
Abstract
Severe left outflow tract obstruction (LVOTO) is not always associated with hypoplastic left heart syndrome (HLHS). Aortic valvar atresia or complex LVOTO in the presence of a large ventricular septal defect (VSD) are a rare group of lesions that offer the possibility of biventricular repair. The Yasui procedure is the commonest surgical approach which can be performed as a primary neonatal correction or as a staged procedure with a Norwood followed by a subsequent Rastelli. This article reviews the surgical outcomes and decision-making process. Both strategies are reasonable with the trend toward staged procedure in the setting of the additional interrupted arch, with neonatal survival of > 90% in the modern era and excellent long-term survival. Re-intervention is mostly related to conduit revision and the need for re-operation for LVOTO is rare. Deciding between conventional repair and the Yasui in cases of LVOTO/VSD can be difficult and there are no uniform accepted criteria. In a typical neonate, an aortic annulus < 4.5 mm is generally the limit of acceptability for a conventional repair. In selected cases of LVOTO/VSD, an alternative to the Yasui is the Ross-Konno. Retrospective comparisons between the 2 techniques are difficult due to differing patient characteristics (especially associated with mitral valve disease) but the neonatal Ross has been associated with higher early mortality.
Keywords
Introduction
Not all aortic atresia is associated with hypoplastic left heart syndrome (HLHS). Within the whole spectrum of left heart obstructive lesions, there are rare variants that combine a large ventricular septal defect (VSD) with either aortic valvar atresia or severe outflow tract obstruction. The large VSD allows for an unobstructed pathway to the systemic circulation by way of the pulmonary artery and ductus arteriosus. 1 Consequently, it allows for normal or near normal development of the left ventricle (LV) in both size and function and therefore has the potential to support a biventricular circulation. Aortic atresia and ventricular septal defect (AA/VSD) is a very rare congenital defect, accounting for 4% to 7% of all patients with aortic atresia,2–4 occurring in 2 per 100 000 live births. It was Maurice Lev in 1966 who noted that the presence of the VSD created a different clinical entity to that of aortic atresia associated with HLHS, 5 typically with an apex forming left ventricle, normal mitral valve with no sign of endocardial fibroelastosis.
In AA/VSD, the morphological origin of aortic atresia is created by extreme malalignment of the conal (outlet) septum. This leftwards and posterior deviation is the feature which also produces the large outlet VSD 3 which is typically a muscular outlet but can have a perimembranous extension. The lack of antegrade flow through the ascending aorta during fetal life then produces a characteristically diminutive vessel postnatally at < 2 mm (see Figure 1A). This hypoplasia of the ascending aorta is the same morphological association as seen in the large studies of HLHS when comparing aortic atresia phenotypes to those with aortic stenosis.
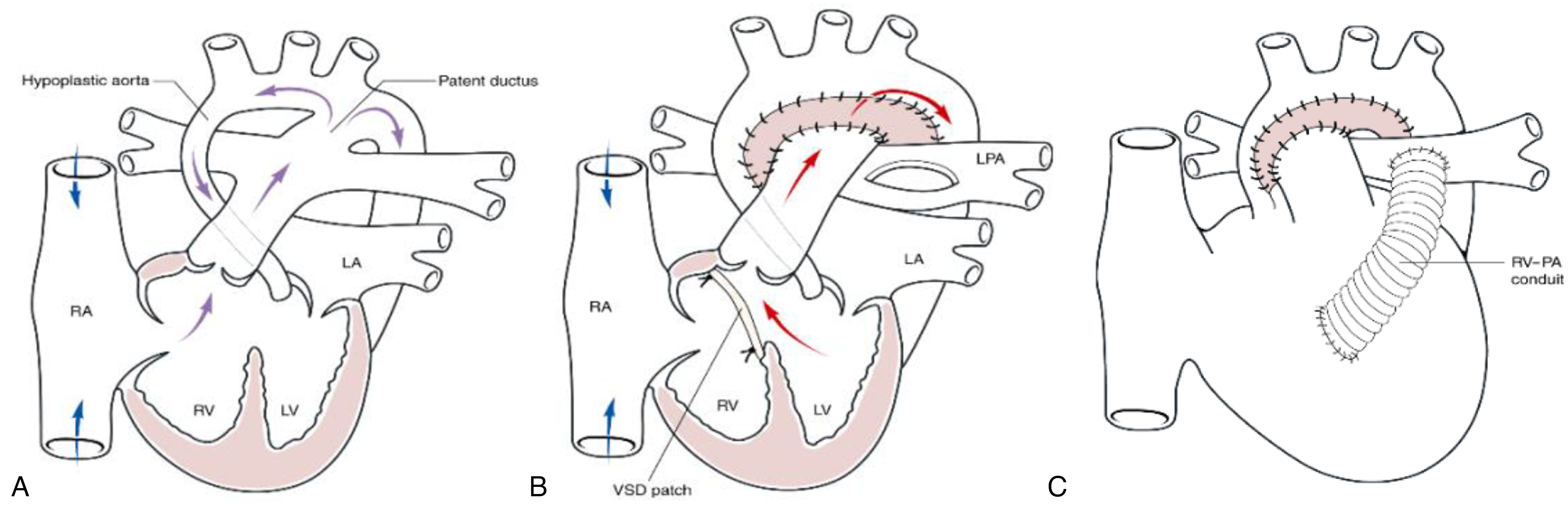
