
Abstract
Background:
Anomalous aortic origin of a coronary artery (AAOCA) is a significant cause of sudden cardiac death (SCD) in children and adolescents. The natural history of AAOCA and the pathophysiology of AAOCA-related SCD are poorly understood. Therefore, the evaluation and management of AAOCA remain controversial. This survey-based study aims to report the current AAOCA management tendencies in Canada.
Methods:
We built a 23-question survey on AAOCA. Questions pertained to patient presentation, investigations, morphology of the anomaly, management, and follow-up. We sent the survey to all the Canadian congenital cardiac surgeons, pediatric cardiologists, and adult congenital cardiologists. Data were anonymized and analysis was performed using descriptive statistics.
Results:
According to our survey participants (N = 47), patient age (94%) and amount of physical activity (60%) are the most influential factors when deciding whether to offer surgical correction. Aborted SCD, exercise-induced syncope, typical chest pain, and left jaw or arm pain are the most important clinical presentations indicating surgery. The most commonly used preoperative investigations are rest echocardiography (75%), electrocardiogram (68%), and exercise stress test (62%). Most respondents favor the unroofing procedure (78%) for surgical correction. For nonsurgical candidates, most physicians choose competitive exercise restriction (64%).
Conclusion:
We found a divergence between current practices and expert consensus guidelines regarding the treatment of asymptomatic left AAOCA with high-risk features. Our survey also revealed a lack of consensus among clinicians regarding the management of asymptomatic patients, very young patients, and those with right-sided AAOCA. Evidence-based criteria derived from sufficiently powered studies remain to be established to standardize AAOCA treatment.
Introduction
Anomalous aortic origin of a coronary artery (AAOCA) is the second most common cause of sudden cardiac death (SCD) in children and adolescents, after hypertrophic cardiomyopathy. 1 –3 This is a rare congenital anomaly in which the left, right, or both coronary arteries do not originate from their respective sinus of Valsalva and follow an abnormal course. The prevalence of AAOCA has been estimated at 0.06% to 0.9% for anomalous right coronary artery (ARCA), 0.025% to 0.15% for anomalous left coronary artery (ALCA), and 0.02% to 0.67% for anomalous circumflex coronary artery. 4 –6 However, the exact prevalence of AAOCA remains unknown because most patients are likely asymptomatic. 7 When symptomatic, patients most often present with angina, syncope, or dyspnea on exertion.
Because the natural history of AAOCA and the pathophysiology of AAOCA-related SCD are poorly understood, AAOCA evaluation and management remain controversial. 3,8 Most agree that ALCA and AAOCA causing myocardial ischemia should both warrant surgical treatment. 8 A greater uncertainty remains for the treatment of patients without symptoms, especially those with ARCA. 2,3,8 Growing use and technological progress in imaging modalities lead to an increase in incidental detection of AAOCA in patients undergoing cardiac imaging for another reason than AAOCA investigation, which resulted in an expansion of the pool of asymptomatic patients and intensification of the already-existing uncertainty in the management of AAOCA.
The present state of knowledge and lack of evidence-based guidelines explains not only the low comfort level of physicians when facing AAOCA but also the discrepancies in patient care. This survey-based study aims to report the current AAOCA management tendencies in Canada.
Material and Methods
After reviewing the current literature, we built an online 23-question survey on AAOCA (Online Appendix S1). Questions pertained to patient presentation, diagnostic investigations, morphology of the anomaly, management, and follow-up.
We searched the email addresses of all the Canadian congenital cardiac surgeons, pediatric cardiologists, and adult congenital cardiologists using physician group email databases, Faculty pages of Canadian university websites, and corresponding author information on published articles. A total of 118 survey recipients were identified. We sent the link to our survey by email to all the recipients, followed by two reminder emails in the subsequent months, destined to those who had not yet answered.
Data were anonymized and analysis was performed using descriptive statistics. Categorical variables were processed with frequency counts and percentages.
Our project was approved by the McGill University Faculty of Medicine and Health Sciences institutional research ethics board. Since a waiver of consent was granted for this study, the documentation of explicit consent from the study participants was not performed. Nonetheless, survey participants were informed of our intention to disseminate the anonymized data from the survey through scientific presentations and/or publications. Therefore, their consent was implied by their completion of the survey.
