
Abstract
Hydatid cyst is a human parasitic disease caused by echinococcus granulosus that affects mainly the liver or the lungs but may be found in any organ, including the heart in up to 2% of the cases. Humans are infected as accidental hosts by contaminated vegetables or water and by contact with saliva from infected animals. Although cardiac echinococcosis can be fatal, it is rare and often asymptomatic in the early stage. We present the case of a young boy living on a farm who suffered from mild exertional dyspnea. He suffered from pulmonary and cardiac echinococcosis and was treated surgically through median sternotomy to prevent potential cystic rupture.
Clinical Presentation
A 12-year-old boy suffered from mild exertional dyspnea and presented with a remarkable thorax deformity. On clinical examination, there were no inspiration-related excursions on the right side and no auscultation murmur.
Computed tomography (CT)-scan (Figure 1) and echocardiography (Figure 2) led to a strong suspicion of pulmonary and cardiac echinococcosis. Because of the risk of cyst leakage or rupture with consecutive allergic reaction with significant morbidity and mortality, surgical resection was considered.
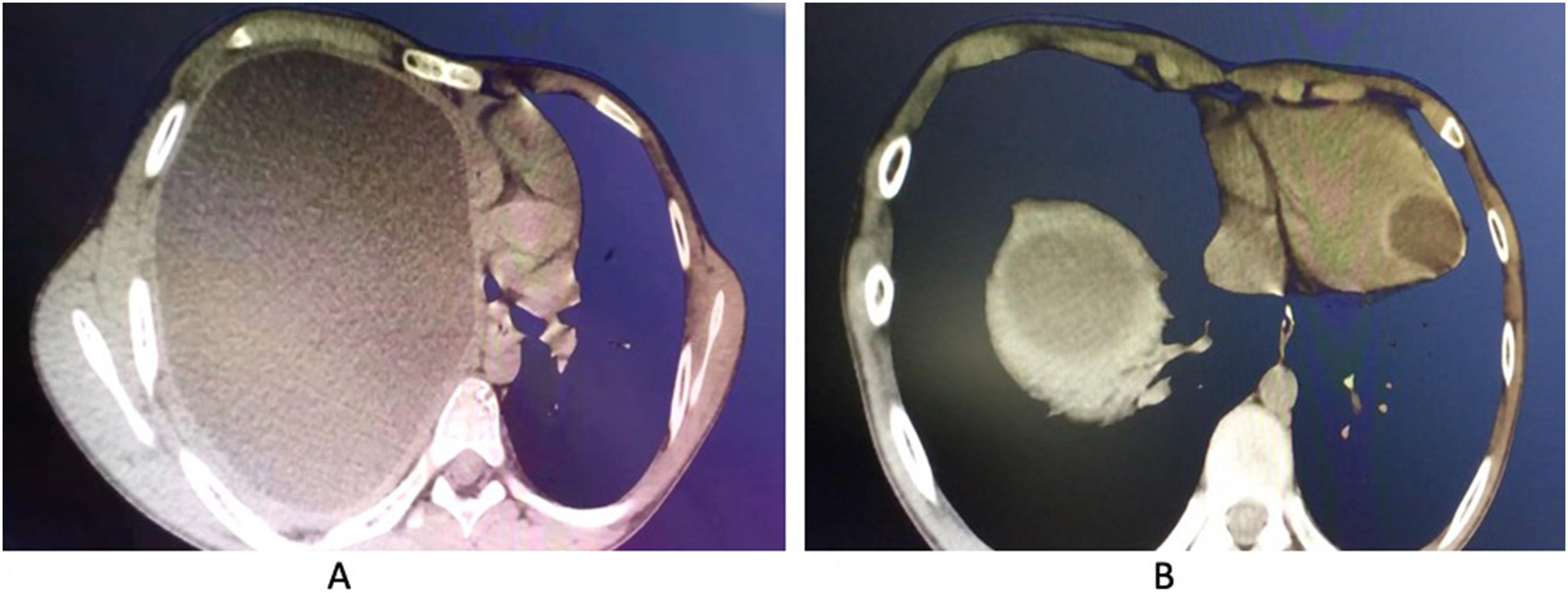
Chest CT-scan demonstrating a huge hydatid cyst leading to a major thorax deformity with almost complete lung collapse on the right side (A) and an additional intraventricular cyst close to the left ventricular apex (B).