Diagram showing the key anatomical findings in aortic atresia with ventricular septal defect and the principles of the Yasui procedure: (A) Pre-operative anatomy showing the large VSD and diminutive ascending aorta with duct-dependent circulation; (B) Yasui procedure in which the aortic arch is reconstructed with the creation of a Damus-Kaye-Stansel procedure and the arch augmented with a patch. The VSD is closed with a patch that commits both the aortic and pulmonary roots to the left ventricle; (C) Yasui Procedure completed with the placement of an RV-PA conduit (RA—right atrium; LA—left atrium; RV—right ventricle; LV—left ventricle; LPA—left pulmonary artery) [printed with permission from Krishna Moorthy PS, McGuirk SP, Jones TJ, Brawn WJ, Barron DJ, Damus-Rastelli Procedure for Biventricular Repair of Aortic Atresia and Hypoplasia, Ann Thoracic Surg. (2007); 84:142-146.].
Closely related to AA/VSD is the cono-ventricular malalignment seen in the interrupted aortic arch (IAA) and VSD, where the aortic root and subaortic area can be prohibitive to supporting the systemic circulation. In 1987, it was 2 cases such as this in which Hasato Yasui first devised the procedure which carries his name: the concept was to amalgamate the aortic and pulmonary roots to create a single outlet and then close the VSD in such a way as to commit the LV to this common outlet (in morphological terms, creating a double outlet LV). 6 An RV-PA conduit was then used to construct the right outflow tract (Figure 1B). The Yasui procedure has since been applied to all variants of extreme left ventricular outflow tract obstruction (LVOTO) and is the definitive biventricular repair for AA/VSD. Since the arch reconstruction shares the same features as the Norwood procedure, this has also been referred to as the “Norwood-Rastelli,” the “Damus-Rastelli” or even the “Norelli” operation.
This article will focus on the 3 areas where management is still not clear:
Whether to complete the Yasui as a single-stage procedure in the neonate or whether to use a staged approach with a Norwood procedure as a neonate and then completing the Rastelli component as a second stage in the older infant. Decision making in the small outflow tract—conventional repair versus Yasui. Comparison of the Ross-Konno as an alternative to Yasui in selected cases.
Patients and Methods
The rarity of AA/VSD and the fact that Yasui is equally applicable to severe LVOTO/VSD has meant that most published experiences with this technique combines both morphological subtypes, and include patients with varying degrees of aortic arch hypoplasia and aortic interruption (Table 1). It has also been used as an LVOT bypass technique to rescue those patients with recurrent LVOT obstruction following initial conventional repair. 19 Conventional repair of LVOTO/VSD with a deviation of the outflow septum is characterized by a high incidence of recurrent left outflow obstruction of 20% to 50% at 5 years16,20 and the need to resect the conal septum at the time of surgery is a marker for those likely to develop this subsequent obstruction. 16
Summary of Published Retrospective Observational Studies of the Yasui Operation.