Results
Survey Respondents
A total of 47 physicians responded to the survey (39.8% response rate). Of which, 68.1% were pediatric cardiologists, 21.3% congenital cardiac surgeons, and 10.6% adult congenital cardiologists. Thirty-four percent of the respondents had been in practice for over 20 years, 51% had started their career between 5 and 20 years, and 15% started practicing less than five years prior to the survey. Thirteen Canadian universities and six provinces were represented among respondents. Among the nonrespondents, 78.7% were pediatric cardiologists, 3.7% were surgeons, and 17.5% were adult congenital cardiologists. All survey recipients (respondents and nonrespondents) worked primarily in an academic center, since, in Canada, pediatric and congenital cardiology and cardiac surgery care is centralized to university-affiliated institutions.
Clinical Presentation
Our respondents thought that aborted SCD, exercise-induced syncope, typical chest pain (defined as substernal chest pain or discomfort that was provoked by exertion or emotional stress and was relieved by rest and/or nitroglycerin), and left jaw or arm pain were the most important clinical presentations indicating surgery. When deciding whether to refer a patient to surgery, age (93.6%) and amount of physical activity (59.6%) were the most influential variables. In addition, for patients in which AAOCA is detected incidentally, surgery is only considered by 12.8% of respondents for patients less than 12 months old and by 23.4% for patients between one and five years old. In contrast, surgery is offered by 80.9%, 76.6%, and 74.5% of the respondents for patients with an incidental finding of AAOCA aged 10 to 15, 15 to 20, and >20 years, respectively.
Investigations
When asked which types of studies were preferred as first-line investigation modalities in patients with suspected AAOCA, rest echocardiogram (75%), electrocardiogram (68%), and exercise stress test (62%) were the most popular answers. Nuclear myocardial perfusion scans (9%) and coronary angiograms (2%) are rarely used as first-line modalities by our survey participants (Table 1). Diagnostic modalities most commonly used as second-line were coronary angiogram (51%), computed tomography angiogram (49%), and nuclear myocardial perfusion scan (40%).
Preferred First- and Second-Line Investigation Modalities in Patients With Suspected AAOCA Among Survey Respondents.
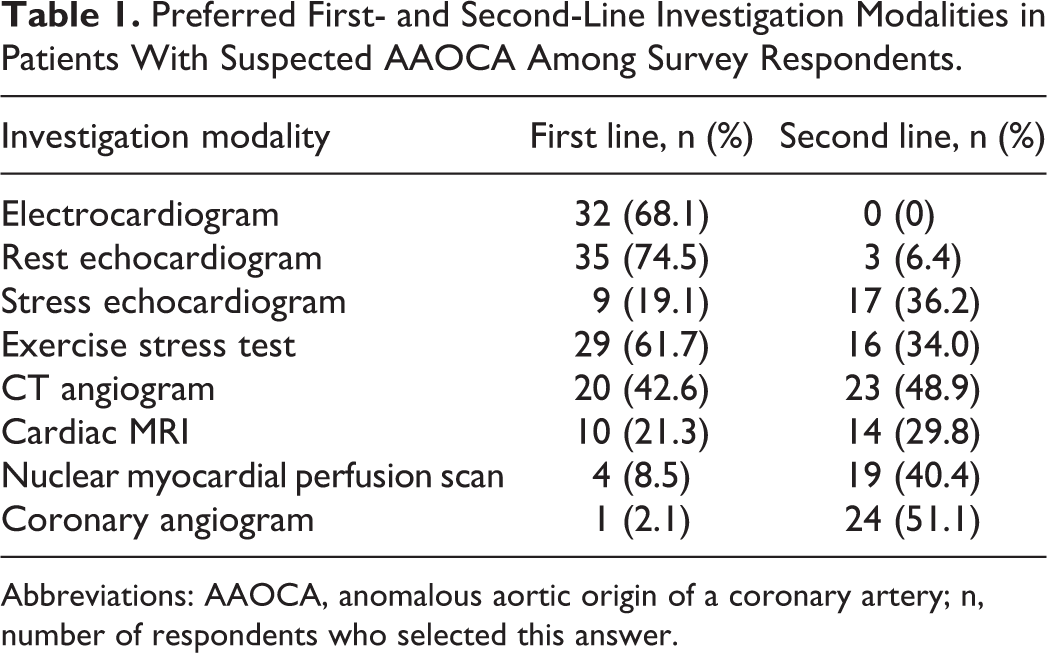
Abbreviations: AAOCA, anomalous aortic origin of a coronary artery; n, number of respondents who selected this answer.
Anomalous Aortic Origin of a Coronary Artery Morphology
According to our respondents, the morphological features causing the highest risk for SCD were in decreasing order of importance, slit-like, elliptic or stenotic ostium, intramural course, interarterial course, and left-sided AAOCA.
