
Abstract
Introduction:
Inotropes are frequently being used in children undergoing heart surgery to prevent or treat low cardiac output syndrome (LCOS). There is only limited evidence that inotropes actually positively influence postoperative outcome. Our aim was to describe the current international practice variation in the use of inotropes following congenital heart surgery.
Methods:
We developed an online survey regarding the postoperative use of inotropes. We sent an invitation to all 197 registered members of the Pediatric Cardiac Intensive Care Society (PCICS) to participate in the survey. We also performed a systematic review of the literature.
Results:
Ninety-eight people (50%) responded, representing 62 international centers. Milrinone is routinely used perioperatively by 90 respondents (97%). Adrenaline/epinephrine is routinely used by 43%, dopamine by 36%, dobutamine by 11%, and levosimendan by 6%. Steroids are used routinely by 54% before initiating cardiopulmonary bypass. Vasopressin is used by 44% of respondents. The development of LCOS is monitored with lactate in 99% of respondents, physical examination (98%), intermittent mixed venous saturation (76%), continuous mixed venous saturation (13%), echocardiography (53%), core–peripheral temperature gap (29%), near-infrared spectrometry (25%), and 4% use cardiac output monitors (PiCCO, USCOM). To improve cardiac output, 42% add/increase milrinone, 37% add adrenaline, and 15% add dopamine. Rescue therapy is titrated individually, based on the patients’ pathophysiology. A systematic review of the literature failed to show compelling evidence with regard to the benefit of inotropes.
Conclusions:
Despite the lack of sufficient evidence, milrinone is used by the vast majority of caregivers following congenital heart surgery.
Keywords
Introduction
Inotropes are frequently being used in children undergoing heart surgery to prevent or treat low cardiac output syndrome (LCOS) that typically occurs 6 to 18 hours after cardiopulmonary bypass (CPB) surgery. 1 There is ample evidence describing how certain inotropes affect the hemodynamics in adults and children undergoing heart surgery. But there is only limited evidence that certain inotropes actually positively influence postoperative outcome. 2 A recent Cochrane review concluded there is insufficient evidence of effectiveness of prophylactic milrinone in preventing death or LCOS in children undergoing surgery for congenital heart disease, compared to placebo. 3 There is no evidence in the literature in favor of one inotrope over another in improving postoperative outcomes. The aim of this study was to describe current international practice variation regarding the use of inotropes in children undergoing heart surgery.
Methods
Survey
In May 2014, we developed an online survey for the members of the Pediatric Cardiac Intensive Care Society (PCICS), with questions regarding the prevention and treatment of LCOS in pediatric patients after cardiac surgery.
The questionnaire consisted of 22 questions covering different aspects of postoperative management in children who underwent cardiac surgery. Most of the questions concerned the treatment and prevention of LCOS in children while other questions where about postoperative temperature control. The management of hypertension in patients who underwent surgery for coarctation of the aortae was part of the same survey and published separately. 4 Most questions could be answered with multiple answers. Respondents were free not to answer a question if they chose not to do so, therefore not all questions were answered by all 98 respondents.
Survey Participants
We sent an invitation to partake in the survey to all 197 registered PCICS members at the time. In the accompanying letter it was mentioned that all responses would be analyzed anonymously and that it was the intention to publish the results. A reminder was sent after two and four weeks if they had not yet responded. Data were collected between May and June 2014.
Data Analysis
The results are descriptive and were expressed as percentages. No comparative statistical tests were performed.
Literature Review
The authors searched PubMed for all known inotropes and cross-referenced them with key words such as “pediatric,” “child,” “neonate,” “newborn,” “cardiac,” “heart,” “congenital,” and “surgery.” The authors also scanned all references in the found articles and then read all titles and abstracts of relevant studies. Then randomized controlled trials were selected in which inotropes were compared with each other or with placebo in pediatric or congenital cardiac surgery, or animal models of congenital heart surgery.
Results
Survey Participants
Ninety-eight people (50%) responded from 62 different medical centers across the world (center distribution: 61% United States, 15% Europe, 8% Canada, 6% Asia, 3% Australia, 3% South America, and 2% Africa; see Table 1). Fifty-six (73%) respondents were pediatric intensive care unit (PICU) consultants, 27 (35%) pediatric cardiologists, 23 (23%) nurse practitioners, 3 (3%) cardiothoracic surgeons (3%), 5 (5%) anesthesiologists, and 4 (4%) PICU trainees. Several medical respondents were dually certified (PICU and cardiology). Most respondents (63%) worked in centers with more than 300 pediatric heart surgeries per year.
