
Abstract
Cardiac tumors are very rare in children, and echocardiography is very important in their detection. The clinical presentation can vary greatly depending on arrhythmia or obstruction. One of the most important factors determining the surgical approach is the clinical process. In this case report, we report the surgical treatment of a rhabdomyoma that caused refractory ventricular tachycardia.
Introduction
Cardiac rhabdomyoma is one of the most common cardiac tumors. Some rhabdomyomas can be fatal by causing arrhythmias, issues with ventricular filling, or outflow tract obstructions.1,2 Rhabdomyomas may present clinically with different symptoms, depending on the location and size. In some cases, medical treatment may be inadequate to overcome arrhythmias caused by this disease. In these cases, surgical removal of the tumor may be indicated. In this case report, we present the successful surgical treatment of refractory ventricular tachycardia that was not controlled by medical therapy.
Case Report
A six-year-old child was referred to our hospital because of refractory ventricular tachycardia originating from a cardiac mass in the left ventricle. Rhythm restoration could not be achieved despite propranolol and flecainide medical treatment. The patient presented with a systolic murmur (graded 2/6), no cyanosis, and no edema. The transthoracic echocardiography confirmed there was a large mobile 27 × 20 mm2 mass attached to the left ventricle apex (Figure 1). The exact localization of the mass was determined by magnetic resonance imaging (MRI), and it was isointense to the muscle on T1-weighted images (Figure 2). Surgical resection of the tumor was planned. A median sternotomy was performed, and cardiopulmonary bypass (CPB) was established through the ascending aorta and right atrium. Cardiac arrest was achieved by placing an X-clamp and giving cardioplegia. Ventriculotomy was performed at the apex of the left ventricle, and the mass with apicoseptal adhesions was resected from the septum (Figure 3). The ventriculotomy was closed primarily with PTFE felt pledgets. The CPB time was 21 min. Analysis of the intraoperative transesophageal echocardiogram image showed the mass was completely removed, and the septum was intact. There were no complications following the operation. Histopathological examination showed the mass was a rhabdomyoma. The patient did not have any rhythm problems in the postoperative period and was discharged on the seventh postoperative day.
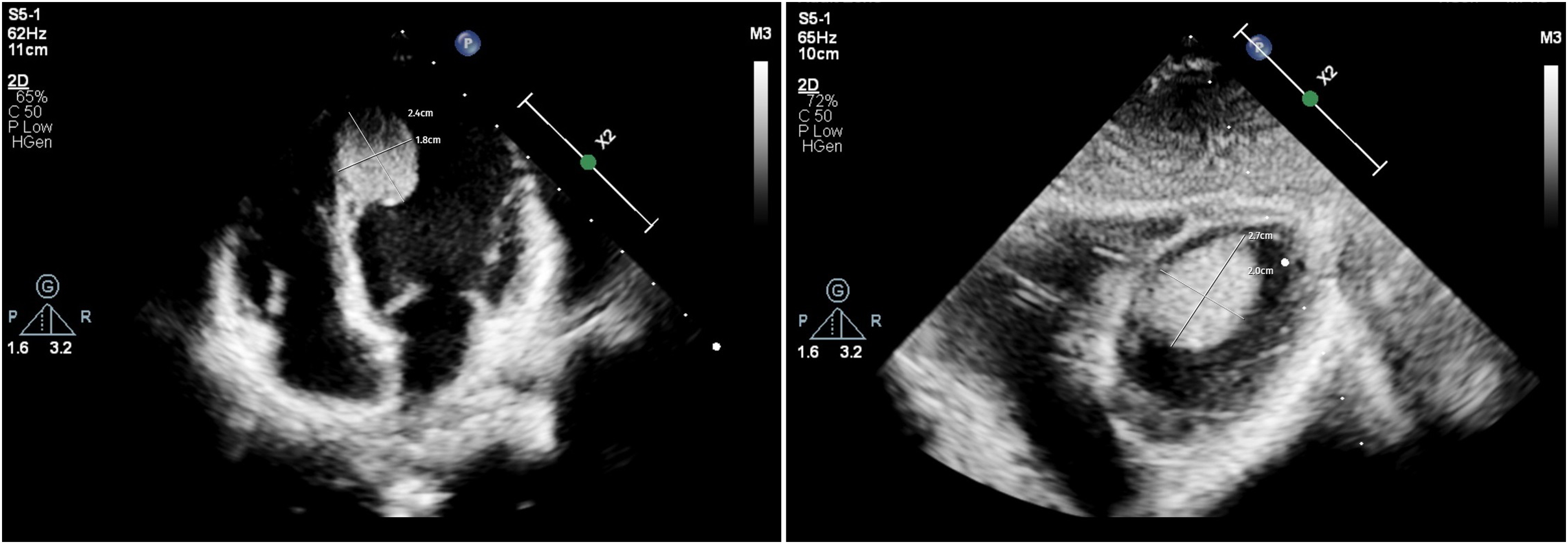
A large mobile mass attached to the left ventricular apicoseptal segment on transthoracic echocardiography.