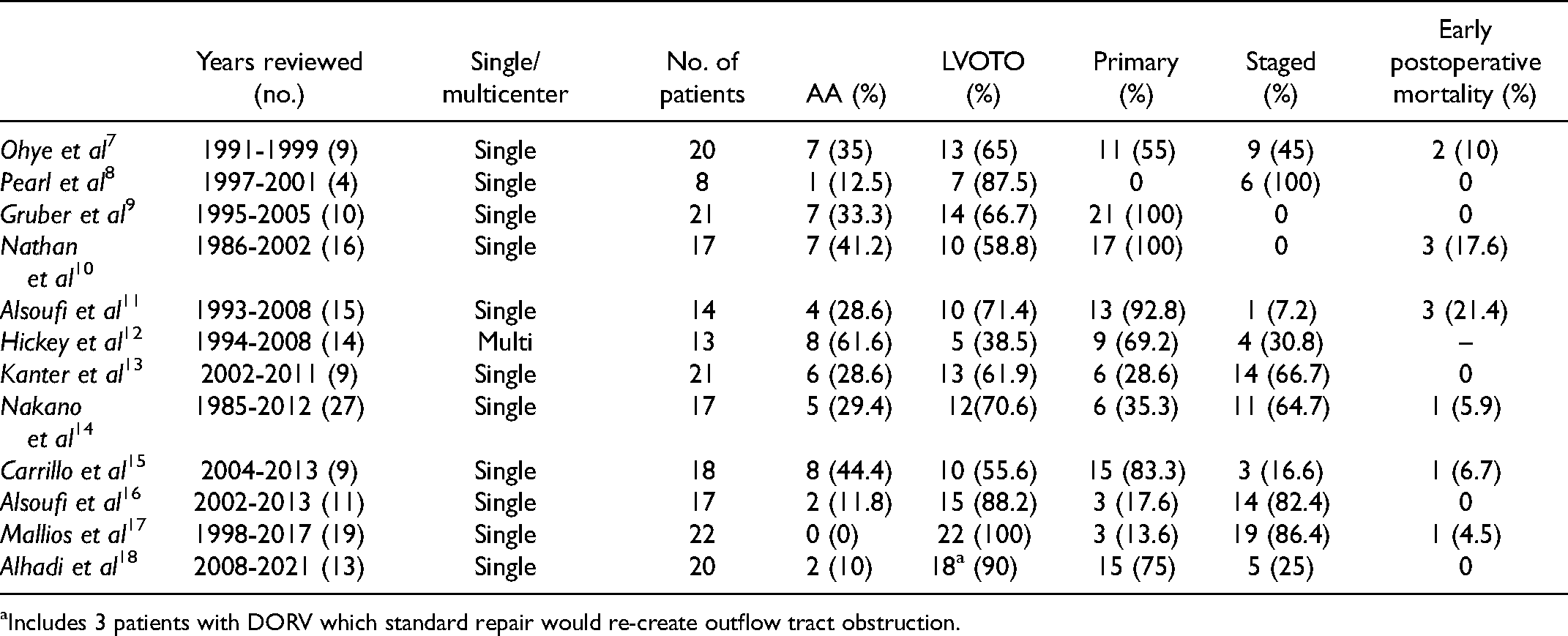
Includes 3 patients with DORV which standard repair would re-create outflow tract obstruction.
In AA/VSD, the surgical decision is straightforward, as usually the LV size and mitral valve are normal and Yasui is the procedure of choice. However, in patients with LVOTO/VSD, the decision to choose conventional repair versus Yasui can be difficult as there are no uniformly accepted criteria. There is no consistent discriminant anatomical value and institutional preference clearly plays a part in decision making. Detailed preoperative measurements of valvar and subvalvar dimensions are most valuable (Figure 2), but although annular and root dimensions are relatively fixed, there can be some dynamic components to subaortic measurements, making these less consistent. In a review of 36 infants following IAA/VSD repair, Hirata et al 21 determined a minimum diameter of the aortic annulus to be the baby's weight (kg) + 1.5 mm for a conventional repair. Seven out of 8 infants with an aortic annulus’ between body weight (kg) + 1 mm to + 1.5 mm required re-operation in contrast with 1/26 of patients with an annulus greater than body weight (kg) + 1.5 mm. 21 Other smaller studies have suggested that body weight + 1 mm may be acceptable.14,21 In a typical neonate, this suggests that an aortic annulus smaller than 4.5 mm is the limit of acceptability for a conventional repair. When examining aortic z-scores, a value of z < −2.5 has been shown to be a risk for postoperative LVOTO in standard repair, below which the rate of re-operation almost doubled when compared to those undergoing a Yasui procedure (64.3% vs 37.5%, respectively) and for the need for LVOT intervention increased by 2.7-fold. 22