Demographics of the Respondents: Origin, Specialization, and Number of Operations Performed at Their Center per Annum.a,b,c
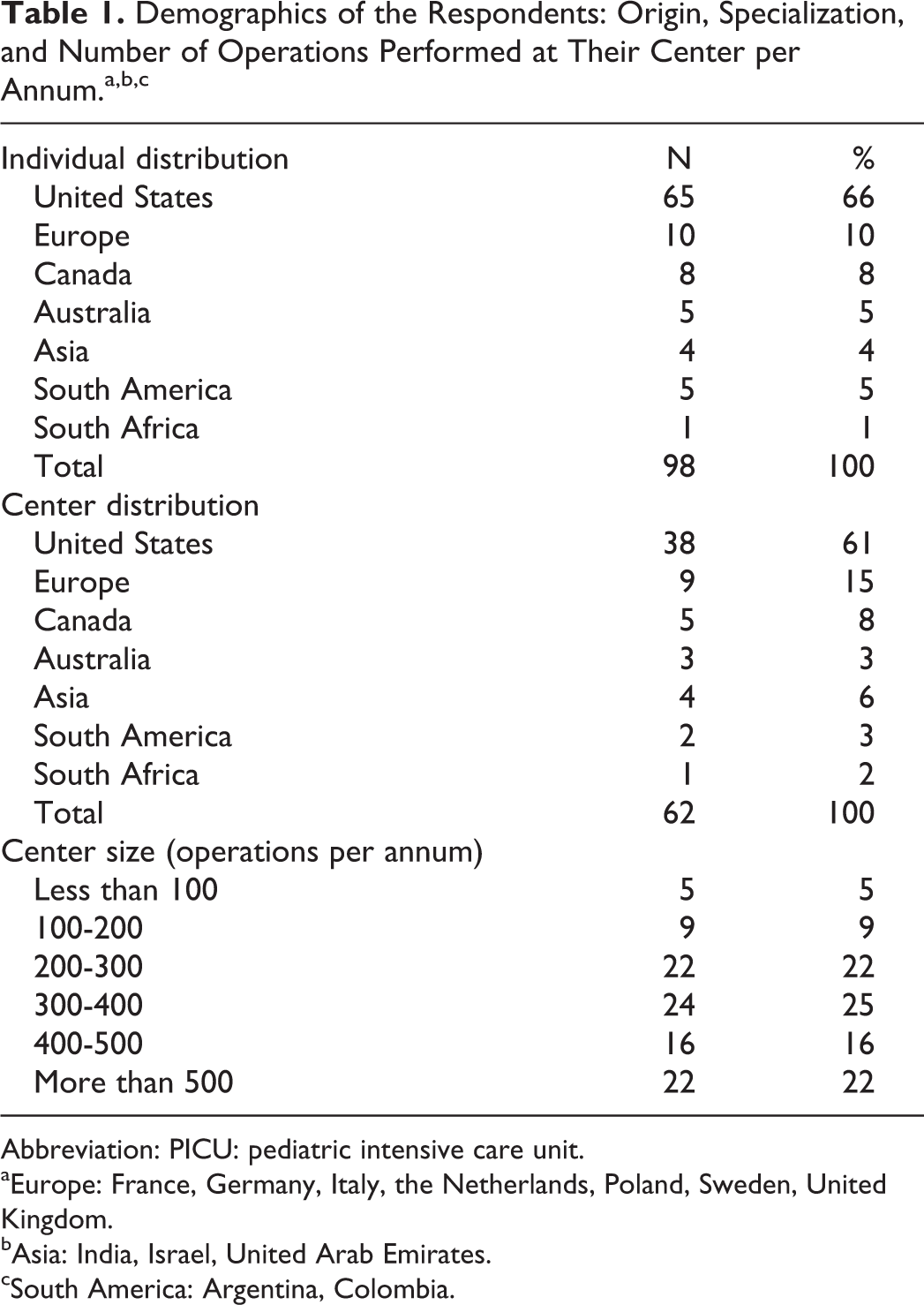
Abbreviation: PICU: pediatric intensive care unit.
aEurope: France, Germany, Italy, the Netherlands, Poland, Sweden, United Kingdom.
bAsia: India, Israel, United Arab Emirates.
cSouth America: Argentina, Colombia.
Drug Choice for the Prevention of LCOS
Ninety-three (95%) of all 98 respondents answered this question. The prevention of LCOS is characterized by considerable variability (see Table 2). Eight different drugs used for the prevention of LCOS. Most respondents use milrinone (97%) routinely for the prevention of LCOS. Other frequently used drugs for the prevention of LCOS are adrenaline (45%) and dopamine (38%). Dobutamine is used by 11% and levosimendan by 5% of respondents.
Reports of Drugs Regimen for Prevention of LCOS and Timing of Administration.a
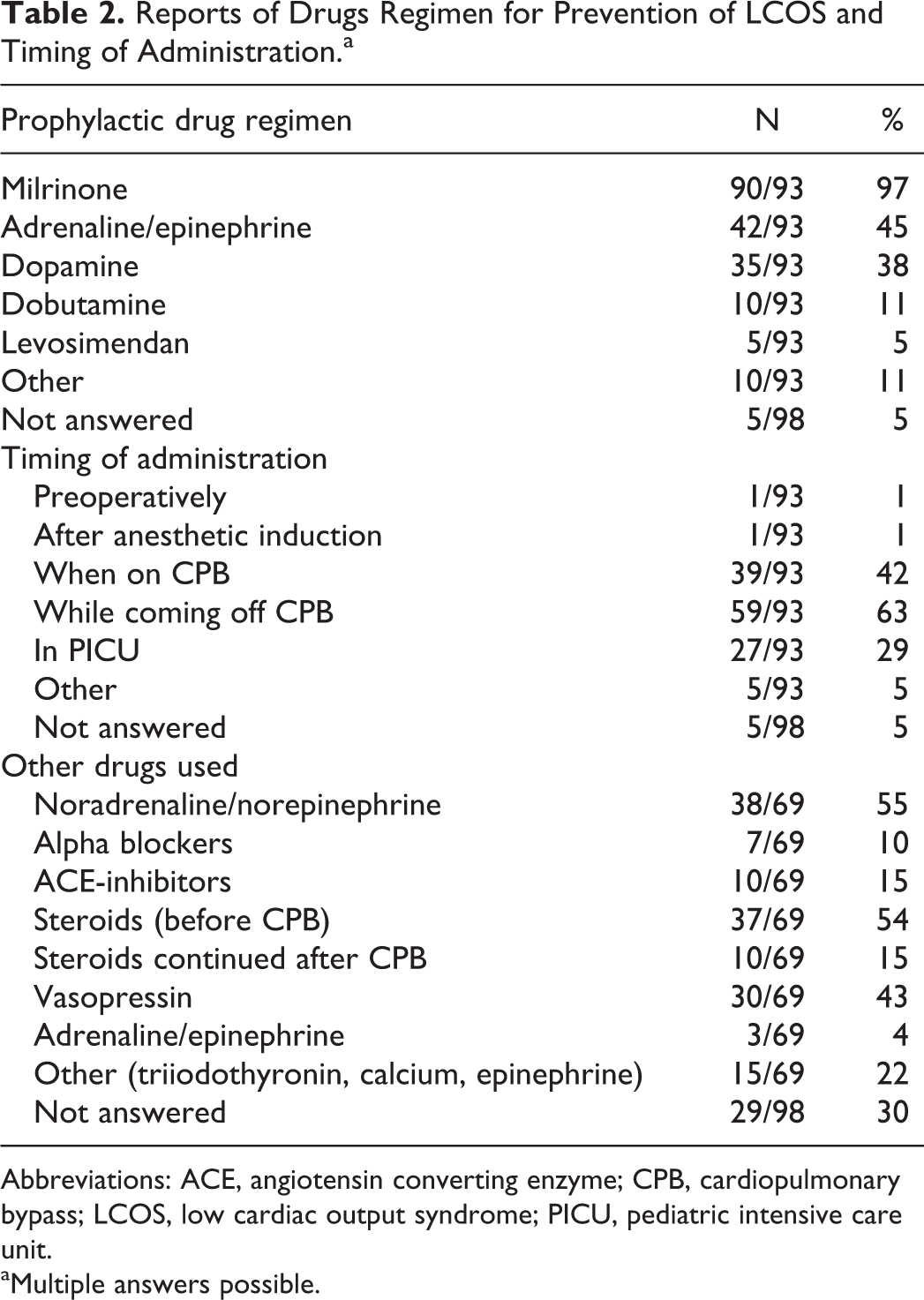
Abbreviations: ACE, angiotensin converting enzyme; CPB, cardiopulmonary bypass; LCOS, low cardiac output syndrome; PICU, pediatric intensive care unit.
