
Abstract
Objectives:
Supravalvar aortic stenosis (SVAS) is a rare congenital anomaly. The “single-patch technique,” “‘two sinus augmentation with an inverted Y-patch” (both nonsymmetrical corrections), “three-patch technique,” and the “slide aortoplasty” (both symmetrical corrections) are the techniques implemented by the majority of surgeons for the correction of SVAS. In the few studies that compared these techniques, no technique was shown to be superior over another. The aim of the present study is to review the 52-year experience with the surgical correction of SVAS in two of four congenital cardiothoracic surgical centers in the Netherlands.
Methods:
We retrospectively reviewed all patient files of those who underwent an operation to correct their SVAS, between 1962 and 2014 in our centers. Patients were divided according to their operating technique. These groups were compared using the end points freedom from reoperation and mortality.
Results:
A total of 49 patients were included, 23 (46.9%) patients in the nonsymmetrical group and 26 (53.1%) patients in the symmetrical group. Survival after 20 years in the nonsymmetrical group was 80% (standard error [SE]: 0.091) and in the symmetrical group was 85% (SE: 0.085; P = .163). Freedom from reoperation after 20 years in the nonsymmetrical group was 88% (SE: 0.079) and in the symmetrical group was 71% (SE: 0.107; P = 0.313).
Conclusion:
In this patient group, there is no significant difference in survival and freedom from reoperation between the different surgical techniques for SVAS repair. Compared to the survival in the general population, the survival of SVAS patients is remarkably low. Apparently, SVAS is not a benign disease and probably patients should be followed more closely for the rest of their lives.
Keywords
Introduction
Supravalvar aortic stenosis (SVAS) is a rare congenital cardiac anomaly and a common feature of Williams-Beuren syndrome, but it also occurs as the result of an isolated autosomal dominant trait. 1,2 A deletion of the elastin gene causes narrowing of large elastic arteries like the aorta or pulmonary arteries. The narrowing of the aorta is seen characteristically in the supravalvar aorta at the sinutubular junction, this is the so-called “discrete” type of SVAS. When the stenosis extends into the ascending aorta, aortic arch, or the origin of the arch vessels, this is called the “diffuse” type of SVAS. 2,3 The incidence of discrete SVAS widely varies (14%-72%) in studies reporting their results of the surgical correction of SVAS. 4 –9 Several SVAS-associated lesions have been described: stenosis of the coronary arteries, bicuspid aortic valve, subvalvar aortic stenosis, and pulmonary stenosis. 3 Supravalvar aortic stenosis is known to be a progressive lesion. 4,5 Various variations in operative techniques have been described, which differ by the number of Valsalva sinuses that are augmented by (patch) repair. The “single-patch technique,” “two sinus augmentation with an inverted Y-patch” (both nonsymmetrical correction), and the “three-patch technique” (symmetrical correction) are the techniques implemented by the majority of surgeons for the surgical correction of SVAS (Figure 1). It is unknown whether any of these techniques leads to superior results. The aim of the present study is to review the 52 years’ experience with the surgical correction of SVAS in two of four congenital cardiothoracic surgical centers in the Netherlands
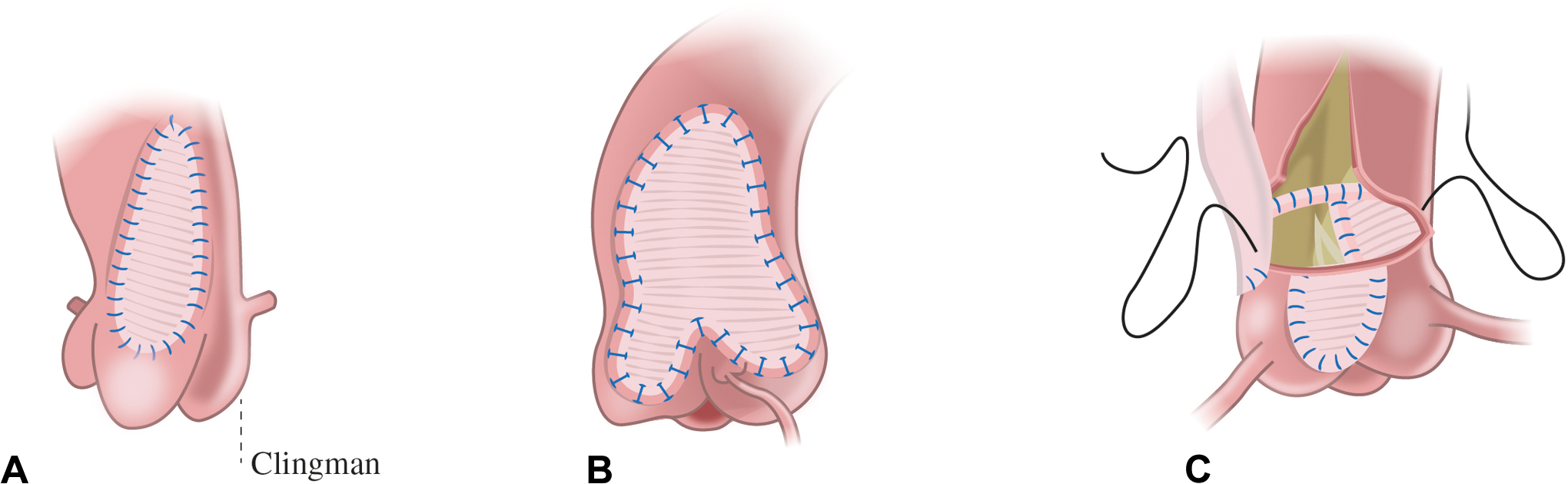
Three surgical techniques. A, Single-patch technique. B, Two-sinus augmentation with an inverted Y-patch. C, Three-patch technique.