Management
When asked to choose a management strategy for a patient with left AAOCA and high-risk features, answers varied greatly depending on the age of the patient. For a teenager, 93.7% of physicians responded surgical repair, 2.1% answered observation, 2.1% chose complete activity restriction, and 2.1% opted for competitive exercise restriction (Figure 1). For a very young child (18 months old), 42.6% answered surgery, 25.5% chose parent counseling on risks of physical activity, 23.4% opted for observation, and 8.5% responded medication (Figure 1). When separating the surgeons’ answers from those of the cardiologists, we obtained the following breakdown: 30% of the surgeons answered surgical management (vs 45.9% for cardiologists), 20% chose parent counseling (vs 27% for cardiologists), 40% selected observation (vs 18.9% for cardiologists), and 10% responded medication (vs 8.2% for cardiologists).
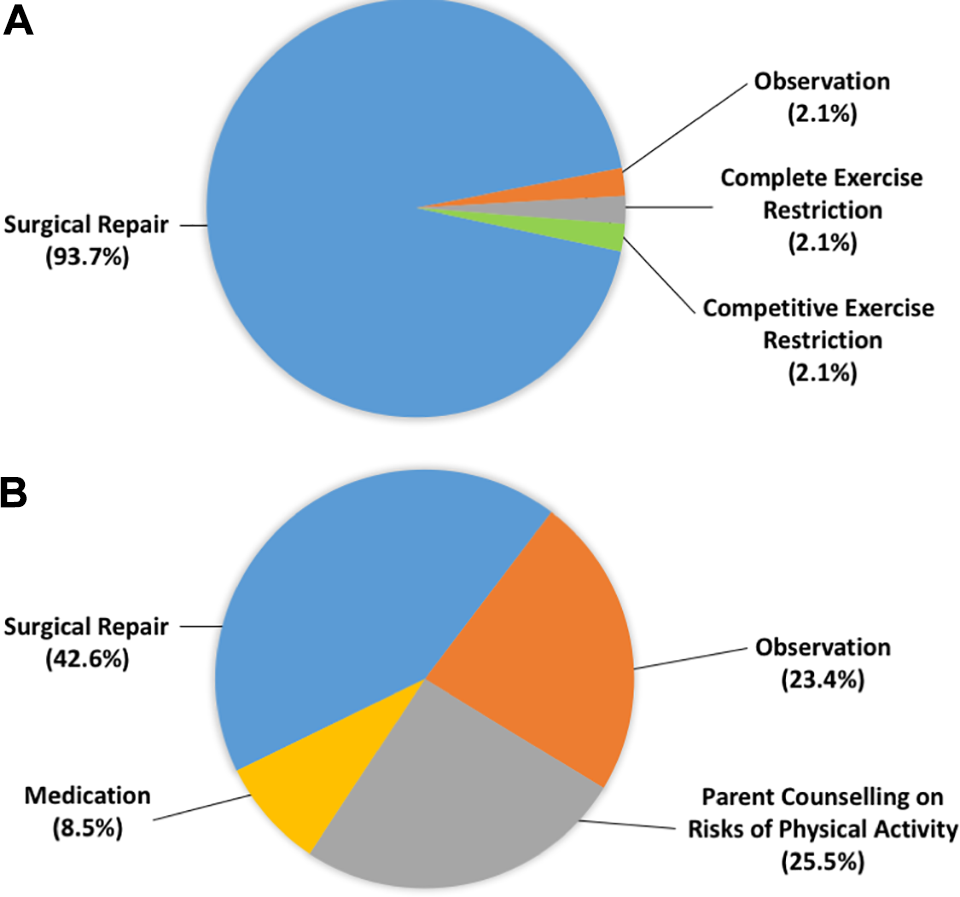
Preferred management of teenagers (A) and very young children (B) with left anomalous aortic origin of a coronary artery (AAOCA) and high-risk features. The teenagers’ management was almost unanimously surgical repair, whereas it was much more controversial for very young patients.
The management of asymptomatic teenage athletes with left AAOCA and no high-risk features was divided between surgery (40.5%), observation (38.1%), and competitive exercise restriction (21.4%; Figure 2). For symptomatic teenagers with right AAOCA and no high-risk features, 72.3% of physicians opted for observation, 17% chose competitive exercise restriction, 8.6% answered surgical management, and 2.1% chose pharmacotherapy (Figure 3).