aMultiple answers possible.
There is marked variability in the timing of initiating prophylactic inotropes. Respondents could give multiple answers as individual clinical indication might necessitate different timing. Forty-two percent start the inotrope at the start of CPB, 63% indicate starting while coming off CPB, and 29% started inotropes when the patient arrives in the ICU.
Sixty-nine respondents (70%) indicated that they routinely use other pharmacological agents besides their main inotrope. Other medications that are frequently used concomitantly are noradrenaline/norepinephrine (55%), steroids (54%), and vasopressin (43%). Thirty percent of respondents indicate that they give noradrenaline/norepinephrine routinely to maintain blood pressure while giving milrinone. Vasodilators such as angiotensin-converting-enzyme (ACE) inhibitors and alpha-agonists are routinely used by 10 (15%) of 69 and 7 (10%) of 69, respectively. Adrenaline/epinephrine is routinely used by 3 (4%) of 69 of respondents.
Out of 69 who answered this question, 57 (83%) respondents specifically indicated that the use of these second-tier medications is based on clinical requirements. The strategies used vary from the use of vasopressors in vasodilated states to improve perfusion pressures, to vasodilators in order to promote afterload reduction and cardiac output.
When steroids are used, they are mostly given before going on CPB (54%) and in 15% it is routinely continued after the bypass.
Monitoring Cardiac Output
Ninety-one respondents indicated the use of different methods to monitor cardiac output postoperatively (see Table 3). Lactate (99%), physical examination (98%), and intermittent or continuous venous saturation (89%) are mostly used for monitoring cardiac output. Echocardiography is used by 53% of the respondents, core–peripheral temperature gap by 32%, and near-infrared spectrometry (NIRS) is used by 26%. The use of minimally invasive cardiac output monitoring (e.g. pulse index continuous cardiac output [PICCO, Pulsion, Germany] or Doppler hemodynamic cardiac output monitoring [USCOM Ltd, Australia] is limited (3%).
Monitoring of Development of LCOS. Multiple Answers Possible. NIRS: Near-infrared Spectrometry.
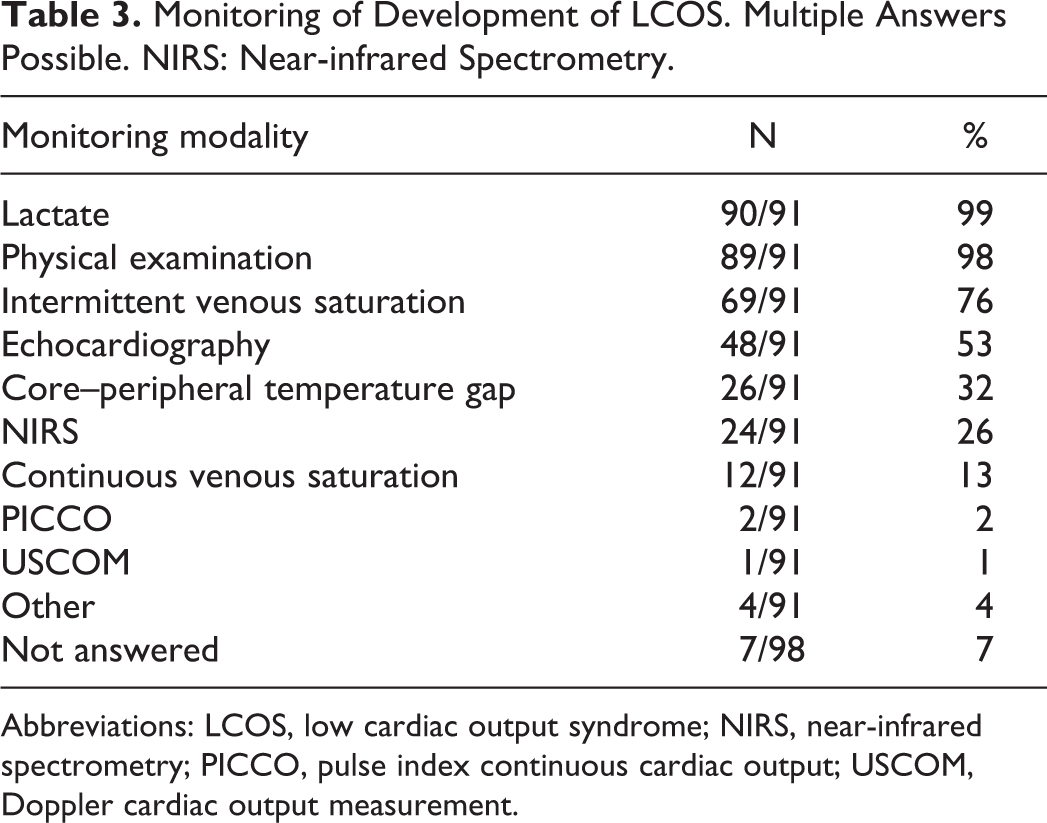
Abbreviations: LCOS, low cardiac output syndrome; NIRS, near-infrared spectrometry; PICCO, pulse index continuous cardiac output; USCOM, Doppler cardiac output measurement.