Patients and Methods
Study Design and Setting
This is a retrospective observational study conducted in two centers in the Netherlands: the Center for Congenital Heart Diseases Amsterdam Leiden CAHAL that includes Leiden University Medical Center, Academic Medical Center Amsterdam, and Free University Medical Center Amsterdam ; and the University Medical Center Groningen. To collect data of all patients who underwent surgery for SVAS, the cardiology and cardiac surgery databases of the different institutions were reviewed. All patients who underwent surgery for SVAS from 1962 until 2014 in one of these centers were included. Patients were excluded when they had acquired postsurgical SVAS or when they underwent SVAS correction and aortic valve replacement in the same initial operation. This study was notified to the medical ethics committee, but because of the observational character of the study it is not part of the Wet Medisch-wetenschappelijk Onderzoek = Law Medical Research and did not need approval by the medical ethics committee.
Data Collection
We collected the following demographic and preoperative data: gender, date of birth, date of initial surgical SVAS correction, syndrome determined by genetic testing, previous cardiovascular operation, form of SVAS (discrete or diffuse), and concomitant preoperative cardiovascular anomalies. Operative data included the operation technique used at the initial surgical SVAS correction (divided in single-patch technique, two sinus augmentation, and three-patch technique; sliding plasty was not performed in our centers), additional surgical procedures at initial operation, patch material used, complications during the operation, and in-hospital complications during postoperative stay. Follow-up data included restenosis on echo, reoperations in the cardiovascular area, and mortality and were collected at the last follow-up appointment with the cardiologist. Any gradient over the supravalvular area that was higher than the gradient directly postoperative was considered a restenosis. The echocardiographic data of all available echocardiographs were analyzed by one cardiologist (R.B.), Z scores were used according to Pettersen et al. 6 Aortic valve disease was defined as valvular stenosis (from mild to severe), regurgitation (from mild to severe), bicuspid aortic valves, or adhesion of one or more leaflets to the supravalvular ridge. For every patient, the general practitioner was consulted in order to check the patients’ well-being. If a patient had deceased, as much as possible information were collected regarding the cause of death. End points were survival rate and freedom from reoperation.
Statistical Analysis
In order to identify significant differences in baseline characteristics between the two surgical groups (symmetrical vs nonsymmetrical), an independent-sample t test was performed for parametric continuous variables. For nonparametric continuous variables, the Mann-Whitney U test was used. For categorical variables, a χ2 test was used. When expected cell count was less than 5 in >20% of the cases, the Fisher exact test was used. A P value of <.05 was considered significant. The survival and reoperation-free survival of the symmetrical and nonsymmetrical groups were described using the Kaplan-Meier curves. The binary logistic regression analysis was used to compare survival rate and freedom of reoperation rate between the 2 groups at 20 years. Due to the observational character of the study, correcting for selection bias was indicated. This was done by performing a separate logistic regression analysis to assess the propensity score for each patient. Based on selected patient characteristics that are considered to be confounding factors, the propensity score predicts the chance that a patient will belong to the symmetrical or nonsymmetrical group. We considered sex, age at first SVAS correction operation, year of operation, presence of Williams syndrome, presence of pulmonary artery stenosis, and presence of aortic valve disease as potential factors to cause selection bias (confounders). We plotted the propensity scores to check whether the overlap was sufficient. The calculated propensity scores were then added to the model to correct the odds for mortality and freedom of reoperation. We used this logistic regression analysis to compare symmetrical and nonsymmetrical operating techniques in survival and reoperation-free survival. The statistical software system IBM SPSS 22 was used for data analysis.
Results
Patient and Operative Characteristics
From 1962 to 2014, a total of 49 patients underwent surgical relief of SVAS. Williams syndrome was present in 24 (49%) patients and Noonan syndrome in 2 (4.1%) patients . An isolated elastin (ELN) mutation was demonstrated in three (6.1%) patients, and in two cases no genetic test was performed. In 42 (85.7%) patients, SVAS was discrete and in 7 (14.3%) patients it was diffuse (Table 1). The mean age at the time of the first operation was 8.16 (standard deviation [SD] = 9.25) years (range: 0-45 years). This wide range is the result of a change in surgical practice over time. After 1974, all patients were operated on as children. Concomitant cardiovascular anomalies are specified in Table 2. Twenty-one (42.9%) patients needed additional procedures during their first SVAS operation. Four (8.2%) needed aortic arch surgery. Others underwent enlargement of pulmonary artery stenosis (n = 5), clipping of patent ductus arteriosus (n = 3), mitral valve repair (n = 3), aortic valve repair (n = 3), valvulotomy of the aortic valve (n = 2), and valvulotomy of the pulmonary valve (n = 1). In 15 (30.6%) patients, untreated autologous pericardium was used as patch material; in 20 (40.8%) patients, glutaraldehyde-treated autologous pericardium was used; in 10 (20.4%) patients synthetic material was used; in 2 (4.1%) patients dura mater was used; in 1 (2.0%) patient xenopericardium was used; and in 1 (2.0%) patient an aortic homograft was used to create a patch. The use of dura mater took place solely in the earlier years of our experience.