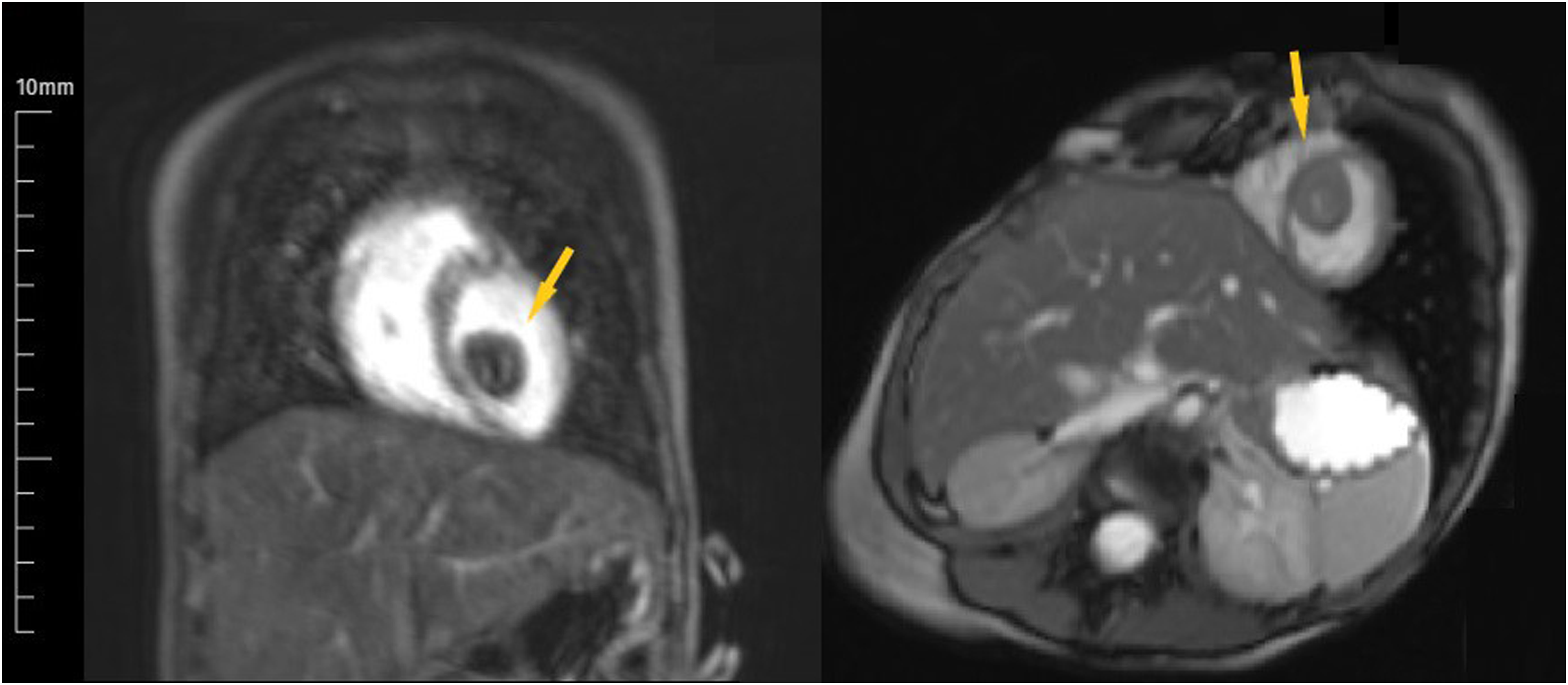
Coronal and axial cardiac MR sections demonstrate isointense mass (arrows) on T1-weighted imaging. MRI, magnetic resonance imaging.