Drug Choice for Improving Cardiac Output
Most respondents indicate that their choice of drugs for improving cardiac output is based on the pathophysiology of the underlying condition, the severity of the LCOS, and the medication that is already being administered. Eighty-five respondents (85/98 = 87%) answered this question and indicated increasing either milrinone (42%) or adrenaline/epinephrine (36%) when cardiac output is worsening (see Table 4). If this treatment fails, then in most of the cases adrenaline/epinephrine (40%) will be added as the second drug of choice. Under “other” 17% indicated that clinical circumstances directed their specific therapies. Extracorporeal membrane oxygenation (ECMO) was also given as an option several times but was not specified by many other respondents. The timing of initiating ECMO postcardiotomy remains challenging. It was not a part of this survey.
Reports of Drugs Regimen for Treatment of LCOS.a

Abbreviations: ECMO, extracorporeal membrane oxygenation; LCOS, low cardiac output syndrome.
aOne answer only.
Managing Cardiac Output in a Mixed Circulation
Eighty-nine respondents (91%) answered questions regarding specific management in mixed circulations (see Table 5). In a mixed circulation, the majority will try to decrease the systemic vascular resistance (SVR) to promote systemic circulation (79%). Forty-two percent will try to increase pulmonary vascular resistance (PVR) to promote systemic cardiac output. A combination of both is indicated by 17%, which is probably an underestimation because we did not specifically ask how many used a combination.
Strategy in Patients With Mixed Circulation.a
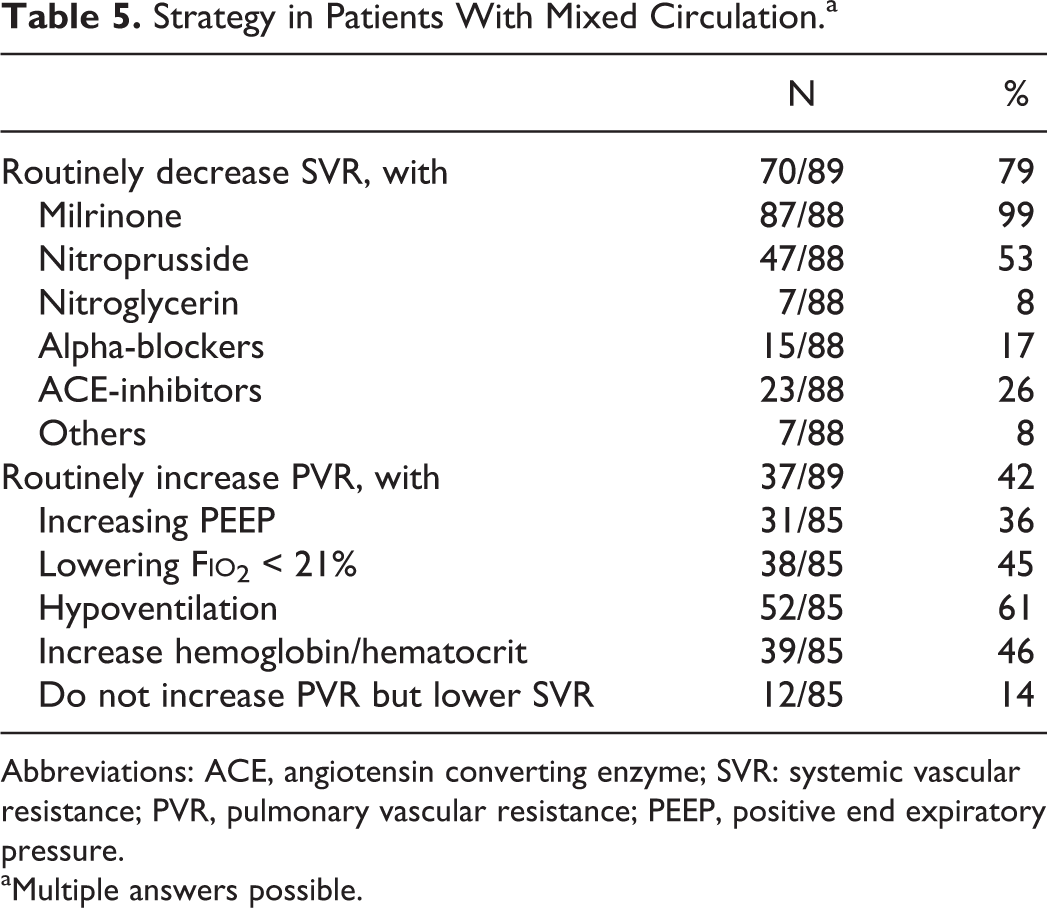
Abbreviations: ACE, angiotensin converting enzyme; SVR: systemic vascular resistance; PVR, pulmonary vascular resistance; PEEP, positive end expiratory pressure.
aMultiple answers possible.
To achieve an increase in PVR, respondents will try to achieve hypoventilation (61%), increase hemoglobin (46%), lower inhaled oxygen concentration below 21% (45%), and/or increase positive end expiratory pressure (36%). All 85 respondents of this question indicate the use of a combination of these nonpharmacological strategies.
Eighty-eight respondents answered the question regarding decreasing SVR. Almost all (87/88) aim to lower SVR by using milrinone (99%) followed by nitroprusside (53%), ACE-inhibitors (26%), alpha-blockers (17%), nitroglycerin (8%), or others like nicardipine or phenoxybenzamine (8%).
Temperature Regulation in PICU
Eighty-seven (89%) and 81 (83%) of 98 respondents answered the questions about temperature management post CPB and post deep hypothermic circulatory arrest (DHCA) respectively (see Table 6). Postoperative hyperthermia is prevented routinely in PICU in the majority of the respondents following CPB (52%) with or without DHCA (48%). Only about 8% will routinely try to achieve mild hypothermia (35°C-36°C or 95°F-97°F). Nine respondents (10%) indicate that hypothermia will be used in patients for heart rate control (eg, in case of junctional ectopic tachycardia).
Temperature Management Following Pediatric Heart Surgery.