Baseline Characteristics: Preoperative.
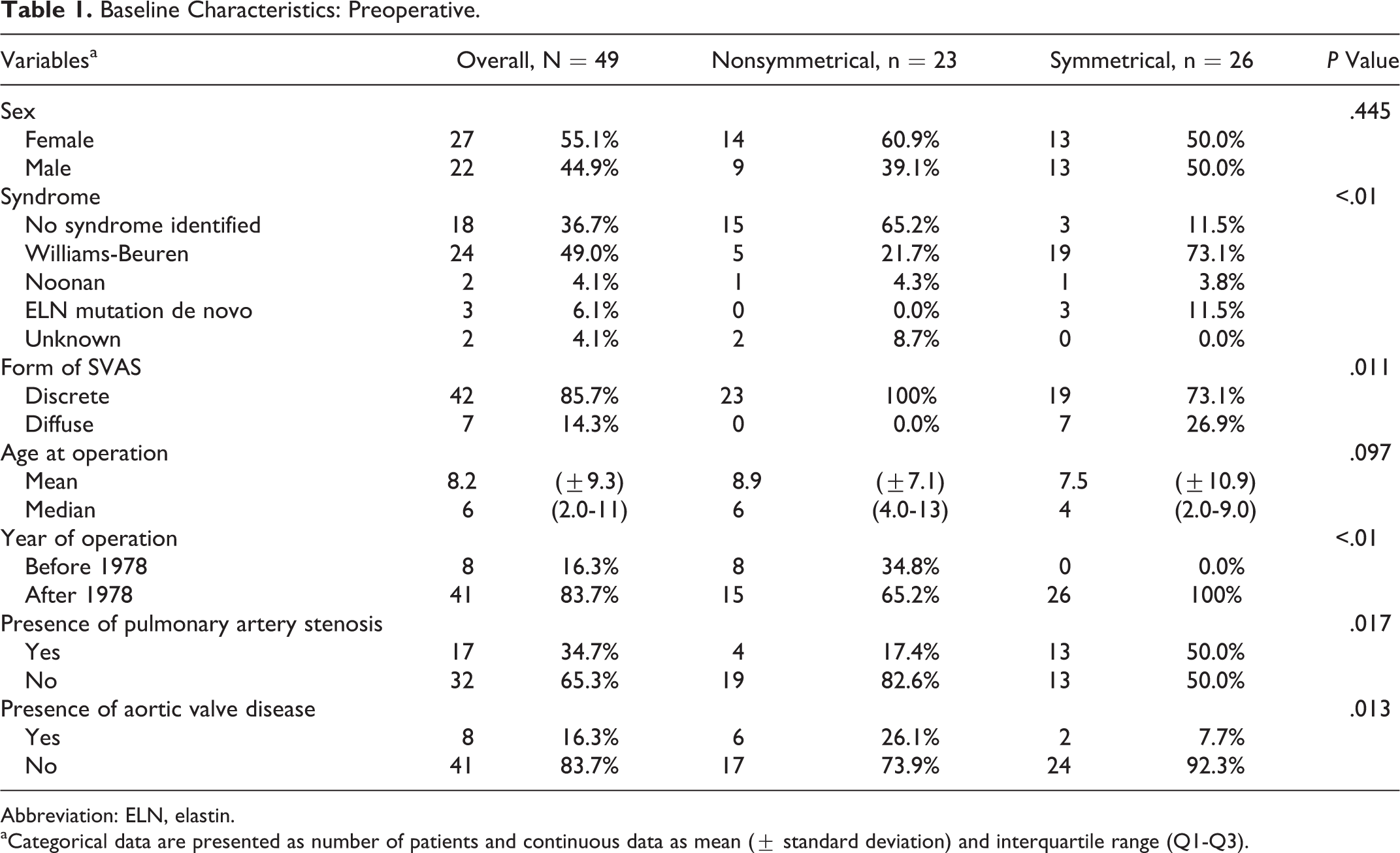
Abbreviation: ELN, elastin.
aCategorical data are presented as number of patients and continuous data as mean (± standard deviation) and interquartile range (Q1-Q3).
Concomitant Cardiovascular Anomalies.
