
Abstract
Ganglioneuroma is a benign tumor requiring subtotal resection as a primary mode of treatment. There are several surgical approaches. A giant ganglioneuroma of the chest cavity may be approached via a clamshell thoracotomy. This manuscript presents a case of giant ganglioneuroma resected en bloc via clamshell thoracotomy in a seven-year-old child.
Introduction
Ganglioneuroma is a benign neuroblastic tumor arising from neuroectodermal cells originating from the neural crest. 1 Despite its benign nature, it can grow to a giant size. A subtotal resection of the tumor bulk is the standard of care for this tumor. 2 Clamshell thoracotomy has been described as a safe and efficient approach for the resection of giant intrathoracic tumors.3‐5 We present a case of en bloc resection of a giant thoracic ganglioneuroma via clamshell thoracotomy.
Clinical Summary
A seven-year-old female was evaluated after reports of weight loss. Heart sounds auscultated on right chest prompted a chest x-ray revealing a giant mass in the left hemithorax. A chest computerized tomography (CT) scan showed an 11.8 × 13.1 × 14.7 cm mass occupying the left pleural cavity and shifting the mediastinal structures rightward (Figure 1).
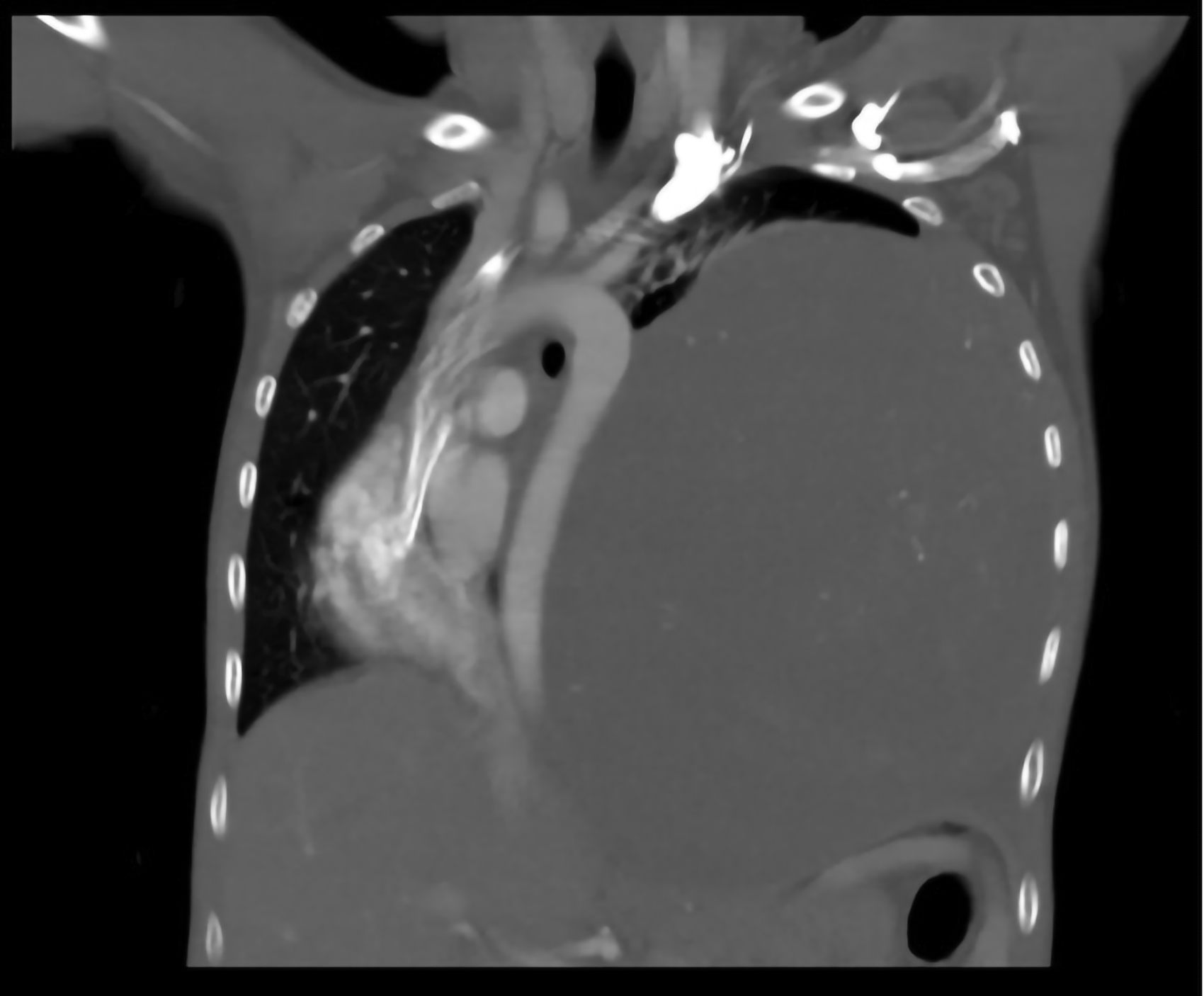
Computerized tomography scan of chest showing giant ganglioneuroma causing compression and deviation of mediastinal structures.