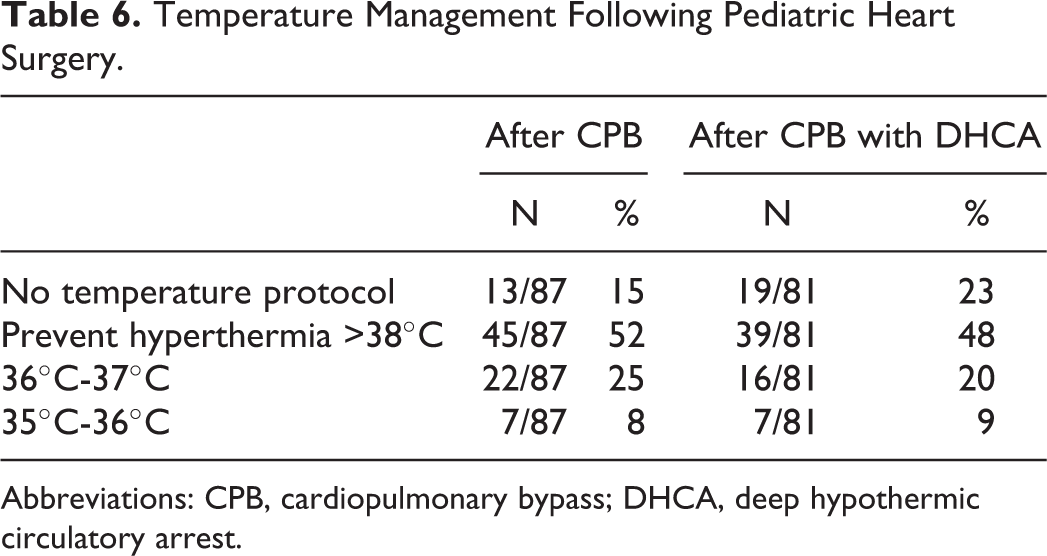
Abbreviations: CPB, cardiopulmonary bypass; DHCA, deep hypothermic circulatory arrest.
Systematic Review of the Literature
We identified 20 randomized controlled trials comparing inotropes in (animal models of) congenital pediatric heart surgery. Table 7 gives a clear overview of these studies, including design, subjects, the presented results, and the effects on clinically relevant outcomes such as mortality, duration of mechanical ventilation (MV), and length of stay (LOS). Of those 20 studies, 2 were crossover studies reporting on hemodynamic variables 5,7 and 2 were animal studies. 11,12 Of the remaining 16 studies in children, 6 studies reported on mortality. 2,14,17,18,20,21 In none of these studies, mortality was positively (or negatively) influenced by the studied inotrope. Duration of MV or LOS (PICU and/or hospital) was reported by 10 of the 16 studies. 2,13,14,16 –18,20 –23 Only in one report the duration of MV was positively influenced, by a combination of milrinone and inhaled nitric oxide (iNO) in children following the Fontan operation. 21 In the other nine studies, no positive effect of inotropes was found on important outcome measures such as duration of MV and LOS.
All Published Randomized Controlled Trials of Inotropes in (Models of) Pediatric Cardiac Surgery.a
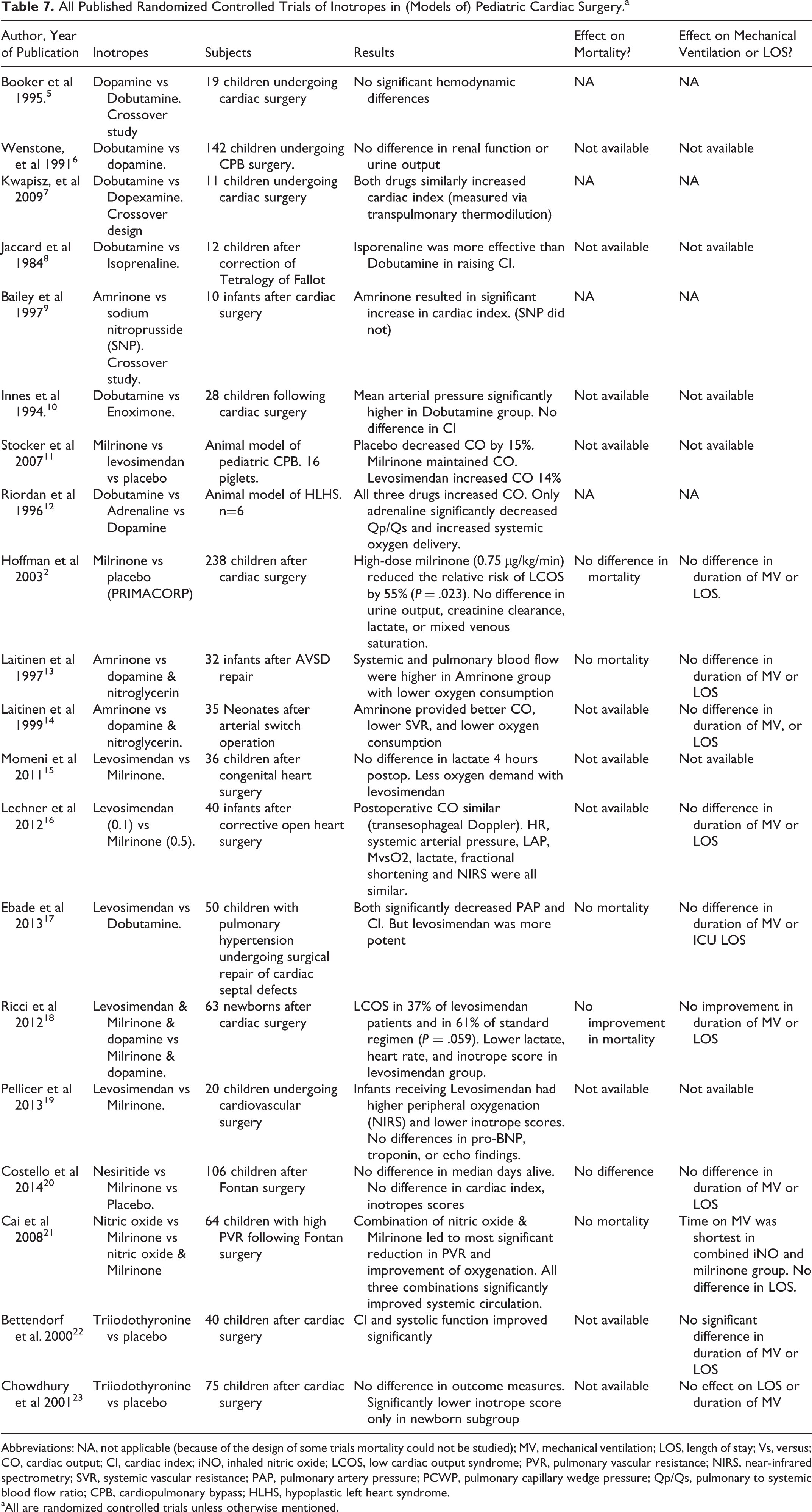
Abbreviations: NA, not applicable (because of the design of some trials mortality could not be studied); MV, mechanical ventilation; LOS, length of stay; Vs, versus; CO, cardiac output; CI, cardiac index; iNO, inhaled nitric oxide; LCOS, low cardiac output syndrome; PVR, pulmonary vascular resistance; NIRS, near-infrared spectrometry; SVR, systemic vascular resistance; PAP, pulmonary artery pressure; PCWP, pulmonary capillary wedge pressure; Qp/Qs, pulmonary to systemic blood flow ratio; CPB, cardiopulmonary bypass; HLHS, hypoplastic left heart syndrome.