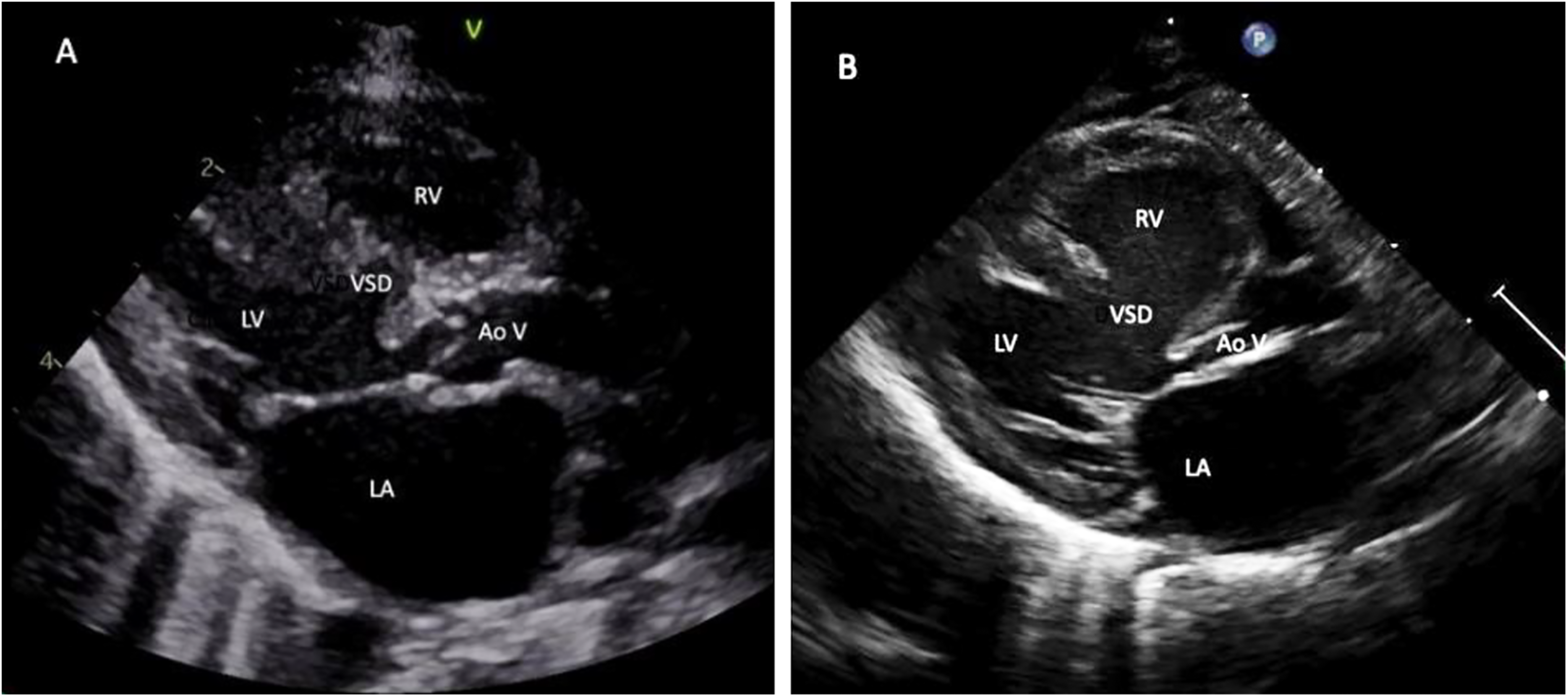
Echocardiogram: parasternal long-axis view demonstrating left ventricular outflow tract obstruction (LVOTO) suitable for the Yasui operation (A) multi-level LVOTO due to mal-aligned VSD and moderately hypoplastic aortic valve. (B) LVOTO tunnel due to the posterior deviation of outlet septum with the severely hypoplastic aortic valve. LA—left atrium; LV—left ventricle; VSD—ventricular septal defect; RV—right ventricle; AoV—aortic valve.
The surgical technique is to set up as for a Norwood procedure, with arterial perfusion via cannulation of the ductus or through a graft on the innominate artery. Two arterial cannulae are used in the setting of IAA. Bicaval cannulation is preferable to facilitate the intracardiac component of the surgery. The VSD is accessed through the right ventriculotomy. The VSD is usually large and does not require enlargement; however, if this is required then it can be safely enlarged to its rightward and superior margin, well away from the conduction tissue. Most VSDs (70-80%) are muscular outlets and are remote from the bundle. Working through the ventriculotomy, the VSD is closed by bringing the patch anterior to the pulmonary valve, even up to the upper margin of the ventriculotomy if needed. 23 Given the outlet position and size of the VSD, this creates a wide pathway through to the neo-aortic valve (Figure 3).
