
Abstract
Background:
Paradoxical hypertension after repair of coarctation of the aorta is a well-known phenomenon. The pathogenesis involves the activation of the sympathetic nervous system (first phase) and renin–angiotensin system (second phase). Only a limited number of different treatment strategies have been published in the literature, without any comparative studies.
Methods:
Our aim was to describe the current international practice variation surrounding pharmacological treatment currently being employed to treat paradoxical hypertension following the repair of coarctation of the aorta in children. We performed an online survey among 197 members of the Pediatric Cardiac Intensive Care Society. We also conducted a systematic review of the literature regarding the treatment of paradoxical hypertension.
Results:
Eighty-eight people (45%), from 62 different centers, responded and answered the questions regarding blood pressure control. Nitroprusside is the first drug of choice for initial blood pressure control in 66% of respondents, esmolol in 11%, labetalol in 11%, and angiotensin-converting enzyme inhibitors (ACEIs) are used by 3% of respondents. For oral blood pressure control after discharge from the pediatric intensive care unit, 75% of respondents use ACEIs, 18% use labetalol, and 12% use other beta-blockers (propranolol, carvedilol, atenolol, metoprolol). The systematic review identified 14 articles reporting pharmacological treatment of direct postoperative hypertension following coarctation repair.
Conclusion:
There is wide practice variability, due to the lack of sufficient compelling evidence. The majority (66%) of caregivers use nitroprusside to control blood pressure in the acute postoperative phase. The ACEIs are the drug of choice for chronic blood pressure control.
Introduction
Paradoxical hypertension after repair of coarctation of the aorta is a well-known phenomenon. It can present early postoperatively (<24 hours) or after two to four days, and this delayed response is associated with abdominal pain due to arteritis and possible bowel necrosis. 1 And, even years after surgery, late hypertension can develop at long-term follow-up, which is also poorly understood but is possibly due to increased arterial rigidity. 2 This late hypertension is beyond the scope of this review.
Stage 1 hypertension in children and adolescents is defined as systolic blood pressure (SBP) and/or diastolic blood pressure (DBP) between the 95th percentile and 5 mm Hg above the 99th percentile. 3 Stage 2 hypertension, which many postoperative coarctation patients have, is defined as SBP and/or DBP >99th percentile plus 5 mm Hg. 4
The phenomenon of paradoxical hypertension is complex and has been the focus of intense study. There are several mechanisms involved in developing postoperative hypertension but its exact cause is not yet fully understood. 1 First, there can be a higher baroreceptor set point due to preoperative high blood pressure as adaptation to the need for sufficient renal perfusion, which can explain the immediate postoperative hypertensive response. Second, the stretch of the baroreceptors will reduce after surgery, causing elevated sympathetic nervous activity as demonstrated by higher epinephrine/norepinephrine levels after surgery compared to operations of similar magnitude. This can be a factor in initiating the delayed response. A third mechanism is activation of the renin–angiotensin–aldosterone system (RAAS) with elevated plasma renin activity (PRA) in the first week post-coarctectomy compared to patients after other cardiovascular operations. 1 A comparative study of balloon angioplasty or surgical repair of aortic coarctation also supports that paradoxical hypertension after coarctectomy is caused by sympathetic activation and RAAS activation. 5 The authors found a significant increase in SBP, DBP, and heart rate with increased PRA, norepinephrine, and epinephrine levels directly postoperatively in the surgical group. Conversely, in the balloon angioplasty group, a reduction in SBP and DBP was identified, without increases in catecholamine levels. 5
Several effective treatment strategies to lower blood pressure post-coarctectomy, targeted at the three above mechanisms, have been published in the literature, but the evidence is still limited. Paradoxical hypertension is known to respond to beta-blockers, arterial smooth muscle relaxants, calcium channel blockers (CCBs), and angiotensin-converting enzyme inhibitors (ACEIs). 6 -19 And new strategies are under development. 20 It is not known which antihypertensive strategy is the most effective, as no randomized controlled trials have been published comparing different strategies in the direct postoperative phase.
The aim of this study was to describe current international practice variation surrounding pharmacological management of paradoxical hypertension following repair of coarctation of the aorta in children. This was done as part of a larger online survey regarding prevention and treatment of low cardiac output syndrome (LCOS) we performed among Pediatric Cardiac Intensive Care Society (PCICS) members (in writing). The second objective was to perform a detailed and systematic review of the literature regarding pharmacological treatment of paradoxical hypertension following coarctectomy.
Methods
We performed a literature search in PubMed using words “aortic,” “aorta,” “coarctation,” “hypertension,” “coarctectomy,” “treatment,” and “antihypertensive agents.” We included all pediatric reports regardless of the year of publication.
In May 2014, we developed an online survey with questions regarding the prevention and treatment of LCOS (in writing]). As part of this larger questionnaire, we asked which antihypertensive medication was being used for the treatment of paradoxical hypertension directly following coarctectomy and which antihypertensive agents were being used in the chronic phase.
