracardinal veins, thus forming a connection with the IVC via the azygos and hemiazygos venous system. 3 Symptoms in these patients are related to the associated cardiac or extracardiac anomalies. In the absence of other anomalies, most patients are asymptomatic or may uncommonly present with SVC syndrome. Very few cases of this anomaly have been reported, but those that have been published are largely from the adult age group. 4
Diagnosis of absent SVC should be made on transthoracic echocardiography, during segmental analysis of the cardiac structures. In the event of suspicion of absent SVC, either contrast-enhanced CT angiography or magnetic resonance imaging scan is imperative to delineate systemic venous drainage. Despite the benign nature of this anomaly, it has clinical implications in procedures such as cardiac catheterization, systemic venous cannulation for extracorporeal membrane oxygenation, transvenous pacemaker implantation and open-heart surgery. 5 Some palliative procedures for single ventricle physiology such as bidirectional Glenn or total cavopulmonary connection are difficult or even impossible to perform when there is absent bilateral SVC. 6
This anomaly in isolation does not warrant any intervention. In our case, the child was diagnosed with systemic venous anomaly on preoperative echocardiography. Computed tomography scan confirmed absent bilateral SVC, and cannulation strategy was planned accordingly. Cannulation strategies consist of venous cannulation of the brachiocephalic veins and IVC, 7 single IVC cannulation with large diameter cannula, or single right atrial cannulation with deep hypothermic circulatory arrest to carry out intracardiac repairs. Brachiocephalic venous cannulation for adequate drainage requires extrathoracic dissection with a risk of damage to adjoining neurovascular and lymphatic structures. Deep hypothermic circulatory arrest has systemic and neurological complications. We were able to achieve satisfactory venous drainage with single IVC cannula to conduct normothermic cardiopulmonary bypass and did not require any additional venous cannulation. In the postoperative period, the patient did not have any features of cerebral venous congestion. Long-term cardiac and abdominal ultrasound examination follow-up may be essential as these patients may be predisposed to portal hypertension due to higher pressure in the IVC due to increased blood volume. 8
Footnotes
Authors’ Statement
Informed consent was obtained from the patient's guardian to publish this case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.