
Abstract
Objective:
Technical performance score (TPS) has been associated with both early and late outcomes across a wide range of congenital cardiac procedures. A previous study has shown that the presence of residual lesions before discharge, as measured by TPS, is accurately able to identify patients who required postdischarge reinterventions after complete atrioventricular septal defect (CAVSD) repair. The aim of this study is to determine which subcomponents of TPS best predict postdischarge reinterventions after CAVSD repair.
Methods:
This was a single-center retrospective review of patients with CAVSD after repair between January 2000 and March 2016. We assigned TPS (class 1, no residua; class 2, minor residua; class 3, major residua or reintervention before discharge for residua) based on subcomponent scores from discharge echocardiograms. Outcome of interest was postdischarge reintervention.
Results:
Among 344 patients, median age was 3.2 months (interquartile range [IQR], 2.4-4.2). There were 34 (10%) postdischarge reinterventions. Median follow-up was 2.6 years (IQR, 0.09-7.9). Trisomy 21 and concomitant procedure were associated with postdischarge reinterventions. After adjusting for these factors, among the subcomponents, left atrioventricular valve stenosis and regurgitation, right atrioventricular valve regurgitation, residual ventricular septal defect, and abnormal conduction at discharge were significantly associated with postdischarge reinterventions.
Conclusions:
We demonstrated the ability of TPS to predict postdischarge reinterventions in patients who underwent CAVSD repair. Residual left and right atrioventricular valve regurgitation and abnormal conduction at discharge were among the subcomponents strongly associated with postdischarge reinterventions. Thus, TPS may aid clinicians in identifying children at higher risk for reintervention.
Better understanding of the anatomy and optimization of surgical techniques have improved early clinical outcome of surgical correction of complete atrioventricular septal defects (CAVSDs). However, several studies report a high risk of reoperation (up to 10%). 1 Technical performance score (TPS), a tool developed to determine technical adequacy of congenital cardiac repairs, has been shown to be an important predictor of both early and midterm outcomes across a wide range of congenital cardiac procedures. 2 A previous study has shown that the presence of residual lesions before discharge, as measured by TPS, accurately identifies patients requiring postdischarge reinterventions (PD-RI). 3 However, in this previous study, overall TPS was used to determine the association between TPS and PD-RI. The association between individual subcomponents of TPS and PD-RI was not investigated. The aim of this study is to determine which subcomponents of TPS best predict PD-RI.
A review of consecutive patients with balanced CAVSDs who were operated on at a tertiary care center between January 2000 and March 2016 was performed with institutional review board approval. Demographic, echocardiographic, and follow-up data were obtained. Primary complete repair of CAVSD was considered the index operation. Only patients discharged alive without heart transplantation were analyzed. Patients with associated major intracardiac anomalies or partial/transitional AVSD were excluded. Postoperative TPS was determined as previously reported 3 based on predischarge echocardiographic findings and clinical status at discharge from the index operation. The TPS for CAVSD repair included the following subcomponents: size of residual atrial septal defect, size of residual ventricular septal defect (VSD), severity of right and left atrioventricular valve (AVV) stenosis and regurgitations, status of the patent ductus arteriosus, and status of the conduction system. Each subcomponent was assigned a score of class 1 (optimal, trivial, or no residua), class 2 (adequate and minor residua), or class 3 (inadequate and major residua), based on specific echocardiographic criteria. 3 The final TPS was based on the subcomponent scores and was class 1 if all subcomponents received a class 1 score, class 2 if one or more of the subcomponents were class 2 but none were class 3, and class 3 if any of the subcomponents were class 3. Any unplanned surgical or catheter-based reintervention for residua in the anatomic area repaired during the CAVSD operation or the need for permanent pacemaker (PPM) placement prior to discharge from index CAVSD surgery resulted in a class 3 (inadequate) score. The outcome variable, PD-RI, was defined as surgical or catheter-based reinterventions that occurred following discharge from index CAVSD surgery on anatomic areas repaired at CAVSD operation, including placement of PPM.
Forward selection was used to develop a multivariable Cox regression model of baseline patient factors associated with time to PD-RI; P < .05 was required for retention in the final model. Qualitative TPS and its subcomponents were then added to this model. Hazard ratios were estimated with 95% confidence intervals. Statistical analysis was performed with SAS version 9.4 (SAS Institute Inc, Cary, North Carolina).
There were 344 patients included in the analysis. There were 211 (61%) females, 67 (19%) were premature, and 305 (89%) had some form of genetic anomaly. The median age at operation was 3.2 months (interquartile range [IQR], 2.4-4.2 months). There were 34 (10%) PD-RI.
Trisomy 21 and concomitant procedure were associated with PD-RI. After adjusting for these factors, among the subcomponents, left AVV stenosis and regurgitation, right AVV regurgitation, residual VSD, and abnormal conduction at discharge were significantly associated with PD-RI (Table 1).