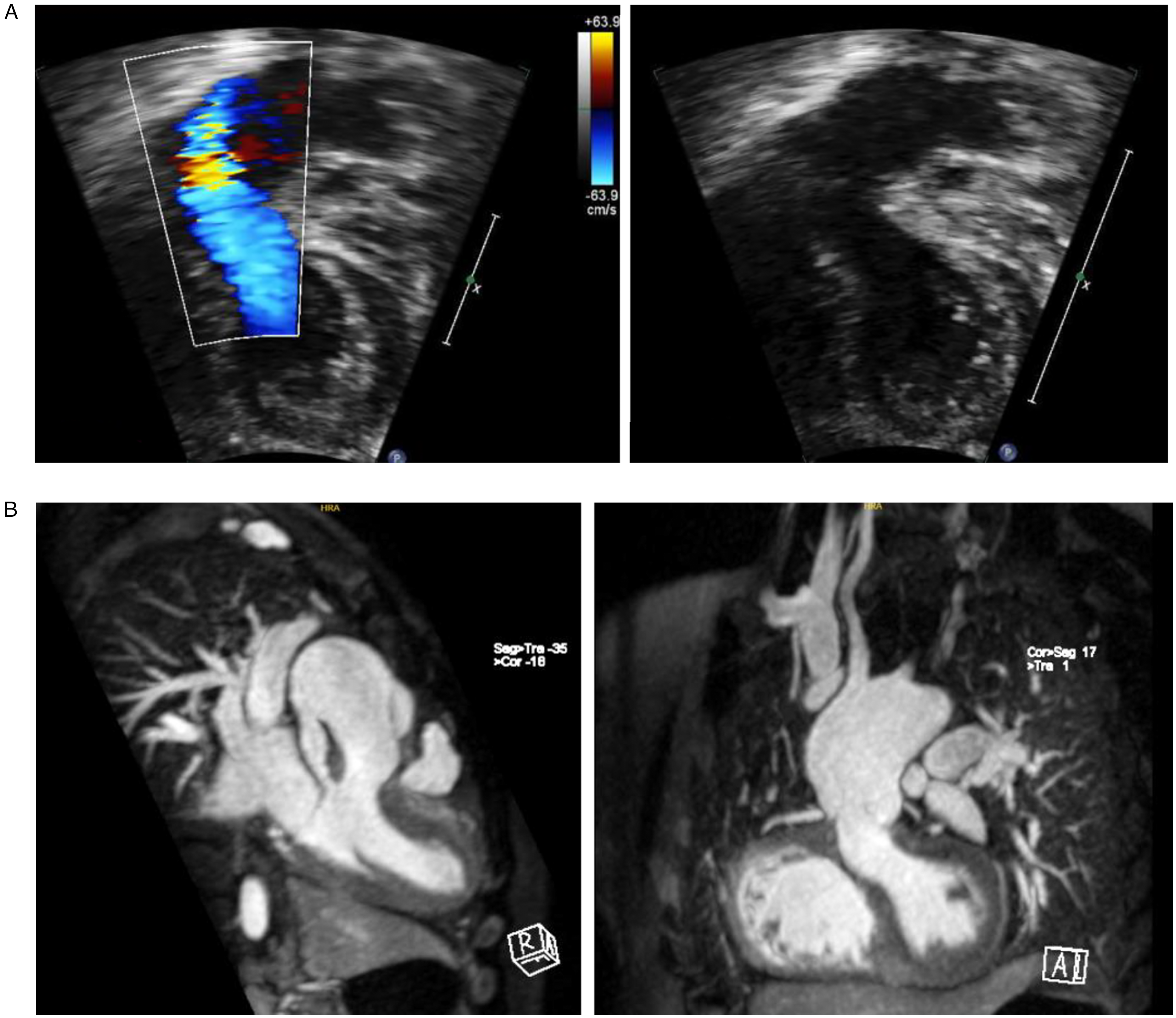
Postoperative imaging demonstrating the intracardiac baffle post-Yasui: (A) Trans-oesophageal echocardiogram showing the left ventricle (LV) and outflow baffled through the VSD to the neo-aortic valve (Neo AoV). (B) MRI images of unobstructed left ventricle outflow baffled to the neo-aortic valve (Neo AoV). The DKS can be seen and is unobstructed.
The arch is reconstructed in the same manner as for a Norwood procedure, usually with a patch of pulmonary homograft or glutaraldehyde-preserved autologous pericardium. The repair is completed with the placement of an RV-PA conduit from the previously created ventriculotomy and is usually routed to the left side of the DKS. It can also be routed to the right side. The most commonly used conduits have been pulmonary homografts and bovine jugular vein conduits (Contegra®).
Some authors have suggested avoidance of a conduit by performing a Lecompte maneuver and attaching the pulmonary artery confluence to the upper margin of the ventriculotomy and then roofing with a simple patch, similar to the REV procedure.7,23,24 However, this does lead to pulmonary regurgitation (ie, regurgitation from the PAs into the RV) which has precipitated high re-intervention in some reports. 25
Results
The majority of outcome data come from a series of single-center experiences, typically of 20 to 25 cases (Table 1). Approximately 70% of the Yasui operations are for LVOTO/VSD and 30% for AA/VSD. The operative mortality is typically 10% to 15%, although there are several smaller series with zero early mortality. Carrillo et al 15 retrospectively compared primary Yasui against a contemporary group of HLHS patients undergoing Norwood and showed significantly lower operative mortality for Yasui (6.7% vs 16%), reflecting the advantages of biventricular physiology despite similar surgical procedures. Heart block is an important risk having been recorded in up to 5% to 10% of cases.9,15,18 Postoperative outcomes are largely influenced by noncardiac comorbidities, especially in the IAA group where the incidence of genetic abnormalities, predominately 22q11, is as high as 60%.9,16,20
Freedom from reoperation on the LVOT is very good in most series (80-90% at 10 years)10,13,14,16,17 and the need to enlarge the VSD at the time of surgery has been shown to be a risk factor for subsequent LVOTO, implying that those patients with a smaller VSD are those at the greatest risk. Some authors have suggested that routine VSD enlargement will reduce the risk of subsequent LVOTO but most studies have not felt that routine enlargement is necessary. 11 The rate of VSD enlargement with Yasui is generally low at 0% to 20% in most series7–10,13,15,17 but this is very variable and much of this is based on subjective surgical assessment at the time of surgery—guidance being that if the septal defect is smaller than the pulmonary valve, then preference is to enlarge it.