Chest/adrenal magnetic resonance imaging and a positron emission test-CT scan were performed. The mass did not have any neural involvement, local or distal spread. Interventional radiology–guided biopsy returned positive for ganglioneuroma. Urine metanephrines were negative.
Surgical Technique
A clamshell incision was made, and the chest was entered through the fourth intercostal space bilaterally. The internal thoracic arteries were ligated and divided. The sternum was transversely divided to connect the thoracotomies. The left lung was reflected medially. The tumor was not well encapsulated at the medial aspect and was adherent to mediastinal structures. Due to dense adhesions, the left vagus nerve was divided. Vascular control of nutrient arteries from posterior intercostal vessels was obtained. The tumor was dissected free of the esophagus, phrenic nerve, and hemiazygos vein. A small tear in the outer muscle layer of the esophagus was recognized, which was easily repaired. Some bleeding was encountered from the hemiazygos vein which was rapidly controlled. Approximately 99% of the tumor was removed en-bloc and was sent to pathology. The tumor close to the neural foramina was left in situ to prevent injury to the nerve roots exiting the spinal column (Figure 2). Station 5 and 6 lymph nodes were sent to pathology as they appeared abnormal. After a Valsalva maneuver, the left lung inflated and filled the majority of the left pleural space. Two chest drains were placed. The sternum was closed with stainless-steel wires, and the thoracotomy was closed in layers in the standard fashion.
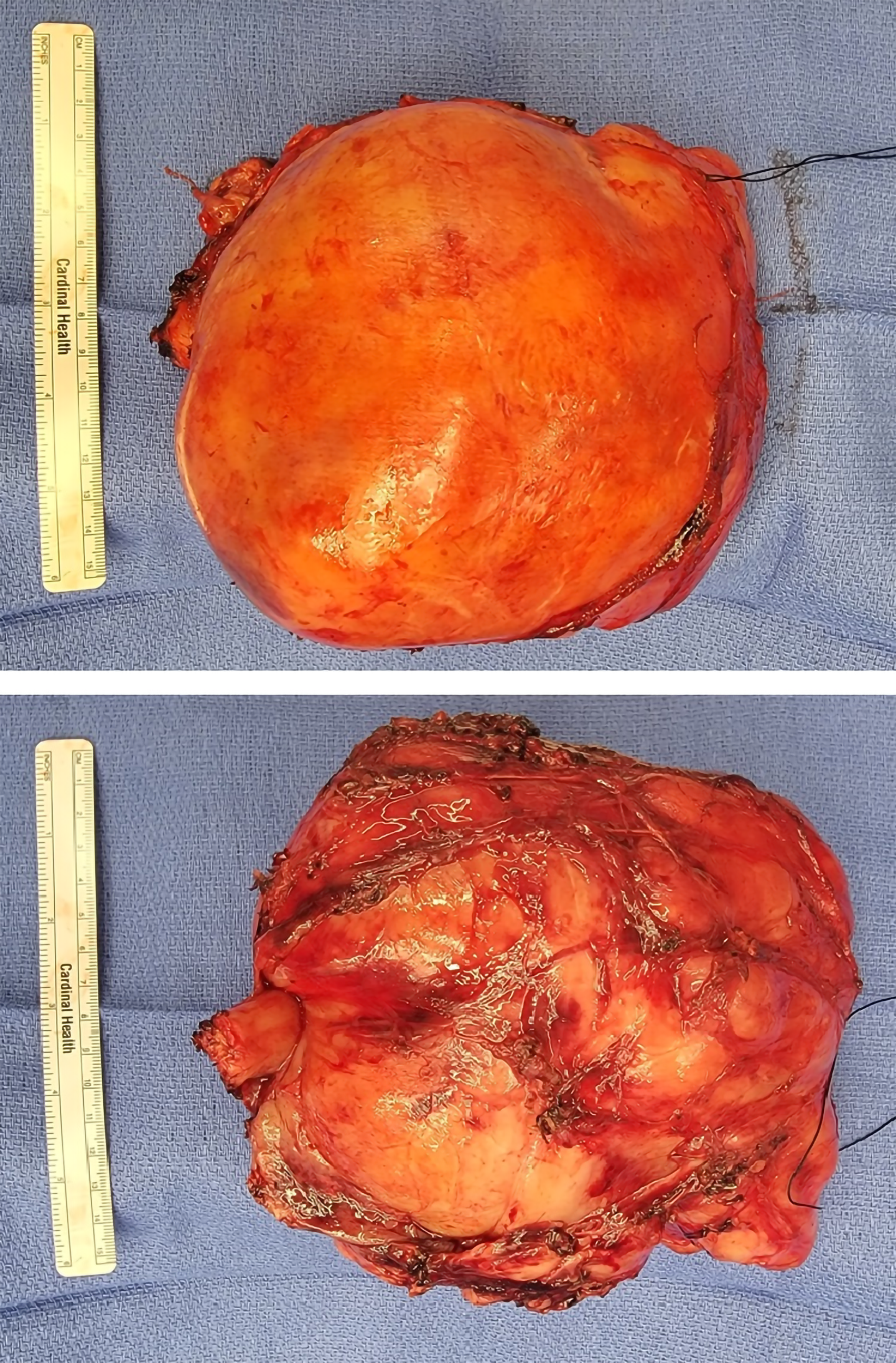
Gross specimen of giant ganglioneuroma resected en-bloc (top: anterolateral aspect, bottom: posteromedial aspect).
The patient was extubated in the intensive care unit on postoperative day 1. Except for a post-chest tube pull pneumothorax requiring percutaneous chest tube placement, her course was uneventful. No blood transfusion was required intraoperatively or postoperatively. The patient was discharged on postoperative day 11. The pathology showed ganglioneuroblastoma, intermixed subtype, with periaortic lymph node involvement.
Comment
Resection of a giant ganglioneuroma of the chest can be a challenge. Different approaches can be used depending on the location and the size of the tumor.6‐8 Typically, these tumors have a capsule and can be easily removed. However, larger ganglioneuromas can compress the mediastinal structures and chronic inflammation may cause adhesions.