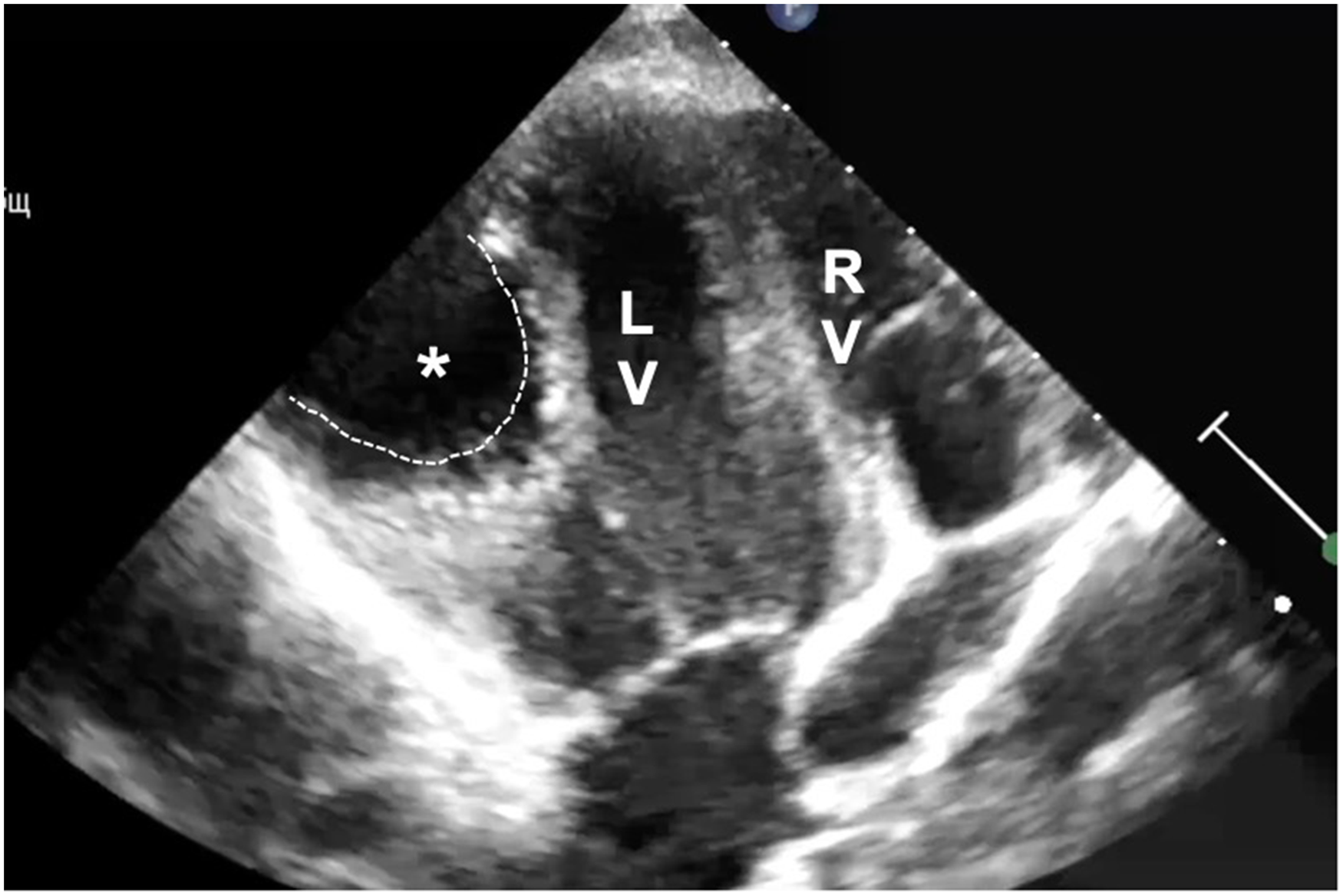
Transthoracic echocardiography shows intraventricular hydatid cyst (dotted line). Surprisingly, there was no significant cardiac valve dysfunction observed. LV, left ventricle; RV, right ventricle.
