
Abstract
Breast cancer screening in the United States is complicated by conflicting recommendations from professional and governmental organizations. The benefits and risks of breast cancer screening differ though by age which should influence shared decision-making discussions. Compared to older women, women ages 40 to 49 years have a lower risk of breast cancer, but the types of breast cancer that develop are often more aggressive with a poorer prognosis. Furthermore, younger women have a longer life expectancy and fewer comorbidities. The primary benefits of screening for women in their 40s are a reduction in breast cancer mortality, years of life lost to breast cancer, and morbidity of breast cancer treatment by detecting cancers at an earlier stage. Compared to older women, the risks of breast cancer screening in women ages 40 to 49 years includes more false positive recalls and biopsies as well as transient anxiety. Concerns regarding radiation induced malignancy and overdiagnosis are minimal in this age group. The shorter lead time of breast cancer in women ages 40 to 49 years also favors shorter screening intervals. This information should help inform providers in their shared decision-making discussions with patients.
Introduction
Breast cancer screening in the United States is controversial, with multiple conflicting published recommendations. The American College of Obstetricians and Gynecologists (ACOG), 1 American College of Radiology (ACR), 2 American Cancer Society (ACS), 3 National Comprehensive Cancer Care Network, 4 and U.S Preventative Services Task Force (USPSTF) 5 all reach different conclusions about when and how often to recommend screening mammography. Each organization places different relative weights on the benefits and risks of screening and uses different standards for evidence. Shared decision-making discussions with patients are a recommendation of several organizations and multiple tools are available online.6,7 While in principle shared decision-making is ideal, in reality it places a burden on providers to help their patients understand and weigh the benefits and risks of a complicated topic upon which expert panels disagree.
The risks and benefits of screening mammography vary by age. Breast cancer incidence peaks in the 70s (1 in 25 women), but one seventh of all new breast cancer diagnoses (45 280 new cases in 2019) are in women in their 40s (1 in 65 women).8,9 Breast cancer is also the most common cause of non-traumatic death in women aged 40 to 49 (3250 deaths in 2019). 10 Younger women are more likely to develop breast cancer at a more advanced stage with a larger tumor size and lymph node positivity, as well as a more biologically aggressive profile (ie, lower estrogen receptor [ER] positivity, HER2 overexpression, and higher nuclear grade). 11 Consequently, younger women have poorer prognoses with a higher risk of recurrence and breast cancer death compared to older women.12-14 These younger women with cancer are also more likely to have genetic mutations (eg, BRCA1).15,16 In fact, premature deaths due to breast cancer among women in their 40s accounts for the same years-of-life lost to breast cancer as women in their 50s and substantially more years-of-life lost than women diagnosed in their 60s. 3
The purpose of this review is to provide context for providers to better understand the individual benefits and risks of breast cancer screening for women aged 40 to 49 years.
Benefits
The primary benefits of mammography screening are a reduction in breast cancer mortality, years of life lost due to breast cancer, and morbidity of breast cancer treatment.
Reduced Mortality
Several metrics describe the impact of breast cancer screening on mortality. All organizations that disseminate screening guidelines agree that more aggressive screening invariably results in fewer deaths.1-5 Mortality reduction measures the percentage of deaths averted due to a specific screening strategy compared to an alternative screening strategy or no screening. As the screening age range expands and screening frequency increases, total mortality reduction improves. Annual screening mammography from ages 40 to 84 years yields a mortality reduction of 40% compared to no screening. 17 The specific contribution to mortality reduction from annual screening ages 40 to 49 years is 12% to 29%.18-20 The mortality ratio (observed breast cancer death rate divided by the expected death rate) is similar between women aged 40 to 49 at first screening, versus women over 50. 21 Another common metric is the number needed to screen (NNS), which reports how many women need to be screened to prevent 1 breast cancer death. Since the incidence of breast cancer is higher in older women, the NNS decreases with age. Estimates from 1 systematic review provide a NNS of 753 for women ages 40 to 49 years, in comparison to 462 and 355 for women ages 50 to 59 and 60 to 69 years, respectively. 22
Reduced Years of Life Lost
The mortality benefits of screening younger women are greater due to the longer life expectancy and often greater family and career responsibilities than older women. An estimated 30% of years-of-life lost due to breast cancer occurs in women diagnosed in their 40s. 3 Although breast cancer incidence increases with age, the increased incidence does not keep pace with shortened life expectancy. One year of life is gained for every 20 women in their 40s who undergo annual screening, while 45 women in their 70s must be screened biennially to gain 1 year of life.23,24 At the moment, no detailed studies are available that assess the socioeconomic impact of life-years gained from averting breast cancer deaths in young women compared to older women. However, it is safe to assume that the impact of breast cancer death on younger working-age women with families outweighs older women who are more likely to be retired from the workforce.