We sent an invitation to all 197 registered PCICS members to partake in the survey. Respondents were reminded of the survey after two and four weeks.
Results
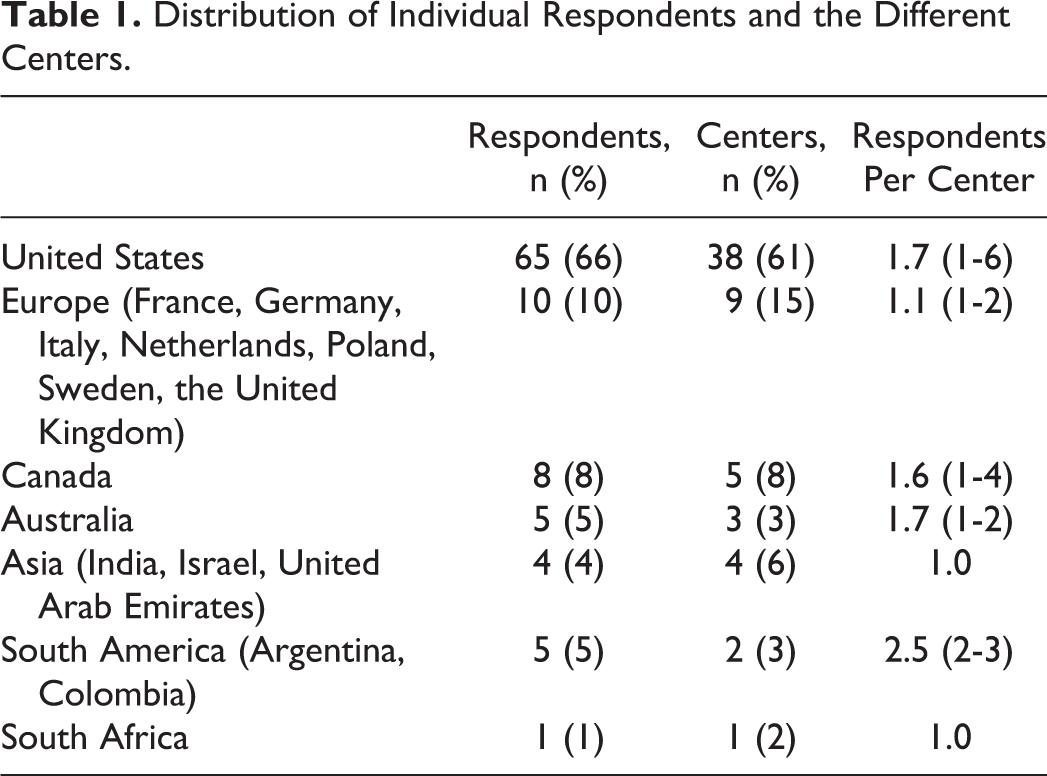
Ninety-eight (50%) people responded from 62 different medical centers across the world (center distribution: 61% United States, 15% Europe, 8% Canada, 6% Asia, 3% Australia, 3% South America, and 2% Africa; see Table 1). Fifty-six (73%) respondents were pediatric intensive care unit (PICU) consultants, 27 (35%) were pediatric cardiologists, and 23 (23%) were nurse practitioners. Several medical respondents were dually certified (mostly intensive care and cardiology). Most respondents (65%) worked in centers that perform more than 300 pediatric heart surgeries per year.
Distribution of Individual Respondents and the Different Centers.
Eighty-eight respondents (45%) answered the questions regarding blood pressure control following coarctectomy. Due to the setup of the survey, it is not possible to determine the summary statistics regarding center distribution, nationality, and occupation of this subgroup. Nitroprusside is the first drug of choice for initial blood pressure control in 66% (58/88) of respondents, esmolol in 11% (10/88), labetalol in 11% (10/88), ACEIs in 3% (3/88) of respondents (Table 2). Four (4%) respondents reported the use of other drugs, such as nicardipine, urapedil, and phentolamine. Another three (3%) respondents indicated that the choice of drug depended on left ventricle function and/or age of the patient.
Responses to the Question, “What Drug Do You Use First to Lower Blood Pressure in Children With Hypertension Following Coarctectomy?”