Perioperative antibiotic prophylaxis was done with a second generation cephalosporins. Surgical approach was performed through median sternotomy to allow access to both the right lung and the left ventricle. Following the opening of the right pleural cavity, the cyst could be resected in toto. However, communication with the bronchial system was observed. Direct closure was not feasible because of the size of the leak that was finally closed using the narrow tissue that was left in situ after the excision of the cyst itself together with its membrane. No residual leak was observed thereafter. Next, cardiopulmonary bypass was instituted in normothermia following heparinization, and excision of the left ventricular cyst was performed on the beating heart through an incision at the level of the apex (Figure 3). This incision was closed using direct running polypropylene suture.

Left: View on the left ventricular apex with the cyst (dotted line) almost perforating the myocardial wall. Middle: after punction of the cyst, complete excision was performed. Right: The left ventricular cavity was also rinsed with hyperosmotic solution and then closed with a continuous monofilament suture.
The cavities were rinsed with hyperosmotic glucose solution for 20 minutes. The postoperative recovery was completely uneventful, and the boy was discharged at postoperative day 5. He was put on albendazole for three months.
Comment
Echinococcosis is a worldwide health problem causing considerable pediatric morbidity and mortality in endemic areas.1‐3 The presentation varies by age and pulmonary cystic echinococcosis is the dominant localization in the pediatric population. 3 Although small pulmonary cysts most often do not cause any symptoms, large cysts may cause chest pain, dyspnea, and hemoptysis.4‐6 Treatment includes enucleation of the cyst, closing of bronchial air leaks in the pericystic cavity which is optionally closed or marsupialized, preserving as much lung tissue as possible.
Cardiac echinococcosis can also be fatal but is rare and often asymptomatic in the early stages. Therefore, clinical suspicion is important for a correct diagnosis. Echocardiography, CT, and magnetic resonance imaging are useful in the diagnosis and location of cardiac echinococcosis. Intracardiac rupture of a cyst can cause germinative membrane or secondary cysts embolization to the lungs or to organs supplied by the systemic circulation. Intrapericardial rupture of a cardiac hydatid cyst can lead to acute pericarditis, cardiac tamponade or eventual constrictive pericarditis. Cysts may also cause valvular dysfunction and/or arrhythmias.
Surgery was performed in Uzbekistan and this explains a few particularities: no conventional chest x-ray was performed because of costs since it was clear that a CT scan would be necessary. Surgery was performed on the beating heart to avoid potential negative effects of myocardial ischemia and facilitate postoperative treatment. This was probably the most critical point of the cardiac approach but due to a large experience with beating hearts (eg, left ventricular assist device implantation, repair of ventricular septal defects, and mitral valve procedures), we found it an attractive technique. Of course, major attention has to be paid to the fact that no air escapes into the ascending aorta, even though an aortic root cannula is used for aortic venting. 7 The technique does not necessarily require a vent through the right upper pulmonary vein but we also paid attention to the fact that the aortic valve does not open and during rinsing, the left ventricle was almost always kept full. Transesophageal echocardiography was used during the operation and the anesthesiologist was continuously checking for any air in the left ventricle and/or in the aorta. In fact, excision of the intracardiac cyst was easily performed because it was located at the left ventricular apex. Closure of the bronchial leak was performed using the thick scar tissue found around the cyst membrane. This was considered a good alternative to a muscle or an omentum flap that would have required more extensive surgery (eg, lateral thoracotomy or opening of the abdominal cavity).
Combined surgical resection, washout of the remaining cavity with hypertonic saline solution, and concurrent albendazole therapy typically yield excellent results. Albendazole alone has also been reported to be successful in treating cardiac echinococcosis. 8
This case report with the impressive imaging and intraoperative pictures demonstrates that combined pulmonary and cardiac resection of hydatid cysts can be performed safely. Washout of the remaining cavity with a hypertonic solution and adjuvant albendazole therapy (2 × 400 mg) led to a good outcome in this young patient who is still doing well more than three years after surgery.
Footnotes
Authors’ Statement
The young patient was informed and the parents gave written consent for publication if this report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.