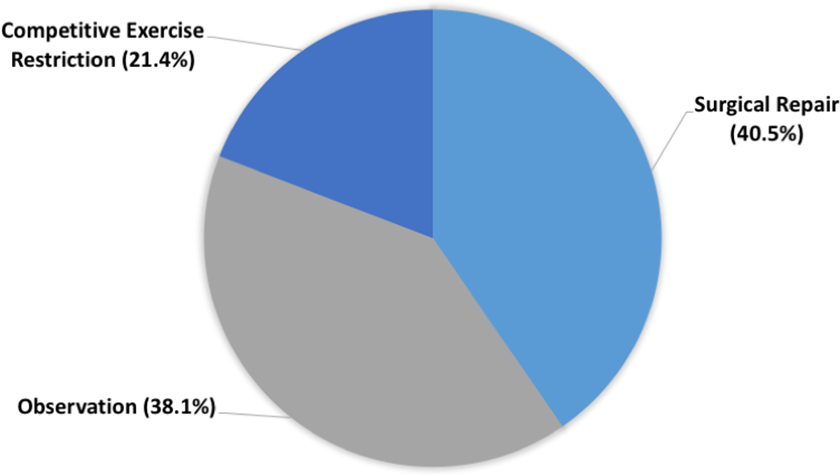
Management of asymptomatic teenage athletes with left anomalous aortic origin of a coronary artery (AAOCA) and no high-risk features.
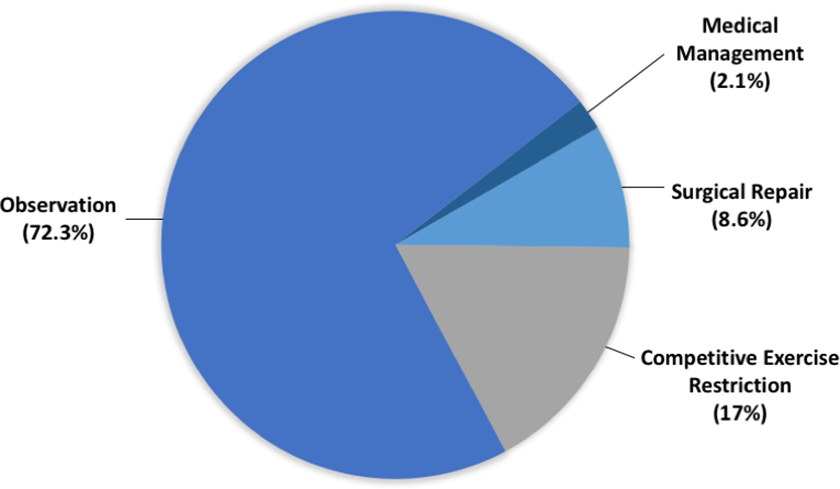
Management of symptomatic teenagers with right anomalous aortic origin of a coronary artery (AAOCA) and no high-risk features.
With regard to absolute indications for surgical repair, aborted SCD (100%), positive stress testing (95.7%), and clinical manifestations of ischemia such as chest pain (85.1%) were the most popular answers. Most surgeon respondents (77.8%) favored the unroofing procedure for correction of AAOCA. Anatomical repair (11.1%), as proposed by Vouhé, 8 and pulmonary artery translocation (11.1%) were the second most preferred surgical techniques for AAOCA patients (Figure 4).
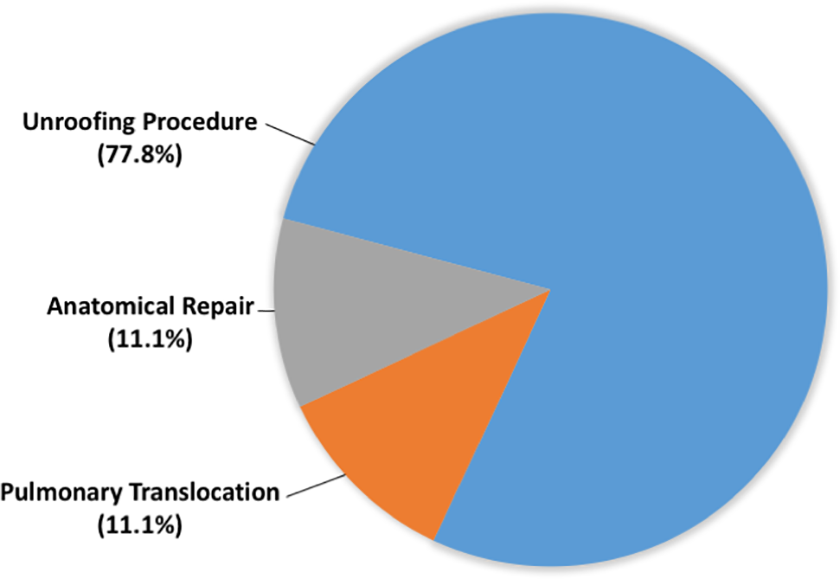
Preferred surgical techniques for correction of anomalous aortic origin of a coronary artery (AAOCA). This question was only asked to surgeon respondents.