We selected a clamshell thoracotomy approach because we anticipated most of the critical dissection to be in the mediastinum. If needed, we had immediate access to the heart and great vessels to put the patient on cardiopulmonary bypass.
In this case, due to the adhesions between the tumor and the vital structures in the mediastinum, had a left thoracotomy been performed, the tumor would have been debulked in piecemeal fashion and it would have been difficult to control bleeding or identify esophageal injury. A sternotomy may have provided us with adequate exposure to the medial aspect of the tumor; however, the approach would have limited the visualization for the rest of the dissection. Postoperative chest X-ray showed mild elevation of left hemidiaphragm. The patient did not have any respiratory distress and, therefore, diaphragmatic evaluation was not performed. We hypothesize that the elevation is due to the hypoplastic left lung falling back into the pleural space after the tumor was removed. Since the natural history suggests that the residual tumor does not grow, no further treatment was necessary. 2 The patient will be monitored with serial CT scans and urine vanillylmandelic acid and homovanillic acid levels.
A clamshell thoracotomy has some potential disadvantages: large incision, postoperative pain, inability to utilize internal thoracic artery for future coronary revascularization, and challenges in pulmonary toilet. Our patient's pain was controlled, and she was discharged on oral analgesics. There was no need for prolonged pulmonary toilet. We recommend considering clamshell thoracotomy as a surgical approach for benign and malignant giant tumors of the thoracic cavity.
Supplemental Material
sj-docx-1-pch-10.1177_21501351231183967 - Supplemental material for En Bloc Resection of a Giant Ganglioneuroma of the Chest Through Clamshell Thoracotomy
Supplemental material, sj-docx-1-pch-10.1177_21501351231183967 for En Bloc Resection of a Giant Ganglioneuroma of the Chest Through Clamshell Thoracotomy by Dhaval Chauhan, Patrick Bonasso and Jai P Udassi, Christopher E Mascio in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Authors' Statement
The Institutional Review Board (IRB) or equivalent ethics committee of West Virginia University approved the study protocol and publication of data. Permission was granted by the patient's parent to publish the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.