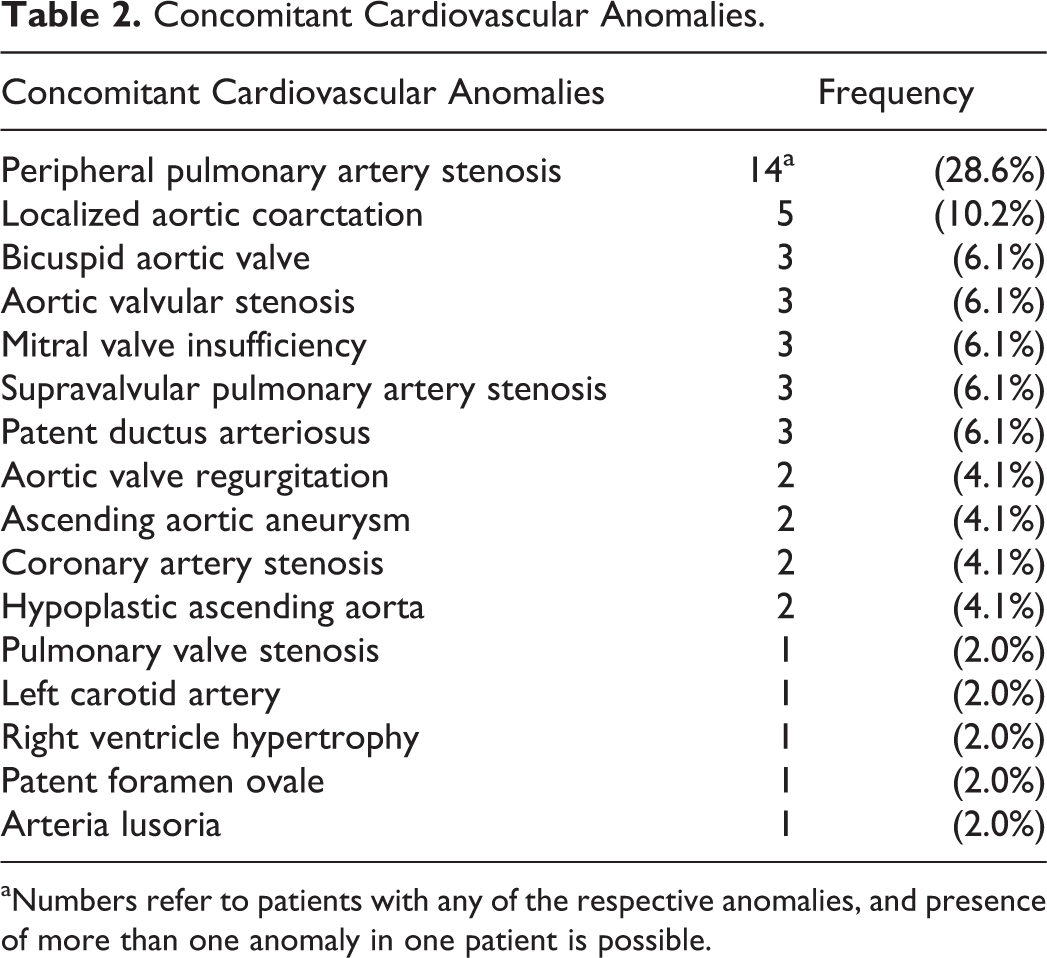
aNumbers refer to patients with any of the respective anomalies, and presence of more than one anomaly in one patient is possible.
We divided the patients in two groups: 23 (46.9%) patients were operated on using the nonsymmetrical techniques (22.4% using the single-patch technique and 24.5% using the two sinus augmentation) and 26 (53.1%) patients were operated using the symmetrical (three-patch) technique.
Mortality
Follow-up was 100% complete. The mean follow-up time was 19.2 years (SD: 12.8, median 19). The longest follow-up time was 52 years. A total of eight (16.3%) patients died, of which two were early deaths and six late deaths (Table 3). Of the six late deaths, four were out-of-hospital cardiac arrests, the age of dead patients varied between 33 and 57 years, and only one patient was diagnosed with Williams syndrome. The actuarial survival of all patients at ten years was 94% (standard error [SE]: 0.035), at 20 years 81% (SE: 0.067), at 30 years 81% (SE: 0.067), and at 40 years 68% (SE: 0.135). In the nonsymmetrical group, actuarial survival at 10 years was 96% (SE: 0.043), at 20 years was 80% (SE: 0.091), at 30 years was 80% (SE: 0.091), and at 40 years was 67% (SE: 0.143; Figure 2
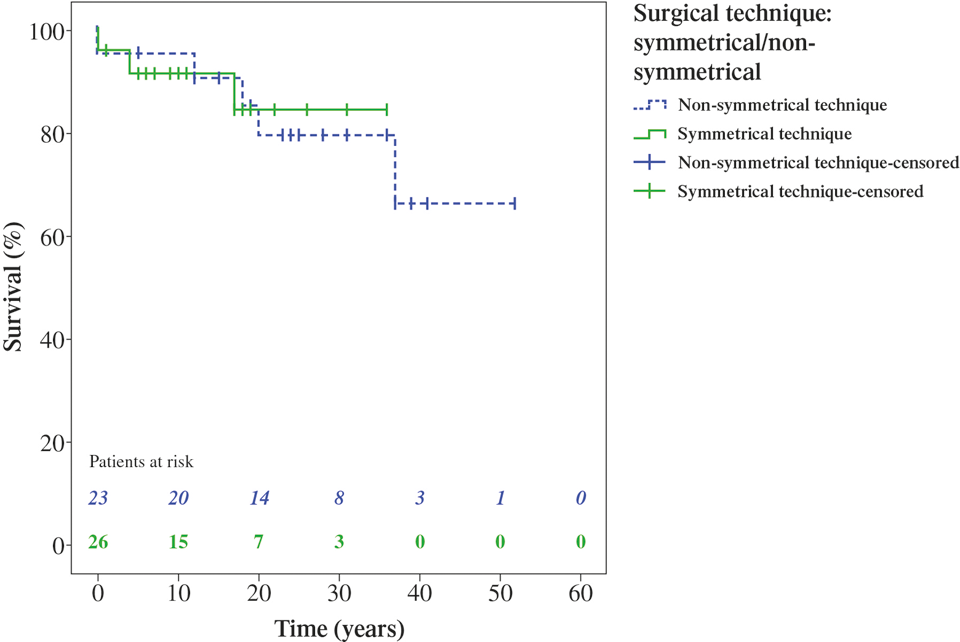
Kaplan-Meier survival curve. The numbers of patients belonging to the nonsymmetrical group are shown in blue, the numbers of patients in the symmetrical group are shown in green.