Late survival is extremely good with very little attrition beyond the immediate postoperative period. Five-year survival is between 75% and 100%7,11,13–16,18 and 10-year survival is between 69% and 88%12,14,16 (Figure 4). Re-interventions are summarized in Table 2, the commonest being replacement of the RV-PA conduit. Conduit replacements are likely to be inevitable as the child grows and constitute the majority of interventions during this later period, with an expected conduit survival of 70% at 5 years. The timing of subsequent RV-PA conduit exchange is quite variable, ranging typically from 1 to 9 years.
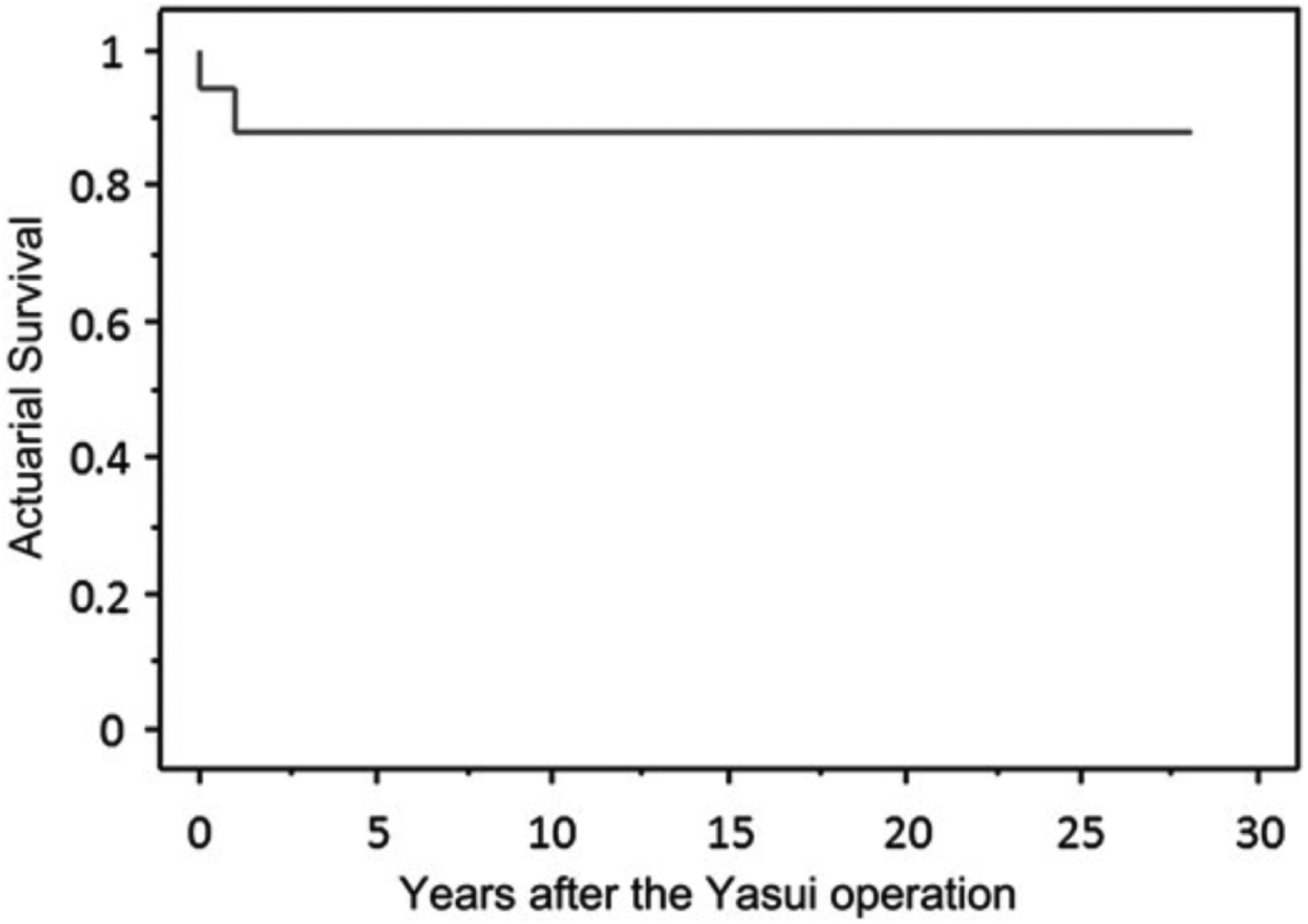
Actuarial survival following Yasui procedure including the original patient from Fukuoka Hospital. There were a total of 17 patients treated over 27 years with a 10-year survival of 89% [printed with permission from Nakano T, Kado H, Tatewaki H, Hinokiyama K, Machida D, Ebuoka N, Yasui H. The Yasui operation for patients with adequate-sized ventricles and ventricular septal defect associated with obstructions of the aortic arch and left ventricular outflow tract. Eur J Cardiothorac surg. (2014): e166-72.].