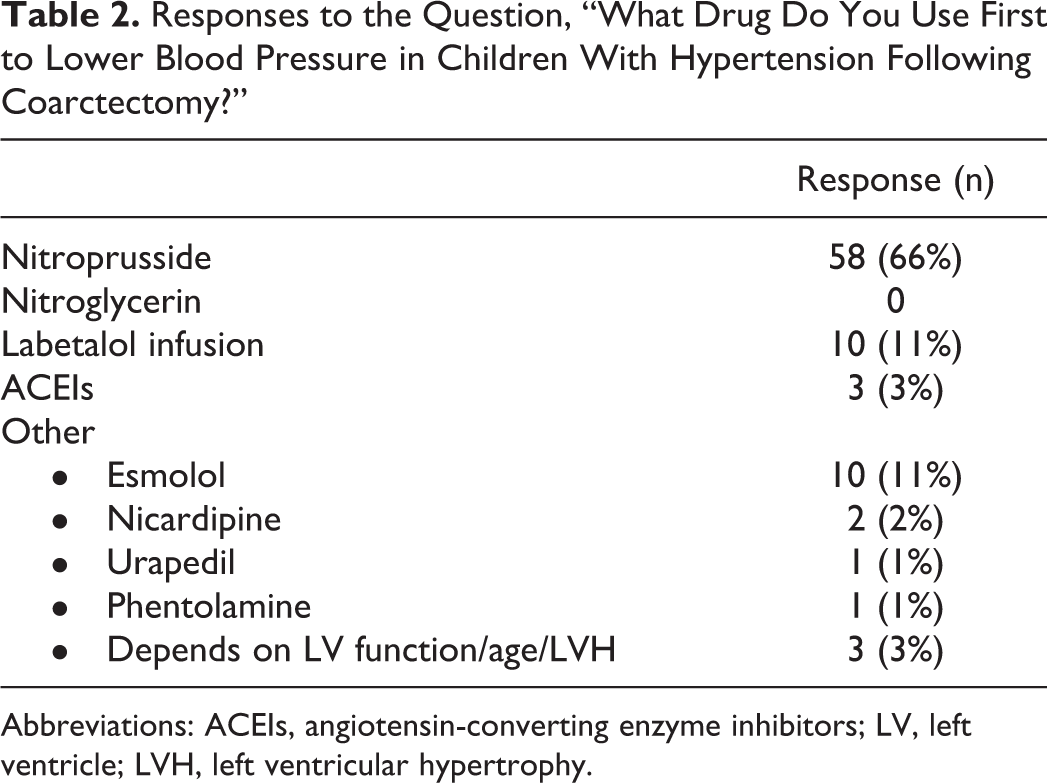
Abbreviations: ACEIs, angiotensin-converting enzyme inhibitors; LV, left ventricle; LVH, left ventricular hypertrophy.
For oral blood pressure control, 75% (65/87) of respondents use ACEIs, 18% (16/87) use labetalol, and 13% (11/87) use beta-blockers (propranolol, carvedilol, atenolol; Table 3). Three (3%) respondents reported the use of other pharmacological agents for oral blood pressure control, such as clonidine, nifedipine, or nitroprusside.
Responses to the Question, “What Drug Do You Use as Oral Antihypertensive Following Coarctectomy in Children?”
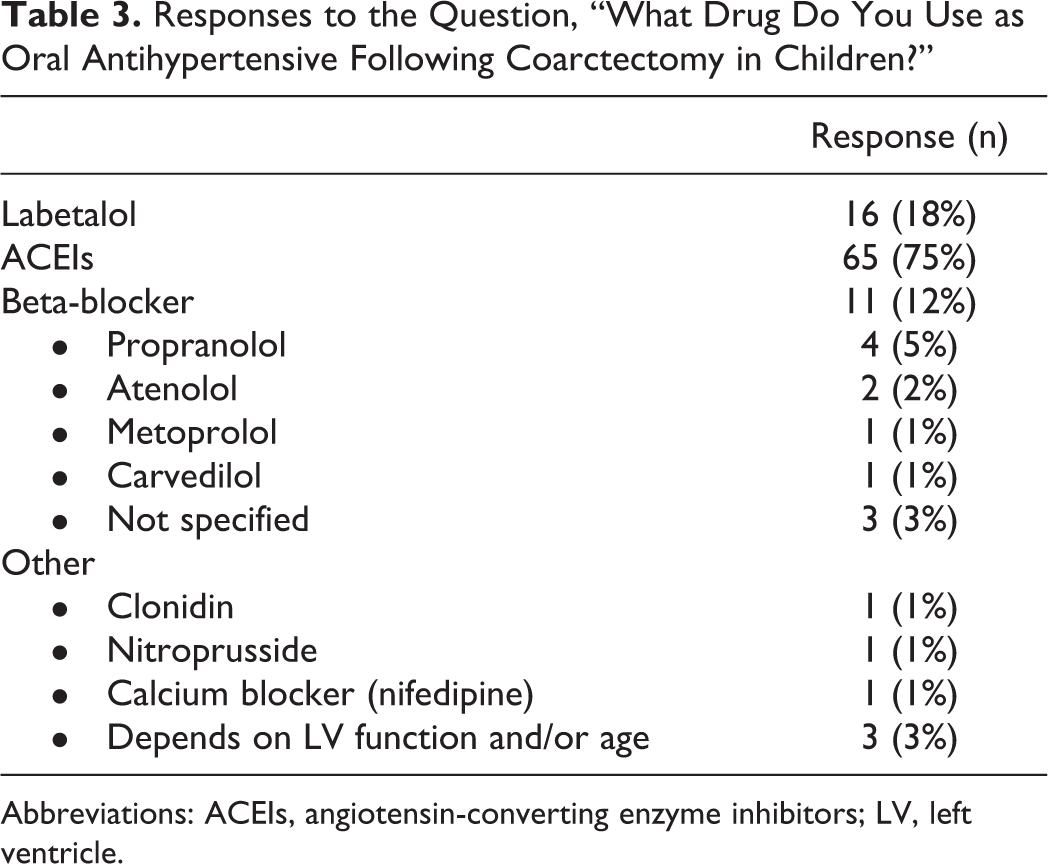
Abbreviations: ACEIs, angiotensin-converting enzyme inhibitors; LV, left ventricle.