Details of Deceased Patients.
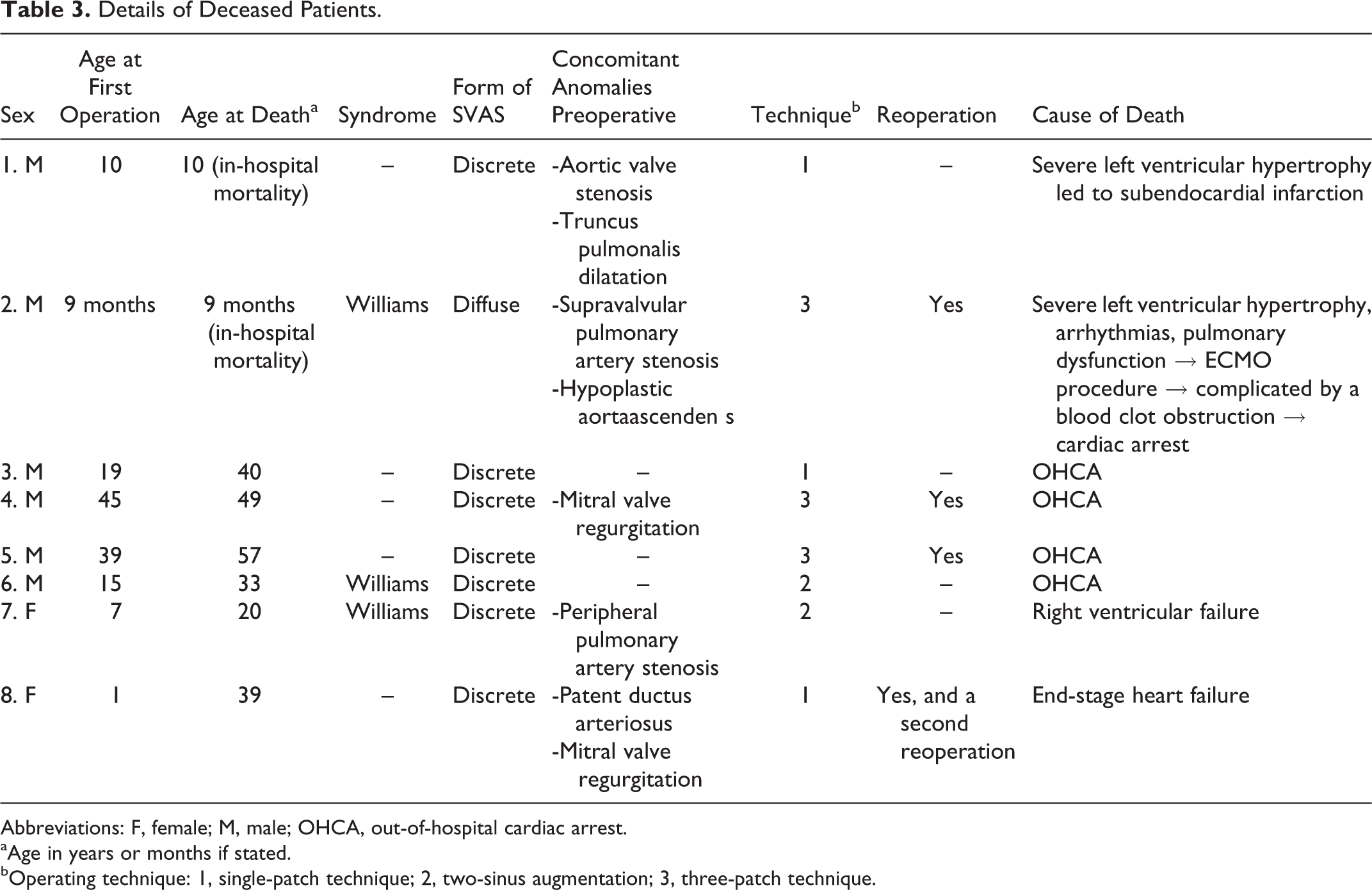
Abbreviations: F, female; M, male; OHCA, out-of-hospital cardiac arrest.
aAge in years or months if stated.
bOperating technique: 1, single-patch technique; 2, two-sinus augmentation; 3, three-patch technique.