Need for Re-operation Following the Yasui Operation, in Particular Need for Conduit Replacement and Left Ventricular Outflow Tract Surgery.
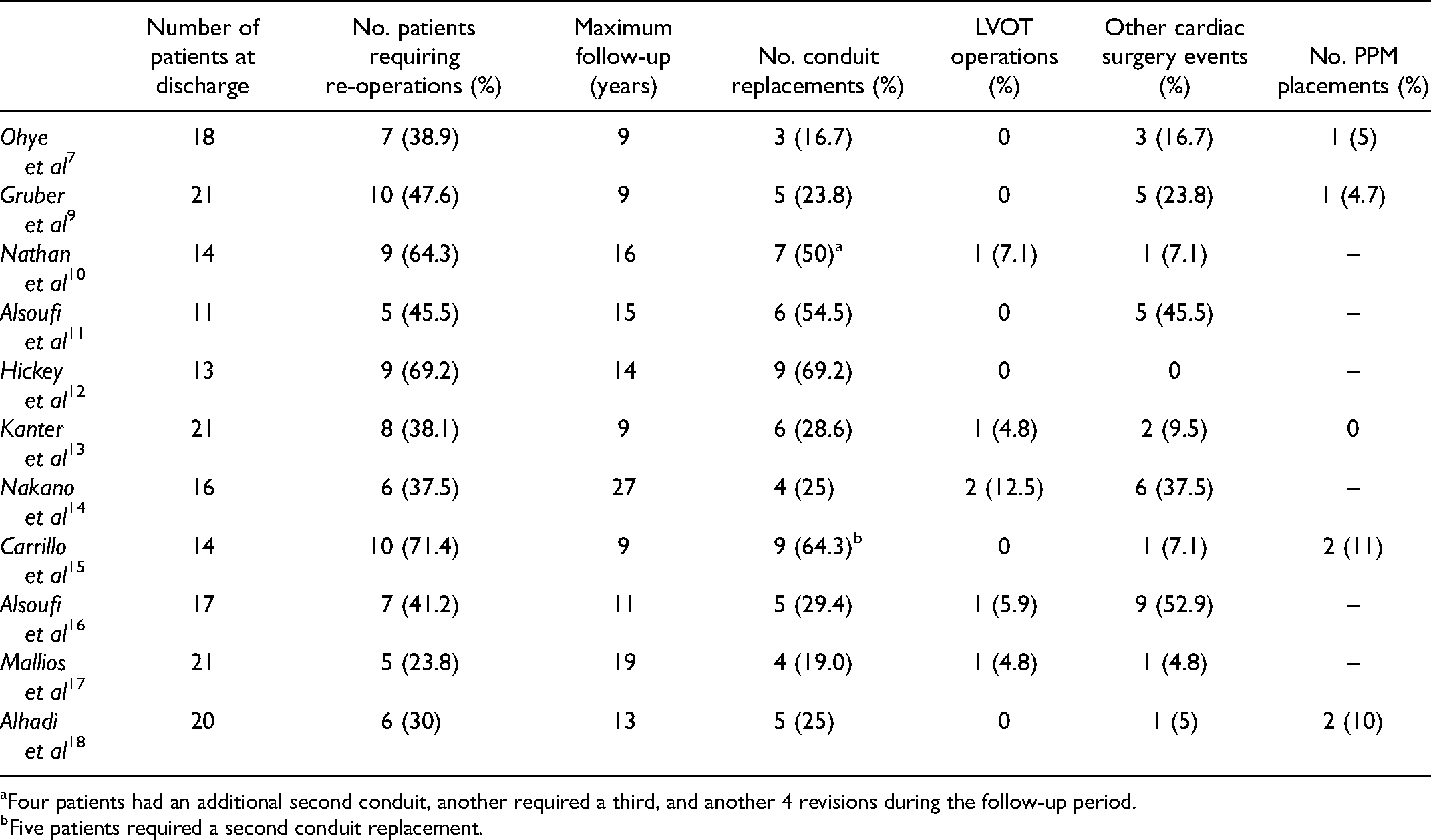
Four patients had an additional second conduit, another required a third, and another 4 revisions during the follow-up period.