We identified 14 articles, published between 1978 and 2016, discussing a pharmacological treatment for direct postoperative hypertension following repair of coarctation of the aorta in children (Table 4). The effect of esmolol on postoperative hypertension has been described in two reports from one prospective randomized trial, 16,17 one case series, 18 and one prospective study. Rouine-Rapp et al performed a placebo-controlled, prospective randomized trial on the effect of enalaprilat on postoperative hypertension. 14 Labetalol has been described in one very small case series. 6 Clonidine therapy in postoperative hypertension is investigated in one prospective trial. 23 The role of prophylactic propranolol has been described in two prospective trials. 9,21 And to our knowledge, there is only one case report about the effect of captopril postoperatively. 7 No studies have been published comparing different pharmacological agents.
A Summary of All Published Literature Regarding Drug Therapy for Paradoxical Hypertension in Children.
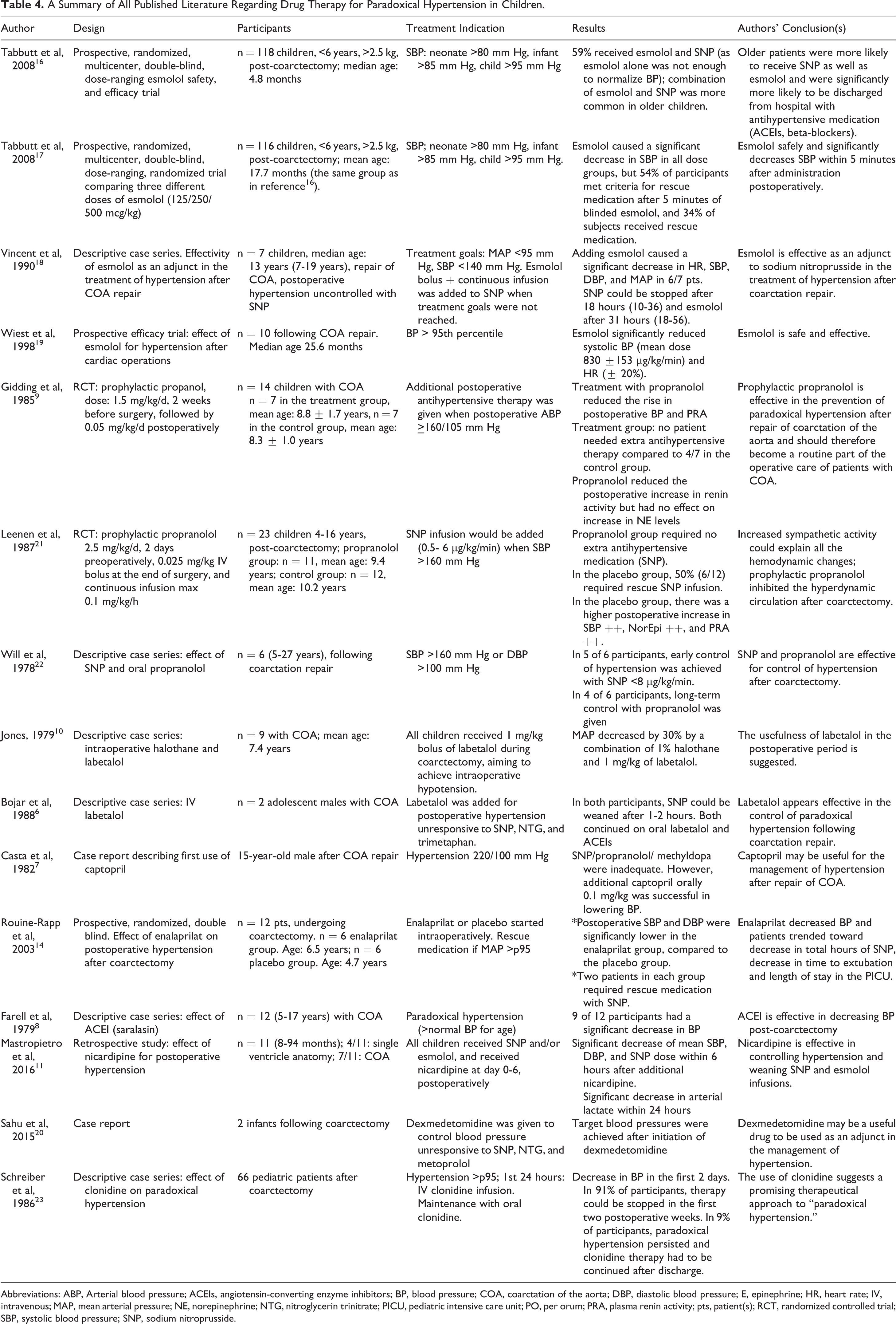
Abbreviations: ABP, Arterial blood pressure; ACEIs, angiotensin-converting enzyme inhibitors; BP, blood pressure; COA, coarctation of the aorta; DBP, diastolic blood pressure; E, epinephrine; HR, heart rate; IV, intravenous; MAP, mean arterial pressure; NE, norepinephrine; NTG, nitroglycerin trinitrate; PICU, pediatric intensive care unit; PO, per orum; PRA, plasma renin activity; pts, patient(s); RCT, randomized controlled trial; SBP, systolic blood pressure; SNP, sodium nitroprusside.