Reoperation
A total of eight (16.3%) patients were reoperated, involving three early reoperations and five late reoperations (Table 4). All techniques combined, the total percentage of patients free from reoperation was 92% (SE: 0.040) after 10 years and 79% (SE: 0.067) after 20 years. In the nonsymmetrical group, freedom from reoperation after 10 years was 100% and after 20 years 88% (SE: 0.079). There were no reoperations performed on the patients at risk in the nonsymmetrical group more than 20 years after their initial operation (Figure 3). In the symmetrical group, freedom from reoperation after 10 years was 84% (SE: 0.072) and after 20 years was 71% (SE: 0 .107). The odds of freedom of reoperation were not significantly higher for patients in the nonsymmetrical group compared to the symmetrical group: adjusted odds ratio: 0.156, 95% CI: 0.004-5.773; P = .313. The Kaplan-Meier curve for freedom from reoperation (Figure 3) shows a marked lower curve for the symmetrical group, mainly due to more frequent early reoperations in the symmetrical group.
Details of Reoperated Patients.
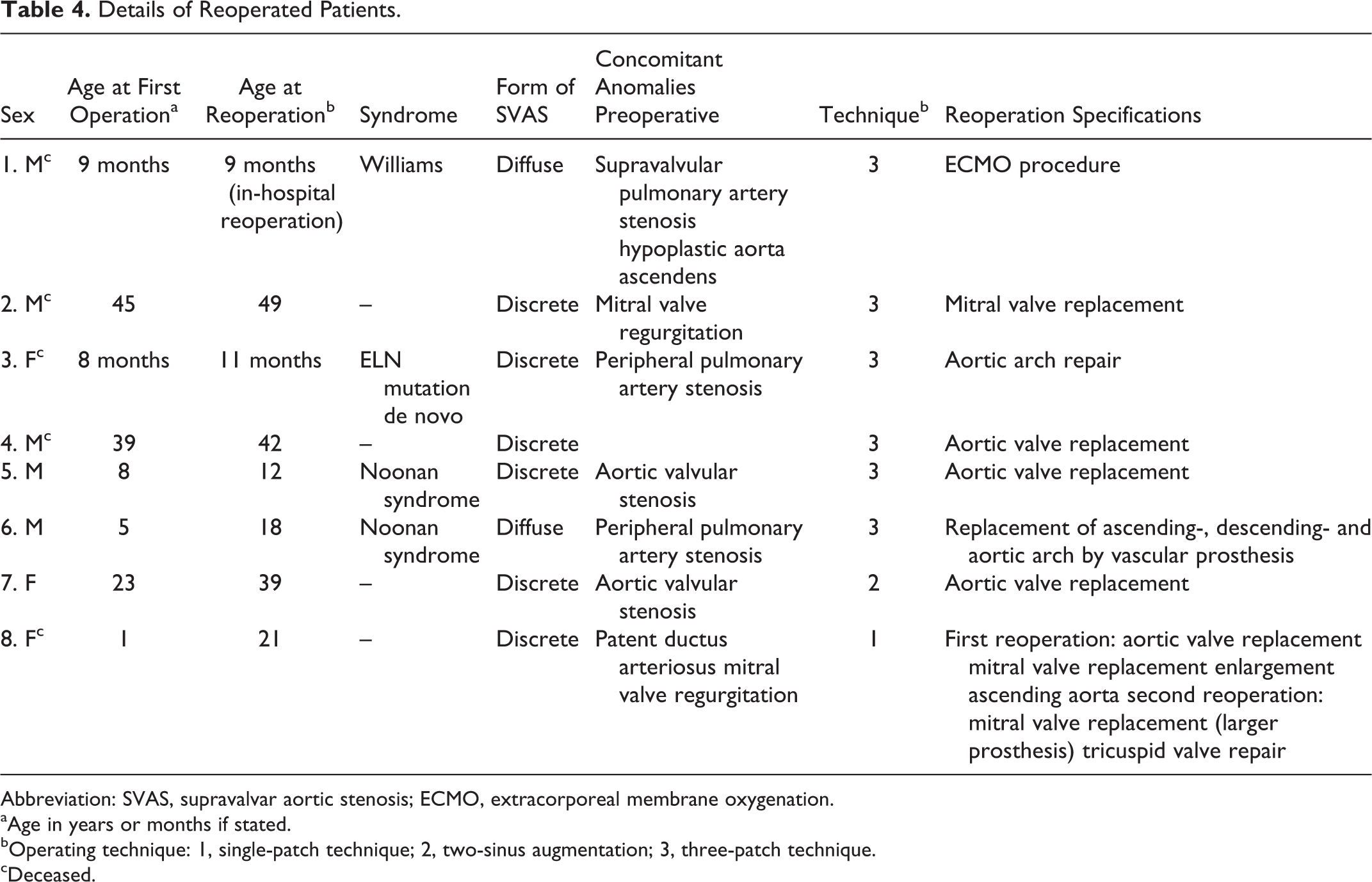
Abbreviation: SVAS, supravalvar aortic stenosis; ECMO, extracorporeal membrane oxygenation.
aAge in years or months if stated.
bOperating technique: 1, single-patch technique; 2, two-sinus augmentation; 3, three-patch technique.
cDeceased.