Five patients required a second conduit replacement.
Primary Versus Staged Approach
Both primary (single stage) repair and staged (Norwood with subsequent Rastelli) repair have been widely practiced—with both strategies being used to varying extents in most reported series. There is a trend toward AA/VSD patients having more primary repairs and IAA/VSD more staged repairs.13,14,18 Primary neonatal repair achieves a biventricular circulation and normal oxygen saturation from the outset but is extensive surgery including creating an intracardiac baffle in a neonate. It also limits the size of the RV-PA conduit that can be used. Staged repair has the advantage of reducing the complexity of the neonatal procedure and delaying the biventricular repair to an older age can make the intracardiac baffle easier and allow a larger conduit to be placed. However, this exposes the patients to an interstage period with cyanotic circulation and concomitant risks.16,17 Despite these theoretical advantages of a staged approach, there is no conclusive evidence that primary repairs have a higher number of LVOT re-interventions 22 or that postoperative heart block and subsequent permanent pacemaker placement occurs more in the primary group.
Most case series include a mixture of both approaches and there is no consistent rationale for one over the other. There are only 2 comparative studies of outcomes in primary and staged approaches, both finding no statistical difference in survival between the 2 strategies (5-year survival of 80-89% with primary and 73-75% with staged repair).7,13 A recent study by Alhadi et al 18 reported both groups had 100% survival at 5 years. Pearl et al 8 is the sole study to include only the staged approach finding excellent results with no operative mortality. Two series examined only primary repairs with very good outcomes with zero operative death 9 and 82% 10-year survival. 10 Series reporting primary repairs certainly include those with some of the best outcomes, but there is insufficient data to say which strategy is preferable and both seem reasonable. The increased popularity of the Norwood with RV-PA conduit certainly makes the staged approach a natural choice for those who prefer this technique for their Norwood procedures and may explain why a staged approach continues to be widely used. Occasional patients have undergone interim bidirectional cavopulmonary connection prior to Yasui, such that their final circulation is a 1½ type circulation. This appeared to have been performed simply to allow the Yasui to be performed at an older age rather than any specific concern regarding the size of the RV (which is generally reported as normal).
Yasui Versus Ross-Konno
In patients with AA/VSD, the Yasui is the only surgical option. However, in the group of patients with LVOTO and VSD then either a Ross-Konno or Yasui could be employed, so long as the VSD position and size are suitable for committing to the pulmonary artery. There are very few studies that have attempted to compare the outcomes of these 2 approaches11,12,17 and none are able to identify specific morphological factors that might favor one over the other. The CHSS cohort 12 of patients with critical LVOTO attempted to review these approaches but the 2 groups were not strictly comparable as most of the Ross patients did not have a VSD (and so Yasui could never have been an option), most had undergone previous aortic valve interventions, and many (40%) had associated mitral valve disease. Consequently, the outcomes for the Ross-Konno group were very poor—although if patients with mitral valve disease were excluded then the outcomes were similar to that of the Yasui group. 12
Two other studies11,17 have attempted comparisons, both with high early mortality in the neonatal Ross-Konno group (15-19%11,17) and a higher number of early complications—although freedom from reoperation for both the LVOT and RV-PA conduit change was similar in both groups.11,17 There is some evidence that the RV-PA conduit performs better in the Ross group than the Yasui, but the total re-intervention rates are similar in both groups. They conclude that although both options are reasonable, the Yasui is the preferred technique so long as the VSD is suitable for committing to the pulmonary valve.
Conclusion
The Yasui or Norwood-Rastelli provides excellent outcomes for the biventricular repair of AA/VSD and complex LVOTO with large VSD, the latter commonly associated with IAA. Both primary neonatal repair and staged strategies have been used and both approaches are reasonable, mainly guided by institutional preference. There is a trend for primary repair in AA/VSD and staged repair in IAA/VSD. Late mortality is rare and conduit replacement is the major re-intervention with excellent freedom from LVOT re-operation. In infants with complex LVOTO/VSD, surgical options include conventional repair, Yasui, or Ross-Konno. Aortic annulus size and z-scores help guide decision making. The Ross-Konno is an alternative for patients with complex LVOTO if the aortic root size is adequate. Although there are no truly comparative studies, prior reports suggest Yasui is preferable as long as the VSD size is adequate.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.