Discussion
Paradoxical hypertension following coarctectomy occurs in the first few days after surgery, is due to several mechanisms, and is known to respond to beta-blockers, arterial smooth muscle relaxants, and ACEIs. 1 The initial phase of direct postoperative hypertension is related to sympathetic activation and usually limited to 24 hours. 24 Hypertension in the initial phase can result in bleeding and/or hemodynamic compromise. The second phase occurs after two to four days and involves the renin–angiotensin system. Systolic and diastolic hypertension in the second phase can cause mesenteric arteritis, a syndrome characterized by abdominal pain, tenderness, ileus, nausea, vomiting, and leukocytosis. If untreated, this could result in peritonitis and possibly prove fatal. 6 The medications used to treat paradoxical hypertension target these different mechanisms to prevent the development of hypertensive complications, such as bleeding and/or mesenteric arteritis. At the moment, it is not known whether any treatment strategy is superior as the literature is limited to pediatric hypertension in general, with no specific advice for post-coarctectomy patients. 25
Our international survey shows that significant practice variability exists, which is also found in a very recent review of the American Pediatric Health Information System (PHIS) database. 26 The authors concluded that the variability in care and the use of newer drugs might be associated with greater costs and suggested that best practice and evidence-based guidelines are warranted for this population.
In the following section, we discuss the results of our survey in relation to the evidence found in our systematic literature search.
Sodium Nitroprusside
Our survey shows that most respondents (66%) use sodium nitroprusside (SNP), a direct vasodilator that increases cyclic guanosine monophosphate, resulting in vascular smooth muscle relaxation. Sodium nitroprusside is mainly used in the initial phase of postoperative hypertension caused by increased norepinephrine levels. Sodium nitroprusside is often used to manage hypertensive crises and hypertension after cardiac operations because of its ease of titration, short half-life, and its rapid onset and offset of action.
19,27
In the United States, SNP is used in 86% of patients with hypertension following coarctectomy.
26
Sodium nitroprusside reduces preload and afterload and can be beneficial in congestive heart failure induced by hypertension.
27
However, SNP is an indirect stimulator of the sympathetic nervous system and may further aggravate the increased sympathetic activity frequently present in patients who have had repair of aortic coarctation.