aAll are randomized controlled trials unless otherwise mentioned.
Discussion
This is the first international survey of the use of inotropes and intensive care management after pediatric cardiac surgery. There have been one Italian and one European survey concerning pediatric LCOS. 24 –26
Prevention of Low Cardiac Output Syndrome
The results of this survey show that, worldwide, milrinone is being used by 97% of respondents for the prevention of LCOS in children (Table 2). The other drugs used are adrenaline/epinephrine (45%), dopamine (38%), dobutamine (11%), and/or levosimendan (5%). These results include the use of multiple drugs. This diversity in pharmacological approaches reflects the current lack of sufficient guiding evidence in the literature. 3
In 2011, a European survey also reported a marked variability with milrinone as the most used inotrope (71%) in pediatric cardiac surgery patients which is significantly fewer than 97% in our survey. 24 In their survey, dopamine (19%) and adrenaline (16%) were used much less frequently than in our survey (45% and 38%, respectively). A recent single-country survey reported that a combination of dopamine and milrinone was the most frequent drug regimen for prevention of LCOS after congenital heart surgery in Italy. 26 This difference in the use of inotropes could reflect differences in European and American approach to the use of inotropes as most of our respondents were North American or Canadian. Due to the design of our study and the survey engine used, it was not possible to do a subanalysis and compare continents.
Improving Cardiac Output
To improve postoperative cardiac output, there is more diversity in inotrope use, whereby milrinone, adrenaline/epinephrine, dopamine, and dobutamine are mostly used (Table 4). In the European and Italian surveys, milrinone was most often used for the treatment of LCOS with elevated SVR or elevated PVR. 25,26 In the European study, dobutamine is preferred for the treatment of LCOS with low SVR, but adrenaline/epinephrine or dopamine were first and second choice in the Italian survey. In this current survey, the authors did not specify the different kinds of LCOS (high SVR, low SVR).
Thus, in this and other surveys, multiple drugs are used for the prevention and treatment of LCOS in pediatric patients after cardiac surgery. But there seems to be a clear preference for milrinone despite the lack of compelling evidence for its benefit over other drug regimens. 3
The Ideal Inotrope
The ideal inotrope would consistently improve systolic and diastolic cardiac function, decrease afterload, improve cardiac output, have a favorable effect on myocardial oxygen hemodynamics, and improve survival and quality of life, with as little adverse effects and interactions as possible. Furthermore, ideally, different specific inotropes would have proven effects and benefits for specific disease states. Unfortunately, the ideal inotrope does not exist. But the (cardiac) intensivist does have a number of pharmacological options at his or her disposal with well-known hemodynamic effects. 27
Milrinone
Multiple studies in adults, and children, have shown the positive hemodynamic effects in response to milrinone, an effect not seen in preterm infants. 28 –34 Milrinone is a phosphodiesterase inhibitor and improves contractility by inhibiting the breakdown of cyclic adenosine monophosphate (cAMP). 29 Other effects are afterload reduction and improved diastolic function (lusotropy) with minimal increase in myocardial oxygen consumption. Together these effects lead to an increased cardiac index and decrease in the mean arterial blood pressure (MAP). Milrinone has a relatively long half-life of 2 to 4 hours. 35,36 Stocker et al showed that milrinone can maintain normal cardiac output in an animal model of congenital heart surgery. 11
Milrinone in the pediatric population was first described in 1995 by Chang et al in ten neonates following cardiac surgery. 37 The authors, using a thermodilution pulmonary artery catheter (Baxter Edwards Critical-Care, Irvine, CA), measured an increase in cardiac index from 2.1 (± 0.5) to 3.0 (± 0.8) L/m2/min with the use of 0.5 μg/kg/min milrinone and 3 to 7 μg/kg/min dopamine, without increased myocardial oxygen consumption. This was not a controlled trial and they did not comment on clinical outcomes. Then in 1998, a pharmacokinetic study in 19 infants and children reported therapeutic plasma levels with both 0.5 and 0.75 μg/kg/min milrinone with reduced clearance compared to adults, especially in infants. 38 They also did not report on clinical outcomes.
In the landmark Primacorp study, by Hoffman et al, a high-dose milrinone (0.75 μg/kg/min) led to a significant reduction in surrogate markers of low cardiac output by 55% in children after biventricular repair. 2 However, there was no difference in lactate, duration of MV, hospital LOS, or mortality. Low-dose milrinone (0.25 μg/kg/min) showed no benefit compared to placebo. Unfortunately the dose of milrinone used was not addressed in the current survey. It might be that underdosing of milirinone can explain the lack of positive effects on clinically relevant outcomes. 39
A pharmacological study in 2013 showed that a median dose of milrinone of 0.5 μg/kg/min led to either sub- or supratherapeutic levels (<100 and >300 ng/mL, respectively) in 52% of the patients. 40 The authors report that there is an association between LCOS (defined as lactate > 2 mmol/L) and supratherapeutic milrinone blood levels, there was no association between subtherapeutic blood levels and LCOS. There was a higher incidence of arrhythmias with milrinone levels >200 ng/mL, but otherwise no correlation was found between blood levels and clinical outcomes such as hypotension, tachycardia, or lactate. However, milrinone dosing was not protocolized and given at the discretion of the treating physician, which may have confounded the results. The authors report an important suboptimal use of milrinone but do not comment on clinical outcome measures such as duration of MV, hospital LOS, and/or mortality. 40
A pharmacokinetic drug-disease model, reported by Vogt et al, also suggests that the current dosage for prevention as well as for treatment of LCOS might not be sufficient and suggests dosing should be age stratified. 39 Another pharmacological study conversely suggested the use of lower dose milrinone (0.2 μg/kg/min) because of drug accumulation post CPB surgery in children. 41 The effects of these age-related doses on the cardiac output and clinical outcomes remain to be investigated.