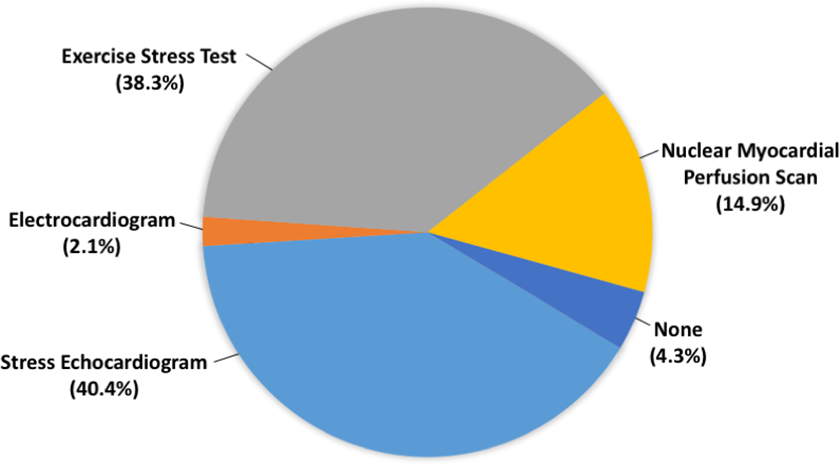
The minimal age at which patients with high-risk features (intramural course, interarterial course, slit-like ostium, acute angulation) should receive surgery varied greatly among respondents. In all, 38.3% believed there was no minimal age for surgery, 19.1% answered 10 to 15 years of age, 27.7% 5 to 10, and 14.9% 1 to 5 years of age (Figure 5). Most physicians manage patients too young for surgery with complete exercise restriction (63.8%) and pharmacotherapy (61.7%) when symptomatic and with competitive exercise restriction (57.4%) and observation (48.9%) when asymptomatic (Table 2). Medical treatment for patients awaiting surgery was recommended for all patients by 23.4% of respondents and for symptomatic patients by 40.4% of respondents (Figure 6).
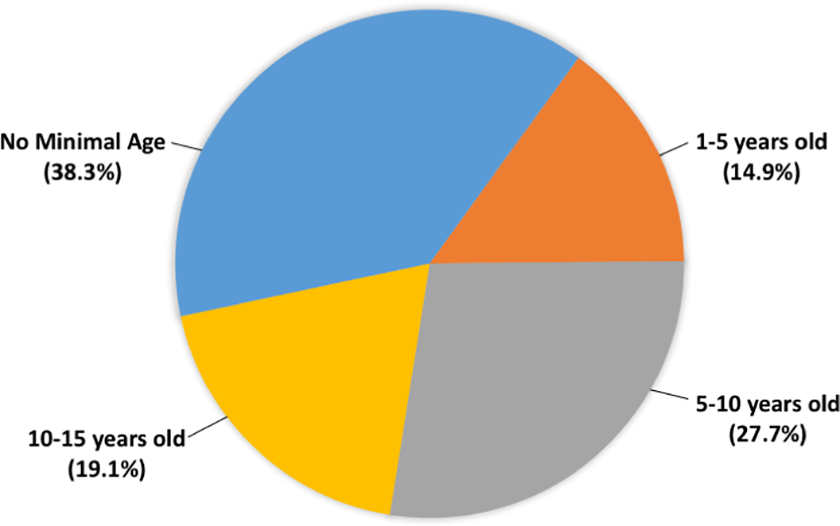
Minimal age at which patients with high-risk features (intramural course, interarterial course, slit-like ostium, acute angulation) should be referred for surgery according to our respondents.
Management Strategy of Symptomatic and Asymptomatic Patients With AAOCA Who Are Awaiting to Become Surgical Candidates.