24,28
Furthermore, SNP can cause thiocyanate toxicity and may add to tachycardia, decreasing Pa
The first report on the effective use of SNP following coarctectomy is a descriptive case series of six patients (5-27 years old) described by Will et al in 1978. 22 In five of six patients, the authors achieved early control of hypertension with SNP <8 μg/kg/min in combination with propranolol. Unfortunately, no comment was made regarding the heart rate and/or the effect of propranolol on tachycardia, which often may be associated with SNP. In another small case series, SNP alone was ineffective in controlling postoperative hypertension, but by adding esmolol, blood pressure control could be achieved. 18 In two more recent studies, SNP was used as an effective rescue medication in 34% to 59% of patients whose blood pressure could not be controlled with esmolol alone. 16,17
Beta-Blockers
The basic mechanisms of paradoxical hypertension are sympathetic activation and renin stimulation, 1 both of which can be targeted using beta-blockers. 9,21 Esmolol, a selective short-acting beta-blocker, is an often-used alternative to SNP, being used in 59% of patients in the recent PHIS review. 26 Esmolol is the most studied in paradoxical hypertension; it has a half-life of 10 minutes and is the first drug of choice in 11% of respondents of our survey. 16 -19 Vincent et al first described esmolol in 1989 in seven children with a median age of 13 years, with postoperative hypertension unresponsive to SNP. Adding esmolol significantly lowered blood pressure in six of seven patients, and SNP could be stopped after a mean of 18 hours. 18 All patients were switched to oral antihypertensive therapy with propranolol and/or ACEIs. In 1998, a prospective esmolol efficacy trial showed that monotherapy with continuous esmolol, mean dose 830 ±153 mcg/kg/min, significantly reduced blood pressure in 10 children following coarctectomy as part of a larger trial of postoperative hypertension. 19 Target blood pressure (<90th percentile for age) was reached after 1.7 hours (0.6-3.6). Heart rate also significantly decreased by 20%. The authors concluded that monotherapy esmolol was safe and effective in reducing blood pressure in this small group of postoperative pediatric cardiac patients (n = 10). 19 In a more recent prospective, randomized, multicenter, double-blind, dose-ranging esmolol safety and efficacy trial by Tabbutt et al, esmolol was used for blood pressure control in the direct postoperative phase in 118 children under six years of age, undergoing coarctation repair via lateral thoracotomy, but 59% of patients also received nitroprusside infusion (0.5-8 mcg/kg/min). 16 And, with increasing age, patients were more likely to receive SNP in addition to esmolol. The median age in this study was lower (4.8 months) than in the study by Vincent et al (13 years). 18 The same group published the dose-ranging part of their trial separately comparing three different doses of esmolol (125/250/500 mcg/kg as bolus followed by 125/250/500 mcg/kg/min continuous infusion). 17 All three doses decreased SBP quickly and significantly, without any statistical difference between groups, but again 54% met criteria for rescue medication because SBP had not decreased below the levels of treatment indication five minutes after administrating the esmolol bolus. Thirty-four percent of participants actually received rescue medication with isoflurane, SNP, fentanyl, or propofol. The authors concluded that esmolol therapy is safe and effective. 17 However, in both studies by Tabutt et al, more than 50% of patients received additional therapy to esmolol, suggesting that monotherapy with esmolol is often not adequate. Esmolol is also used in other, noncoarctectomy-related, pediatric hypertensive crises, particularly when there is associated tachycardia. 27 It is advocated that esmolol should not be used when a hypertensive crisis is caused by catecholamine excess, as hypertension is perpetuated by persistent alpha stimulation. 19
In this survey, the use of beta-blockers as oral therapy in the postoperative phase was reported by 12%. Specific beta-blockers reported were propranolol, atenolol, metoprolol, or carvedilol. The only study describing the use of oral beta-blockers in the specific postoperative coarctectomy patients is the study by Will et al who describe the use of SNP in combination with oral propranolol in four of six patients with sustained hypertension following initial satisfactory control of blood pressure with SNP. 22 In adults who developed late hypertension 26 (±15) years after coarctectomy, metoprolol was found to have a more antihypertensive effect than candesartan, an angiotensin II receptor blocker. 29 In the United States, metoprolol is the only beta-blocker approved by the US Food and Drug Administration (FDA) for pediatric hypertension based on one trial in essential pediatric hypertension (not post-coarctectomy). 25
In 1985, Gidding et al advocated that prophylactic propranolol should become a routine part of the operative care of patients with coarctation of the aorta. 9 The authors had shown that two weeks of prophylactic propranolol and one week of postoperative propranolol significantly reduced the rise in postoperative blood pressure in seven children following repair of coarctation of the aorta (mean age 8.8 year ± 1.7). Leenen et al confirmed in a randomized, placebo-controlled, double-blind trial that prophylactic propranolol inhibited the hyperdynamic circulation after coarctectomy in 11 children (mean age 9.4 years). 21 The authors’ strategy entailed two days of prophylactic propranolol and six days of postoperative propranolol. None of the patients received rescue therapy with SNP, compared to 6 of 12 patients in the placebo group. In our survey, no questions were asked about prophylactic strategies, as our scope was postoperative care; therefore, information on the current use of prophylactic strategies is not available. We would hypothesize, however, that the prophylactic strategy has not found its way to the current routine approach to “coarctectomy care,” possibly because of the quickly effective postoperative treatments with SNP, esmolol, and labetalol. Moreover, since patients are operated at younger ages, postoperative hypertension is possibly not as therapy resistant as it used to be in the 1970s and 1980s.