Multivariable Model, Subcomponents of TPS, and Postdischarge Reinterventions (n = 344).a
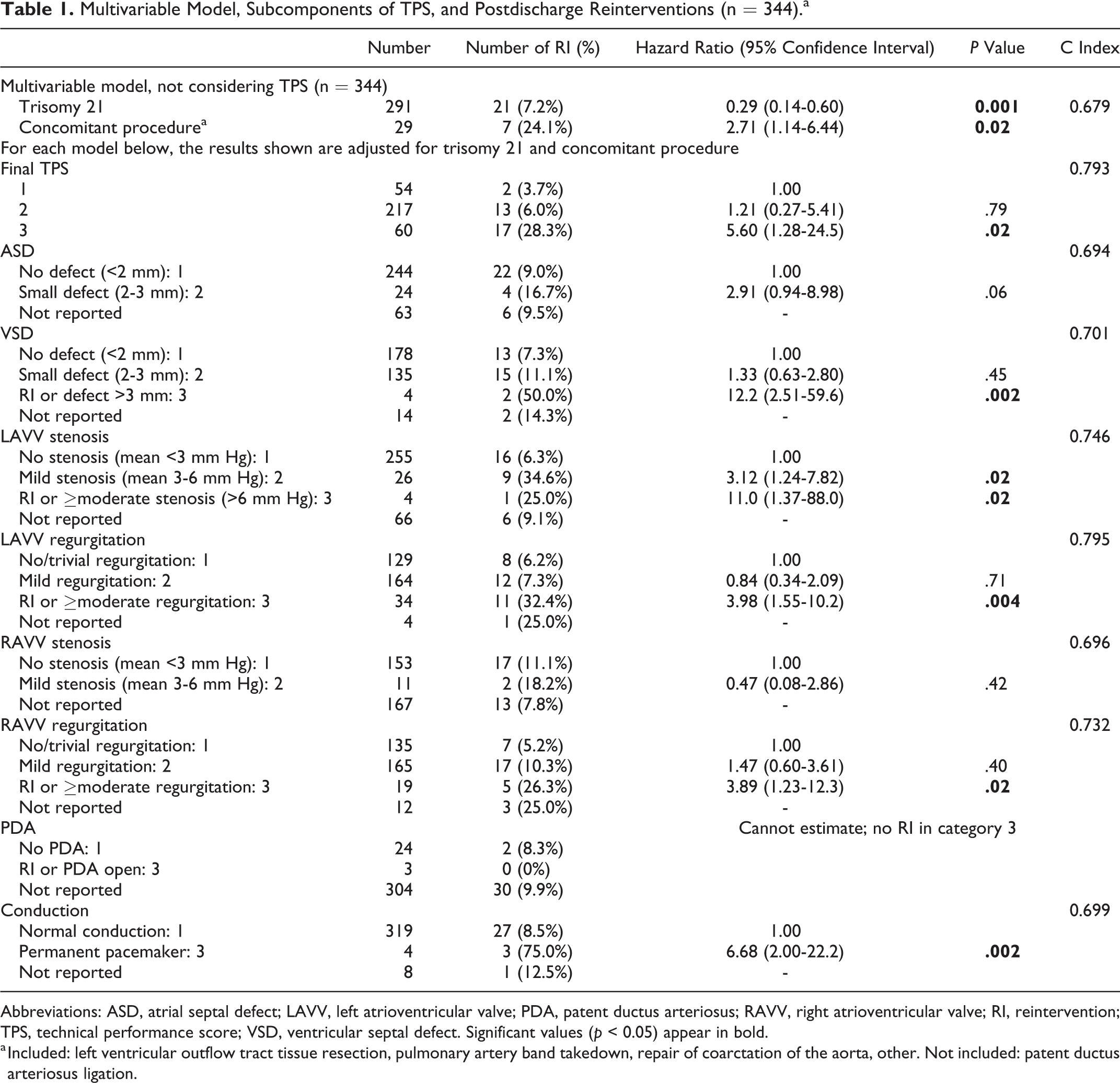
Abbreviations: ASD, atrial septal defect; LAVV, left atrioventricular valve; PDA, patent ductus arteriosus; RAVV, right atrioventricular valve; RI, reintervention; TPS, technical performance score; VSD, ventricular septal defect. Significant values (p < 0.05) appear in bold.
a Included: left ventricular outflow tract tissue resection, pulmonary artery band takedown, repair of coarctation of the aorta, other. Not included: patent ductus arteriosus ligation.
A potential limitation of this study is that it represents a single center’s experience with TPS using retrospective data with its inherent problems of missing and incomplete data, although only 4% of our patient population had missing qualitative echocardiographic data at discharge.
We demonstrated the ability of TPS to predict PD-RI in patients who underwent CAVSD repair. Residual left and right AVV regurgitation and abnormal conduction at discharge were among the subcomponents strongly associated with PD-RI. Thus, TPS may aid clinicians in identifying children at higher risk of future reinterventions who may benefit from more frequent follow-up.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.