The only study in which milrinone improved an important clinical outcome was reported by Cai et al who showed that in 46 children following Fontan-type surgery, combined use of iNO and milrinone (0.5 μg/kg/min) did significantly reduce the duration of MV. 21 Length of hospital stay, however, was not affected.
In adults there have been concerns of chronic use of milrinone increasing mortality. 42,43 However, a more recent meta-analysis of 20 randomized trials showed no increased mortality due to milrinone in adult patients undergoing cardiac surgery. 44 But the higher-quality trials did suggest a trend toward increased mortality with milrinone. Although pediatric studies were included, no pediatric subanalysis was performed. Adults with chronic heart failure are very different than young children with congenital heart defects following surgery, but unlimited use of milrinone might not be without harm.
Therefore, we can conclude from the literature that there is insufficient evidence that milrinone improves clinical outcomes post pediatric heart surgery, a finding confirmed by a recent Cochrane review. 3
However, despite this lack of evidence, the positive hemodynamic effects of milrinone do lead to a widespread use as shown in our and other surveys. 24 –26 One of the hemodynamic effects is vasodilation with afterload reduction leading to improved cardiac output, however, there is also a high concomitant use of vasopressors as 55% report the use of noradrenaline and 43% use vasopressin to treat low SVR and blood pressure in our survey. Therefore, we must ask ourselves how much of the beneficial effect of milrinone is being counteracted by the use of vasopressors. This may be a reason why no study has yet been able to report a positive effect on clinical outcomes.
Adrenaline/Epinephrine
Epinephrine or adrenaline, is an endogenous catecholamine with dose-dependent effects. At lower doses (0.05-0.1 μg/kg/min), it stimulates the beta-adrenergic receptors leading to increased contractility, increased heart rate, and afterload reduction through peripheral vasodilation. 45,46 At higher doses (>0.1 μg/kg/min), it also stimulates alpha-adrenergic receptors leading to vasoconstriction. The stimulation of the beta-receptors leads to an increased calcium influx into the myocardial cell and increased cAMP, at the cost of increased oxygen consumption. In 1979, Benzing et al reported that the cardiac index in 13 children after cardiac surgery increased significantly when epinephrine was added to sodium nitroprusside, without a significant change in systemic resistance. 47
In animal models of single ventricle physiology, adrenaline increased cardiac output, systemic perfusion, and systemic oxygen delivery. 12,48 Despite the fact that there are no randomized controlled trials with adrenaline in pediatric heart surgery, 45% and 40% of respondents use adrenaline for prevention and treatment of LCOS, respectively, in this survey.
Dobutamine
Dobutamine is a synthetic catecholamine, with a short half-life of two minutes, which asserts its effect through beta receptors, stimulating a calcium influx and increase in cAMP. It has positive inotropic and chronotropic effects with peripheral systemic vasodilatation and no pulmonary vasodilatation. 8,49 –52 Important side effects are arrhythmias and increased myocardial oxygen consumption. Several adult and pediatric studies have found that dobutamine led to an increase in cardiac index in patients who underwent cardiac surgery, due to an increase in heart rate without an increase in stroke volume. 8,34,49 Myocardial oxygen uptake and coronary blood flow is increased with dobutamine. 53 In an animal model, Ferrara has found that dobutamine at higher dosage produced an increase in cardiac output only in term animals compared to preterm animals, with a significant increase in mean systemic arterial blood pressure. 54 When compared to enoximone, dobutamine also increased the MAP, but there was no difference in cardiac output in a study of 28 children following heart surgery. 10 The authors did not comment on mortality, duration of MV, or LOS. There is, to our knowledge, no literature on the effect of dobutamine on clinically relevant outcomes in children after heart surgery despite its well-known hemodynamic effects. Dobutamine to prevent LCOS is used routinely by 11% in this survey.
Dopamine
Dopamine also has dose-dependent actions but with relatively unpredictable dose response. 5,55 In low doses (<5 μg/kg/min) dopamine acts on dopaminergic receptors inducing natriuresis, diuresis, and increased mesenteric flow. 54,56 In medium dose (5-15 μg/kg/min) dopamine stimulates beta1-adrenergic receptors increasing cardiac output through chronotropy (mild effect), inotropy, and afterload reduction and increases glomerular filtration rate (GFR) and urine output through via dopaminergic receptors. 57 At high doses (>15 μg/kg/min) peripheral resistance increased via alpha-receptors leading to an increased MAP. Side effects are increased myocardial oxygen consumption, arrhythmias, hypothyroidism, and impaired T-lymphocyte proliferation. 55,58,59 In one adult study comparing dobutamine with dopamine, both drugs increased myocardial oxygen uptake but dopamine seemed to cause coronary constriction. 53 In children, an increase in pulmonary artery pressure (PAP) and PVR is seen with dopamine in a dose higher than 7.5 μg/kg/min. 5 Dopamine also causes an increase in cerebral, cardiac, and intestinal blood flow in term and preterm animals, which is dose dependent. 54 Dopamine has not been proven useful in the prevention or alteration of the course of acute renal failure. 60 When compared to dobutamine, there was no difference in renal function or urine output in 142 children after heart surgery. 6 Again, to our knowledge, there is no literature on the effect of dopamine on clinically relevant outcomes in children after heart surgery. However, because of its hemodynamic effects, it is used to prevent LCOS by 38% of respondents in this survey.