Labetalol
In this survey, IV labetalol, a combined alpha-1 and nonselective beta-blocker, is used by 11% of respondents for the direct treatment of paradoxical hypertension following repair of coarctation of the aorta in children, compared to 20% in the recent PHIS review. 26
The IV labetalol has direct vasodilator properties, is easily titratable, and prevents reflex tachycardia. The beta to alpha blocking potency ratio is 3:1 for oral labetalol and 7:1 for IV labetalol, 13 but the majority of side effects can be attributed to alpha blockade (headache, dizziness). Labetalol has a relatively long half-life of three to five hours and is often used in children with hypertensive crises but should not be used in patients with bronchospastic disease or congestive heart failure as it has a negative inotropic effect. 27
In patients with coarctation of the aorta, labetalol was first described, in nine children, in combination with 1% halothane to control blood pressure intraoperatively. 10 In 1988, Bojar et al described two adolescent males with coarctation of the aorta, with postoperative hypertension unresponsive to SNP. 6 Both patients responded quickly to labetalol and SNP could be weaned off within two hours of starting labetalol. The IV labetalol could successfully be converted to oral labetalol. The authors concluded that labetalol addresses the basic mechanism of elevated sympathetic activity responsible for the postoperative hypertension and that it is an easy, effective, and safe medication for the control of paradoxical hypertension following repair of coarctation of the aorta. 6 There is no literature comparing labetalol with other beta-blockers. In the recent PHIS review, esmolol is used more frequently (60%) compared to labetalol (20%). 26 This is possibly due to the longer half-life of labetalol, compared to esmolol. Both agents are used by 11% of respondents of our survey.
Oral labetalol can be used in the long-term treatment of primary and secondary hypertension (eg, renal disease, autoimmune disease, essential hypertension), with few side effects in adults and children. 15 Labetalol has no pediatric FDA labeling. Oral labetalol for the control of hypertension in the second postoperative phase was reported by 18% of respondents in this survey.
Angiotensin-Converting Enzyme Inhibitors
Renin stimulation is mostly responsible for the second phase of paradoxical hypertension 1 ; however, the use of ACEIs in the management of the initial phase of postoperative hypertension is reported by 3% of respondents of our survey. The survey did not ask as to which ACEIs are being used. Angiotensin-converting enzyme inhibitors block the angiotensin-converting enzyme required for the conversion of angiotensin I to angiotensin II, a potent vasoconstrictor. Angiotensin-converting enzyme inhibitors also block angiotensin II-mediated aldosterone release, thereby preventing salt and water retention. 3 Blood pressure response to ACEIs is affected by ethnicity, with black children demonstrating lower antihypertensive effect compared to white children. 30
The effective use of an IV infusion of saralasin, a partial agonist of angiotensin II receptors, was described once (in 1979) in 12 children with immediate hypertension following coarctation repair. 7 No other reports regarding saralasin post-coarctectomy have been published. Currently, enalaprilat is the only available IV ACEI that can be effective in renin-mediated hypertension in the immediate postoperative phase with only limited data available on its use in children with hypertensive crisis. 27 Rouine-Rapp et al reported 14 children between 1 year and 18 years of age, receiving enalaprilat or placebo infusion after coarctectomy. 14 The enalaprilat group trended toward a decrease in the total hours of SNP and demonstrated improved control of SBP and DBP.
Oral captopril has been used in the first phase of paradoxical hypertension to lower blood pressure in children unresponsive to SNP, propranolol, and methyldopa. 7 But the renin–angiotensin system is attributed mostly in the second phase of postoperative hypertension, which is reflected in the fact that 75% of respondents of our survey use ACEIs as oral therapy. Captopril is one of the earliest ACEIs, with substantial evidence for its efficacy in children with renal or vascular secondary hypertension, although its usage is off-label. 3,12 Enalapril and lisinopril do have pediatric FDA approval. In pediatric populations, ACEIs are the most commonly prescribed antihypertensive for both primary and secondary hypertension, especially in children with chronic kidney disease and diabetic nephropathy. 3,31
Alpha-Agonist
The effective use of clonidine, a centrally acting alpha-agonist, has been described in one case series of 66 pediatric patients following repair of coarctation of the aorta. 23 Clonidine decreases sympathetic nervous system outflow, leading to peripheral vasodilatation and decrease in heart rate, blood pressure, and cardiac output. 32
None of the respondents of our survey reported the use of clonidine in the acute phase. One respondent (1/88 = 1%) reported the use of clonidine in the chronic treatment of paradoxical hypertension. Phentolamine, phenoxybenzamine, prazosin, and doxazocin are other alpha-blockers that are often used in catecholamine-induced hypertension, as in pheochromocytoma. 27 In this survey, the use of phentolamine in the acute phase was reported by one respondent (1.1%).