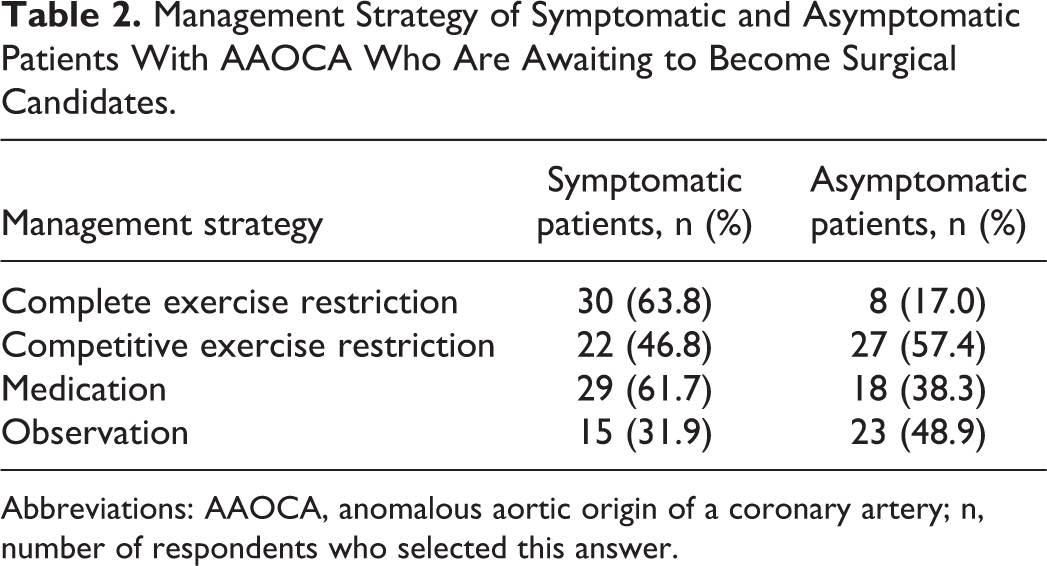
Abbreviations: AAOCA, anomalous aortic origin of a coronary artery; n, number of respondents who selected this answer.
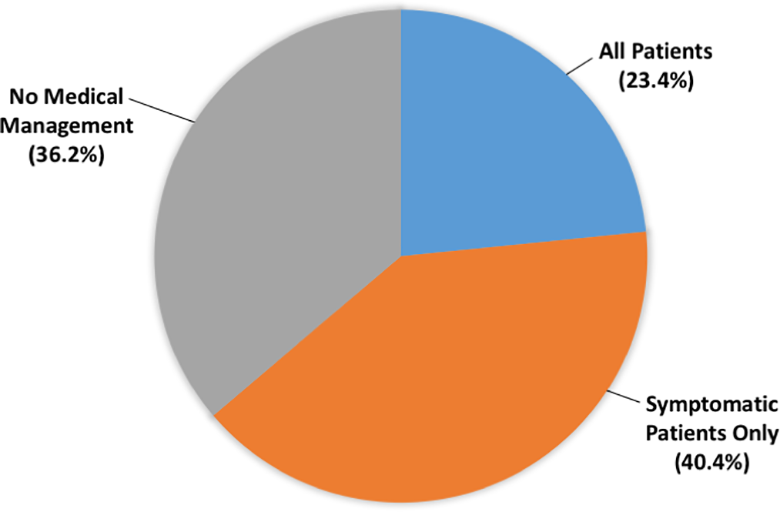
Proportions of respondents who use medical management in patients awaiting surgery.
Follow-Up
Postoperative patients are followed yearly by 46.8%, every three months by 12.8% and every six months by 29.8% of physicians. The most popular investigation modalities used for postoperative follow-up were stress echocardiography (40.4%) and exercise stress test (38.3%; Figure 7). In all, 74.5% of physicians recommend no exercise restriction for postoperative patients, while 25.5% recommend competitive exercise restriction. Thirty-two percent of respondents do not use pharmacotherapy after surgery, 66% prescribe aspirin, 19.1% use β-blockers. Lipid-lowering agents (8.5%) and nonaspirin antiplatelet agents (4.3%) are also used by some respondents (Figure 8).
Preferred investigation modalities for postoperative patients.
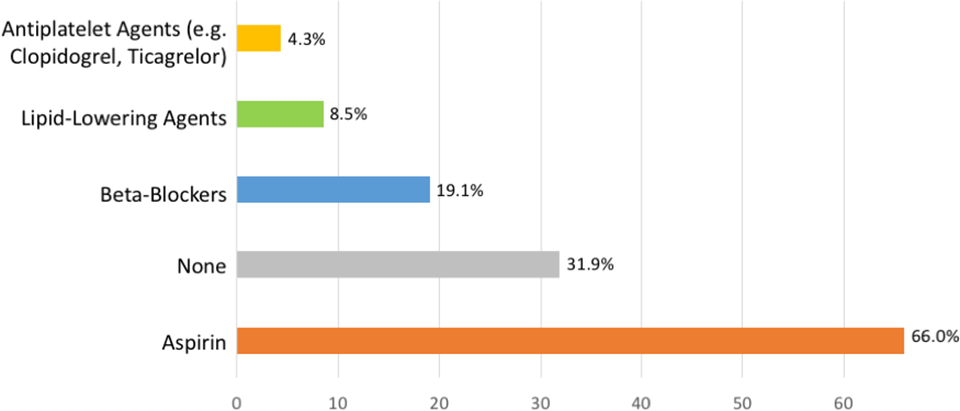
Long-term pharmacological management of postoperative patients after anomalous aortic origin of a coronary artery (AAOCA) correction. Participants could select multiple answers.