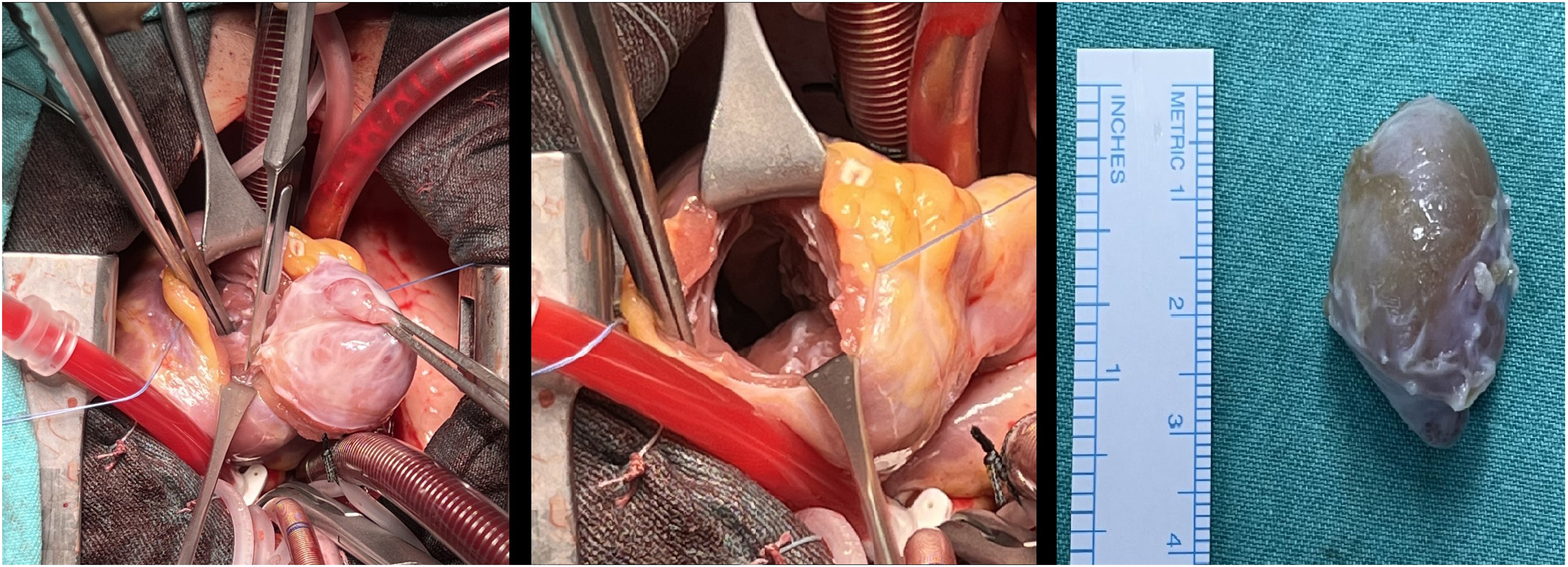
Intraoperative resection of the mass via ventriculotomy.
Comment
Rhabdomyoma is one of the most common childhood cardiac tumors. Rhabdomyomas are often located in the left ventricle and may cause sudden death in childhood. 3 Although spontaneous regression can sometimes be observed, some patients require surgical intervention. In clinical evaluation, whether the patient is symptomatic or not is very important for decision-making. Patients with cardiac rhabdomyoma require surgery primarily for hemodynamic reasons affecting blood flow or for the management of arrhythmias. 4 Proximity to or contact of the tumor with the nervous system may cause arrhythmias, and resistant arrhythmias that cannot be controlled with medical treatment may require surgical resection. 5
Echocardiography has significant diagnostic value for diagnosing tumors and is the primary imaging modality in children because it can accurately show the location and size of tumors. In addition, computed tomography and MRI are of crucial importance in helping to confirm the diagnosis and gain more insight into the surgical strategy.
Delmo et al reported that urgent surgical intervention may be required in cases of hemodynamic impairment. 6 Wang et al emphasized that surgery should be performed as soon as possible after the detection of a symptomatic intraventricular mass. 7 In the case we presented, there was refractory ventricular tachycardia that did not improve despite all medical treatments. Therefore, we planned an operation as early as possible in order to prevent the increased risk of mortality and morbidity. Removal of the tumor with its capsule was performed without the need for any ventricular resection. No invasive or noninvasive arrhythmia treatment was required for our patient, who did not have any arrhythmia after the operation. We have demonstrated that a good outcome for arrhythmia caused by rhabdomyoma can be achieved with an effective surgical resection.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.