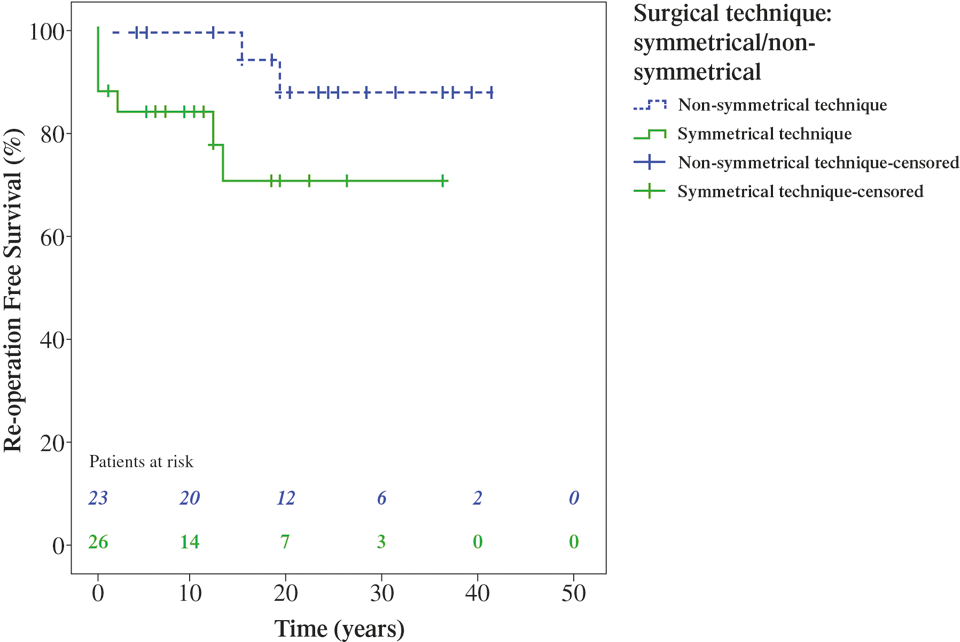
Kaplan-Meier reoperation-free survival. The numbers of patients belonging to the nonsymmetrical group are shown in blue, the numbers of patients in the symmetrical group are shown in green.
Echocardiography
The echocardiographic follow-up was incomplete due to the retrospective character of the study. Some patients did not visit their cardiologist regularly and some were followed up without echocardiographic imaging. Echocardiographic images that were suitable for analysis were available in 13 patients (26.5%), 9 of whom were operated with the nonsymmetrical technique and 4 with the symmetrical technique. None of the patients showed a significant restenosis of the supravalvular area (Figure 4).
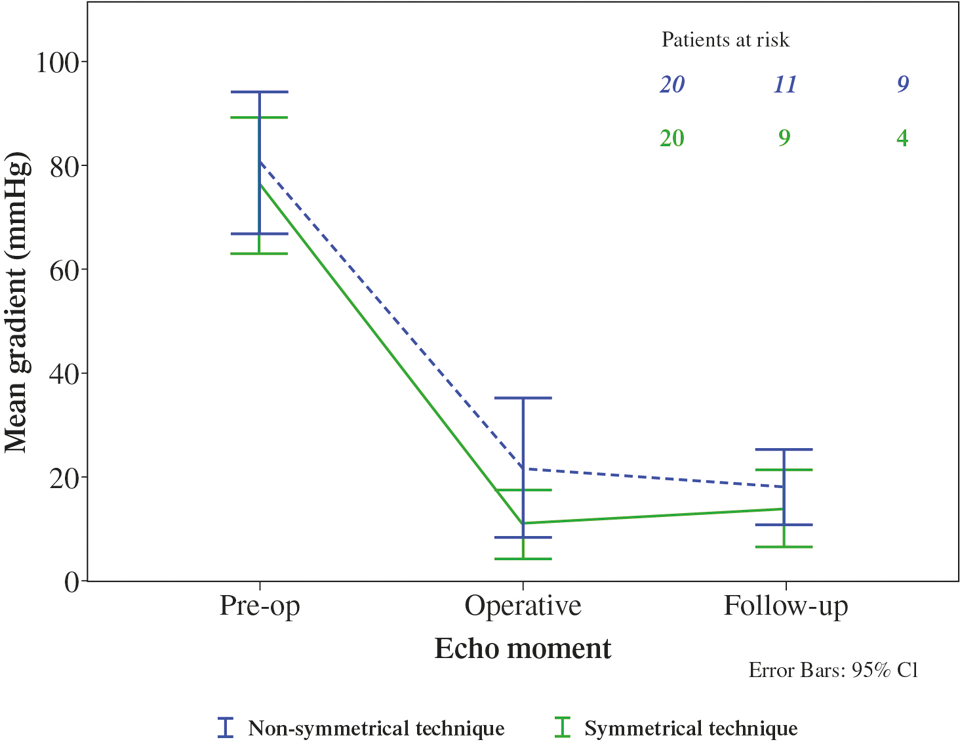
Echocardiographic gradients.
Discussion
This study did not show a significant difference in mortality and reoperation rates between an asymmetrical and symmetrical correction of SVAS. Interestingly, compared to the survival in the general population, the long-term survival of SVAS patients is remarkably low.