Comment
The main goal of our survey was to evaluate the current management of patients with AAOCA in Canada. We found that investigation and management practices diverge among our respondents, especially for young children, asymptomatic patients, and those with ARCA.
The American Association for Thoracic Surgery (AATS) recently published expert consensus guidelines on anomalous coronary arteries. 9 Recommendations on diagnostic imaging included the use of transthoracic echocardiography in individuals with suspected AAOCA to identify the origin and course of the proximal coronary arteries (Class I, Level of Evidence B). 9 Our results mostly converge with this statement, as 74.5% of our respondents use rest echocardiography as a first-line investigation. The AATS also advocates the use of exercise stress testing in patients without a history of ischemic chest pain or aborted SCD to help assess the ischemic burden of the anatomic variant (Class I, Level of Evidence B). 9 Of our respondents, 61.7% commonly use exercise stress testing as a first-line investigation. Interestingly, a majority (68.1%) of our participants also use electrocardiography as a first-line modality. However, Roberts and colleagues found that electrocardiography is not a suitable modality for screening or identifying individuals with AAOCA. 10 In fact, signs of ischemia such as Q-waves are rarely found in AAOCA patients. 9 Moreover, stress cardiac magnetic resonance imaging is a rising clinical assessment tool that can be used in the pediatric population for evaluation of myocardial perfusion. 11,12 This imaging modality can facilitate patient risk stratification and better correlate the morphology of each patient’s AAOCA to their degree of myocardial ischemia.
In their recent Scientific Statement, the American Heart Association and American College of Cardiology advocate for differentiation between interarterial ALCA and interarterial ARCA, as the former is thought to correlate with a much higher risk of SCD. 13 Moreover, prior to clearing patients from competitive exercise restriction, a stress test should be performed to rule out ischemia. 9,13 For the management of symptomatic patients with ARCA and no high-risk features, 72.3% of our respondents chose observation (Figure 3); however, the most recent AATS guidelines recommend surgical repair and exercise restriction. In fact, these guidelines state that individuals with AAOCA with symptoms of ischemic chest pain, aborted SCD, or syncope suspected to be due to ventricular arrhythmia should be activity restricted and offered surgery (Class I, Level of Evidence B). 9 The management of asymptomatic ALCA patients with no high-risk features was very much divided among our respondents (Figure 2). Brothers et al state that once ischemia is ruled out with a stress test, ALCA patients with low-risk features do not require surgery or competitive exercise restriction. 9 Low-risk ALCA features include prepulmonic and retroaortic courses, and they only rarely cause ischemia. 7,9 The intraseptal course of a coronary artery is also considered a benign feature; however, in a recent cohort study, Doan and colleagues found that it can be associated with inducible myocardial perfusion. 14
Among our respondents, the management of asymptomatic patients with high-risk ALCA depended greatly on the age of the individual. In fact, for a teenager, almost all survey participants opted for surgical repair, while for a very young patient (<two years old), the answers were much more divided (Figure 1). Although age was a popular variable when deciding whether to offer surgery, there are currently no guidelines on the minimal age for surgical repair, and the timing of surgical intervention remains controversial. 15 Interestingly, when we compare the surgeons’ answers from those of the cardiologists, we find that cardiologists have a lower threshold than surgeons for recommending surgical management of very young patients with high-risk ALCA. This may be partly explained by the differing perspectives of surgical versus nonsurgical physicians. For instance, congenital cardiac surgeons are likely to better appreciate the incremental technical difficulties involved in operating on very young and small patients. Surgeons are therefore likely more inclined to delay surgical correction, whenever possible, to allow for patients to grow, which theoretically decreases surgical risk and complexity.
In addition, the use of medical therapy such as β-blockers and aspirin for very young patients with high-risk features and for small patients awaiting to become surgical candidates was a common answer among our respondents. Although there is currently no strong evidence to support the use of medication in AAOCA, practicing physicians may still elect to use it. We therefore decided to include medical therapy as part of our answer choices.