Dexmedetomidine, a selective alpha-2 receptor agonist with sedative and analgesic properties, is mostly used for sedation in the postoperative situation in the PICU. Common side effects are hypotension and bradycardia, suggesting a possible beneficial effect post-coarctectomy. Dexmedetomidine was shown to be effective in two infants as adjunct therapy in the treatment of paradoxical hypertension after coarctectomy. 20 Dexmedetomidine can safely be used in the extubated patient and is helpful in keeping the patient out of pain, less agitated, and calm, thereby preventing the rise in blood pressure and heart rate. 20
The CCBs
The CCBs achieve vasodilatation by blocking calcium entry into the vascular smooth muscle cell. Amlodipine, isradipine, nicardipine, and nifedipine are common oral CCBs used in primary and secondary pediatric hypertension. 3,11 The CCBs can safely be used in children with renal failure, as it is metabolized by the liver and does not have renal effects seen with ACEIs. 3 Nicardipine was used in 14% of patients, according to the recent PHIS review. 26
Regarding pediatric patients with coarctation of the aorta, Mastropietro et al recently demonstrated a significant decrease in mean SBP and DBP and a significant decrease in the dosage of SNP in children receiving nicardipine as a substitute for SNP or esmolol following coarctectomy. 11 Nicardipine is used as the first-line therapy in hypertensive crises in children, is well tolerated, efficacious, and can be used for a longer period of time without the fear of cyanide toxicity. 27 Tachycardia is a side effect of therapy. The use of nicardipine was reported by 2 (2%) of 88 respondents.
Other Strategies
Although furosemide has no pediatric FDA approval for hypertension, diuretics play an important role in the management of hypertension in children. They reduce blood pressure by decreasing sodium and water retention, thereby reducing extracellular volume. Diuretics are usually combined with other antihypertensive medications but have not been researched specific to paradoxical hypertension. 3
Hydralazine and minoxidil are FDA-approved vasodilators used in children, but none of respondents of this survey reported their use.
In older literature, reserpine and trimethaphan are often mentioned, but they are not used anymore. Intramuscular reserpine blocks sympathetic activity but has a slow onset of action and could not easily be titrated. Trimethaphan, a ganglionic blocker, can control blood pressure without producing tachycardia, but tolerance to its effects usually occurred after 48 hours. None of the respondents reported the use of these two pharmacological agents.
Limitations
This survey was designed to gain insight into the pharmacological strategies that are currently being used to treat hypertension following repair of coarctation of the aorta, as it is not known which could be the most effective strategy. It is also not known which blood pressure to target in the postoperative phase. Almost all the identified studies targeted different blood pressures (Table 3). Many centers target blood pressures below the 95th to 99th percentile for age. Unfortunately, we do not know the blood pressure targets employed as no questions were asked regarding treatment goals.
Another limitation is that the survey was set up to determine provider-dependent practice variation rather than center-dependent variation and it was therefore also not possible to compare practice variation between the different continents and/or countries. However, the average number of respondents per center is approximately 1.6, which is consistent for all centers apart from the European and South African centers. Therefore, the practice variation we identified in all respondents also reflects in the different centers and probably indicates that practice variation is more center dependent than provider dependent.
Conclusion
The results of the survey show that there is wide practice variation regarding the treatment of paradoxical hypertension following surgical repair of coarctation of the aorta. This variability in care may be associated with increased costs. 26
The systematic review of the literature shows that there is only limited evidence regarding the treatment of paradoxical hypertension. There is no evidence that one pharmacological strategy is superior to any other and often multiple drugs (eg, esmolol and SNP) are necessary to control blood pressure in the acute postoperative phase. In the recent PHIS review, patients received a median of three antihypertensive medications. 26 Sodium nitroprusside is the most widely used (66% of respondents), probably because of its ease of titration; however, tachycardia and cyanide toxicity are important concerns. There is no literature on monotherapy with SNP. Beta-blockers target the two important mechanisms, sympathetic activation and renin release, involved in paradoxical hypertension and seem a logical choice to control blood pressure. 1 Esmolol is the most studied; but in up to 59% of patients, monotherapy is not adequate in controlling blood pressure. 16,17 Both esmolol and labetalol are being used by 11% of respondents. Thirty years ago, the use of prophylactic beta-blockers has been shown to be effective in controlling postoperative blood pressure. 9,21 As the current use of prophylactic beta-blockers was out of scope of this survey, no data were gathered on this topic. However, this would be very interesting to investigate further. Other pharmacological approaches with alpha-agonists and/or CCBs have not found widespread use but deserve attention. Especially, nicardipine shows promising results. 11
In the second phase of paradoxical hypertension, most respondents use ACEIs to control sustained high blood pressure, targeting the renin–angiotensin system.
In conclusion, based on the literature it is not possible to advise one pharmacological agent over another and further research is warranted. It would be very interesting to start by comparing SNP with a beta-blocker (esmolol or labetalol) in a prospective randomized controlled trial with duration of antihypertensive therapy and PICU length of stay as primary end points. Secondary end points of such a study should include the development of side effects (eg, bradycardia, cyanide toxicity, hypotension), the development of complications from hypertension (eg, postoperative bleeding, rupture of anastomosis, and the development of mesenteric arteritis), and costs of treatment. Target blood pressures should be based on age-related normograms.
Footnotes
Authors’ Note
Both authors had full control of the design of the study, methods used, outcome parameters, analysis of data, and production of the written report
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.