The most common reason for reoperation identified in the present study was aortic valve replacement, which was identified in previous studies as well. 7 –19 Enlarging the aortic root could theoretically lead to aortic regurgitation, because the aortic cusps might not be sufficient for the “new”aortic root geometry. A nonsymmetric repair would more likely cause an unbalanced aortic valve, causing regurgitation as well. Four patients needed aortic valve replacement. Two patients were operated with the symmetrical technique, one had aortic valve regurgitation and the other patient had aortic valve stenosis. Two patients were operated on with the nonsymmetrical technique, one had aortic valve regurgitation and the other patient had aortic valve stenosis. Other studies also did not find differences between the groups, mainly due to the small reoperation rates or short follow-up time. 3,4,9 –19 The results of the single-center study of Metton et al actually showed that at the last follow-up the lowest incidence of moderate aortic regurgitation was found in the three-patch technique group compared to the one- and two-patch technique groups. 17
Previous studies showed that the presence of diffuse SVAS is a possible predictor of early and late mortality. 20 In the present study, of the patients who died (n = 8), seven had discrete SVAS and one had diffuse SVAS. Because of the small incidence of diffuse SVAS (n = 7) in this study, no conclusions can be drawn concerning the form of SVAS as a predictor of mortality. Previous studies show low early mortality rates (1%-5%) and when follow-up time increases, both mortality rates and reoperation rates rise. These studies show ten-year survival rates of 84% and 95%, and 20-year survival rates of 70% and 90%. 9,10,12,16,21 Our study reports the longest follow-up. Our results show a rise of both mortality and reoperation rate after the first decade (10-year survival: 94%, 20-year survival: 81%, and 40-year survival of only 68%; 10 years of freedom from reoperation: 92% and 20 and 40 years of freedom from reoperation: 79%). The survival in 1962, 1988, and 2014 in these age groups was >99% among the general population in the Netherlands. 22 Thus, compared to the survival in the general population, the survival of SVAS patients in our study is remarkable low.
Four of the six late deaths were out-of-hospital cardiac arrests. These four patients died at an age between 33 and 57 years. No autopsies were conducted. All were operated on for discrete SVAS and one had Williams syndrome. They all were operated on at a relatively old age (>14), therefore, we could argue that the coronary arteries were exposed to a high pressure in the prestenotic area for a relatively long period of time, which might have caused endothelial damage leading to ischemic heart disease as a cause for their sudden cardiac arrest. In two of these late deaths, echocardiography was conducted, respectively, one and two years prior to death, showing no abnormalities. This remarkably high mortality rates considering the character of the surgery, of which a high percentage out-of-hospital cardiac arrests makes us plead for a closer (preferably lifelong) follow-up of patients after surgical correction of SVAS including exercise capacity and Holter monitoring.
Strength and Limitations
Even though this study has the longest follow-up time (52 years) ever reported in patients operated for SVAS with a mean length of follow-up of 19.2 years (SE: 1.8), and although this study includes patients from two of four congenital heart surgery centers in the Netherlands, the study population consisted of only 49 patients. Also the majority of the patients included have a follow-up of less than equal to ten years, the number of patients declines fast after this point, and therefore it is difficult to draw conclusions after this point. A strong feature of this study is that the different operating techniques are well divided over the population: nonsymmetrical techniques (46.9%) and symmetrical technique (53.1%). Most other studies show higher percentages for one particular technique. Nevertheless, in order to compare those two groups by means of a binary logistic regression analyses, a sample size of 49 patients is too small. As Long stated, sample sizes of <100 should be avoided in these analyses and a sample size of 500 or more should be adequate for almost any situation. 23 The rareness of this disease makes it very difficult to obtain a high number of patients in one country. 24 As all other studies that are conducted in this field so far, all have study populations of less than 100, the question rises what these conclusions really tell us. 3,4,9 –19 A meta-analysis would be an option. As shown in Table 1, the two groups are significantly different on various characteristics. We corrected for these differences and potential confounding factors by means of the propensity scores. Nevertheless, this will not provide total equalization of the groups. Unmeasured confounders will still be there, for example, the form of SVAS could not be matched using propensity scoring because the number of patients was too small. Nevertheless, all seven patients with the diffuse form of SVAS were in the symmetrical group. This might be considered an unmeasured confounding factor. Also all patients operated on before 1978 belonged to the nonsymmetrical group, and this group had a higher percentage of preoperative pulmonary artery stenosis. This cohort is too small to state that one confounder might influence the results more than another or might influence the results at all.
In our cohort, there were only three patients with SVAS and a bicuspid aortic valve, all three were operated on with a nonsymmetrical technique. Based on our present experience, we do not prefer a nonsymmetrical over a symmetrical reconstruction in patients with a bicsupid aortic valve. We would enlarge the sinuses with one or two patches depending on what looks best.
We took survival and reoperation as end points. In both groups, there were eight events. The small cohort and the relatively small number of events with the end point reoperation are limitations of this study. The lack of additional information regarding those deaths is another limitation, as is the less than optimal echocardiographic follow-up percentage (74%) for this cohort.
Conclusions
In this patient group, there was no significant difference in survival and freedom from reoperation between the different surgical techniques for SVAS repair. Compared to the survival in the general population, the survival of SVAS patients is remarkably low. Apparently, SVAS is not a benign disease and probably patients should be followed more closely for the rest of their lives.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.