Several surgical procedures are available for AAOCA correction. However, there has been no formal comparison between approaches; hence, superiority of one of them has not been determined. 9,16 The choice of a surgical approach over another depends on the morphology of the anomaly. For instance, intramural lesions are often repaired with coronary unroofing. 15,17 This procedure can be performed safely, but symptoms can persist despite normal postoperative testing. 18 Nonintramural lesions are often not amenable to unroofing and are rather managed with coronary artery reimplantation, ostial plasty, and pulmonary artery translocation. 19 Rarely, coronary artery bypass grafting (CABG) can be performed in AAOCA, but it is associated with a high rate of symptom recurrence, namely because of substantial competitive flow, especially when the native coronary artery is not ligated. 7,20 For this reason, CABG is usually reserved for older patients with concomitant atherosclerotic coronary artery disease. 9 Another surgical approach, the anatomical repair, was proposed by Vouhé. 8 This method may be favorable because it creates an enlarged neo-ostium in the appropriate sinus, restores a normal take-off angle, and eliminates the intramural segment. 21
The optimal follow-up strategy for patients with AAOCA is another source of uncertainty among physicians. This has been depicted by our survey results, namely with regard to frequency of follow-up and investigation modalities. According to the AATS Expert Consensus Guidelines on AAOCA, 9 patients who undergo surgical intervention for AAOCA should have a lifelong follow-up with a cardiologist, as long-term effects of surgery remain largely unclear. In fact, patients who initially present with aborted SCD and undergo surgical repair may remain at risk of SCD once they return to exercise postoperatively. 22 For this reason, patients with aborted SCD should only return to competitive exercise at least 12 months after surgery, and only if they remain free of ischemic symptoms and if exercise stress testing does not show evidence of ischemia or high-risk arrhythmias. In contrast, postoperative patients without prior history of aborted SCD may likely return to recreational and competitive exercise after three months, if they remain symptom-free and if their exercise stress test is negative postoperatively. 9 Establishment of presence or absence of postoperative ischemia is therefore essential to guide follow-up and postoperative management strategy. Brothers and colleagues performed a prospective cohort study with 24 patients who underwent surgical intervention for AAOCA and found that nine (37%) patients had postoperative evidence of myocardial ischemia. 23 Similarly, in a recent prospective cohort study by Mery et al, 7% of patients had postoperative chest pain and 14% had an abnormal stress nuclear perfusion scan. The results of these two cohorts illustrate how postoperative ischemia remains relatively common and should therefore be carefully assessed with functional testing.
Although we believe our survey positively contributes to the AAOCA literature, this study has several limitations. Firstly, with a response rate of 39.8%, there may be a risk of nonresponse error, because nonrespondents may have a different perspective from that of respondents. However, we believe the nonrespondent group is likely similar to the respondent group in terms of the type of practice. In fact, in Canada, the pediatric and congenital cardiology and cardiac surgery care are concentrated in university-affiliated centers, the majority of which were represented among our participants (13 of the 17 centers). Secondly, we did not have access to the email addresses of some of the cardiologists, especially those working in less research-heavy centers, which might have skewed our results. Lastly, wanting to keep the survey as succinct as possible, we chose not to split the management questions by severity of symptoms and by AAOCA morphology, which may have influenced the answers of some of our participants.
In conclusion, our national survey revealed a lack of consensus among clinicians for the management of AAOCA. We found discordance between standard clinical practices and current guidelines. Most notably, physicians do not all offer surgical correction to patients with ALCA and high-risk features, especially when patients are below two years old. Other points of divergence between the current management of AAOCA and expert recommendations include the approach to symptomatic ARCA with no high-risk features and to asymptomatic ALCA without high-risk features. Because AAOCA is a rare disease, building evidence-based guidelines with sufficiently powered studies remains challenging. Multicenter data registries, such as the Congenital Heart Surgeons’ Society Registry of Anomalous Aortic Origin of a Coronary Artery, 24 have been funded to address this challenge by collecting clinical information on a larger number of patients. The ultimate goals of such collaborations is to better understand the natural history of this congenital defect and to build evidence-based management guidelines. This will hopefully reduce the clinicians’ knowledge gap and standardize practices.
Supplemental Material
Supplemental Material, sj-docx-1-pch-10.1177_2150135121999030 - Current Management of Anomalous Aortic Origin of a Coronary Artery: A Pan-Canadian Survey
Supplemental Material, sj-docx-1-pch-10.1177_2150135121999030 for Current Management of Anomalous Aortic Origin of a Coronary Artery: A Pan-Canadian Survey by Kenza Rahmouni and Pierre-Luc Bernier in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Abbreviations
Authors’ Note
The authors of this manuscript had full control of the design of the study, methods used, outcome parameters, analysis of data, and production of the written report. They did not receive any financial, property, or intellectual aid from a commercial source. The McGill University Faculty of Medicine and Health Sciences Institutional Review Board (Montreal, Quebec, Canada) approved this study and granted a waiver of consent.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.