Other drugs and strategies
Levosimendan, a calcium-sensitizer, is a relatively new inotrope and one of the most studied. 61 –64 Levosimendan has a half-life of 1 hour (in adults) and is metabolized into an active metabolite, OR-1896, with a much longer half-life of 75 to 80 hours. 65,66 Both levosimendan and OR-1896 improve myocardial contractility by making troponin C more sensitive to the available intracellular calcium during systole, without affecting diastolic function. 67 It does not cause chronotropy and does not increase myocardial oxygen demand. 68,69 By stimulating potassium channels in vascular smooth muscle cells, levosimendan causes peripheral, coronary, and pulmonary vasodilatation. 70,71 Because of these effects, levosimendan could be useful in children with congenital heart disease. 72 The most important side effect is hypotension due to peripheral vasodilation. Levosimendan improves outcomes in adults with acute decompensation of chronic heart failure, and in adults with poor left ventricle function undergoing coronary artery bypass surgery. 63,64,73 In neonatal and infant congenital cardiac surgery patients, levosimendan was shown to be as efficacious as milrinone. 15,16 However, myocardial oxygen demand was significantly lower in the levosimendan group. In a pediatric study, levosimendan lowered PAP and increased cardiac index significantly more than dobutamine. 17 But when added to a standard postoperative protocol of milrinone and dopamine, levosimendan did not improve mortality, duration of MV, or hospital LOS in one study of 63 neonates. 18 After heart surgery, levosimendan improved peripheral oxygenation (NIRS) and lowered inotrope scores in 20 children. 19 The current level of evidence is insufficient to judge whether prophylactic levosimendan prevents LCOS and mortality in pediatric patients undergoing surgery for congenital heart disease. 74 The use of levosimendan is reported by 5% of respondents of this survey. Currently, there are three studies registered at clinicaltrials.gov comparing milrinone with levosimendan in neonatal cardiac surgery (NCT00549107, NCT01576094, and NCT00695929).
Calciumgluconate is often used based on the knowledge that the neonatal myocardium is calcium dependent. It increases MAP and SVR, probably due to peripheral vasoconstriction but has been shown not to increase cardiac index in adults or in premature neonates. 75 –77 The only report of calciumgluconate increasing myocardial contractility and cardiac output was in healthy horses without changing filling pressures or MAP. 78
Hypothyroidism, with prolonged ICU LOS, is well described in adults and children following CPB. 23,79 –81 Triiodothyronin supplementation may be a useful adjunct in the management of patients after CPB, improving cardiac index, cardiac function, and inotrope requirements, but its positive effect on clinical outcomes has not been established. 22,23,82,83
New inotropes like istaroxime, nesiritide, apelin, or omecamtiv mecarbil have shown some beneficial hemodynamic effects in adults, but there is too limited evidence in children at this time. 20 Costello et al compared nesiritide with milrinone and placebo in 106 children following Fontan operation and found no difference in cardiac index or survival. 20 None of the respondents in this survey reported their use.
Amrinone, a phosphodiesterase inhibitor, is not being used anymore but has been shown to increase cardiac output in children following heart surgery. 9,13,14
Postoperative Temperature Control
The use of hypothermia during heart surgery is well established, decreasing oxygen demand. Following congenital heart surgery, moderate hypothermia (32°C-33°C) has been used in children with refractory low cardiac output state. 84 In the retrospective study, cooling led to a significant increase in MAP, pH, and urine output and a decrease in heart rate, right atrial pressure, and platelet count.
Hyperthermia is known to increase oxygen consumption by 11% for every 1°C rise in temperature above 36°C. 85 Therefore, it has been advocated that normothermia should be maintained in children after cardiac surgery. 55 Most respondents of this survey routinely prevent hyperthermia or try to achieve a temperature below 37°C. Only 9% report to target 35°C to 36°C degrees routinely after congenital heart surgery with DHCA. Whether targeting hypothermia will improve outcomes remains to be investigated. At the moment no clinical trials comparing postoperative temperature management are registered at clinicaltrials.gov. The use of hypothermia for heart rate control is beyond the scope of this survey and review.
Future Research
It would be very interesting to investigate the difference between milrinone and other inotropes on mortality, duration of MV, and LOS in future randomized trials These multicenter trials need to be large enough, which can be a challenge requiring strict study protocols as many other factors may influence cardiac output postoperatively (eg, anesthesia, surgical techniques, CPB management and duration, postoperative sedation, extubation management, fluid management, and ICU treatment goals such as temperature, pH, blood pressure, etc). Furthermore, these studies have to focus on specific congenital defects as different disease states (eg, biventricular vs univentricular heart disease, VSD vs Fallot, Norwood versus Fontan, etc) will require different inotrope approaches. But first we may have to focus on the pharmacokinetic aspect of inotropes, assessing the effect of inotropic plasma levels on cardiac output and then try to find a dose–effect relationship. This will also need to be done in different age-groups. It will be very hard to convincingly show benefit of one inotrope over another in the many specific situations intensivists are faced with.
Currently three studies are comparing levosimendan and milrinone, hopefully these studies will be large enough to focus on the important clinical outcomes and not only the hemodynamic effects.
Limitations
The survey results are limited by the reliance on the self-reports by the participants. One limitation of the survey was that it did not specifically address the dosage of the different drugs that are being been used nor did we address the different types of LCOS. Another limitation is that the survey was set up to determine provider-dependent practice variation rather than center-dependent variation and it was therefore also not possible to compare practice variation between the different continents and/or countries. However, the average number of respondents per center is approximately 1.6, which is consistent for all centers apart from the European and South African centers which both had one respondent per center. Therefore, the practice variation we identified in all respondents also reflects practice variation in the different centers and probably indicates that practice variation is more center dependent than provider dependent.
Conclusions
There are several inotropes available to the (cardiac) intensivist with, more or less, well described hemodynamic effects. The use of these inotropes seems very logical and appropriate in the prevention and treatment of low cardiac output states following pediatric heart surgery. Different inotropes can be used for different clinical situations, but the choice of inotrope is up to the treating physician as there is a lack of compelling evidence in the literature favoring one inotrope over another or even placebo. Despite this currently insufficient evidence on clinically relevant outcomes, milrinone is, by far, most often used for the treatment and prevention of low cardiac output in children worldwide.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.