Reduced Treatment Morbidity
Screening detects breast cancers at an earlier stage. Compared to symptomatic cancers, screen detected cancers are typically smaller and without lymph node involvement. 25 This in turn affects prognosis with 5-year survival rates of 99% for localized disease, 86% for regional disease (eg, axillary lymph nodes), and only 27% for distant metastatic disease. 26 Stage also influences treatment options with more extensive disease requiring more aggressive surgery and radiation therapy. 27 This is reflected in data comparing treatment approaches between screened and unscreened women. Women ages 40 to 49 years who do not get screened are 3.4 times more likely to undergo a mastectomy, 4.6 times more likely to undergo axillary node dissection, and 2.5 times more likely to undergo chemotherapy, than screened women. 28 More extensive surgery is associated with increased post-surgical complications including persistent pain and lymphedema.29,30 As a result, the detection of earlier stage cancer by screening can substantially reduce the morbidity associated with breast cancer treatment.
Risks
The most commonly cited risks of mammography screening are overdiagnosis, false-positives, anxiety, and radiation injury.
Overdiagnosis
Overdiagnosis is the detection of cancer at screening that would otherwise have never been clinically evident in the woman’s lifetime. Overdiagnosis can be separated into 2 components: obligate and non-obligate. 31 Obligate overdiagnosis occurs when a woman dies from other causes before her screen-detected cancer becomes clinically apparent. Non-obligate overdiagnosis occurs when a screen-detected cancer fails to progress to being clinically apparent. All screening studies cause some overdiagnosis, as they aim to identify patients before they become symptomatic. Direct measurement of overdiagnosed breast cancer is not ethically feasible so estimates are based on randomized controlled trials and observational data. Well-designed studies provide an overall breast cancer overdiagnosis estimate of 10% or less.31-34 These estimates are for all women over 40 years, but are elevated by older women who have competing comorbidities and shorter life-expectancies.
Obligate breast cancer overdiagnosis in a 40-year-old woman is estimated at 0.1% because of her long life expectancy and low all-cause mortality.31,35 Non-obligate overdiagnosis is also very low because of the higher likelihood of biologically aggressive cancer and the long duration over which even a slow growing cancer has to progress. No cases of spontaneous regression or disappearance were reported among 479 untreated cancers visible on imaging. 36 Consequently, a rare non-progressive breast cancer detected via annual screening mammography at age 40 would still be apparent on biennial screening mammography at age 50. Therefore, although breast cancer overdiagnosis may influence an older woman’s decision of when to stop screening, the extremely low rates of overdiagnosis in women aged 40 to 49 years should not influence when to start or how often to undergo screening.
False-positives
There are 2 types of “false-positives” in breast cancer screening: false-positive recalls and false-positive biopsies. In a false-positive recall, a woman without breast cancer is recalled from a screening mammogram for additional images to evaluate a questionable area. This occurs in ~6.5% of screening mammograms (Figure 1). 37 A false-positive recall does not refer to a woman being told she has breast cancer when in fact she does not, it instead refers to a request for additional imaging that turns out to be normal or benign. False-positive recall rates are affected by the age at which women start screening. On average, a woman who starts annual screening at age 40 will have 1 false-positive recall every 10 years, while a woman who starts at age 50 will have 1 false-positive recall every 11.5 years.17,38 Of note, the recall rate is approximately 50% higher on a baseline mammogram because the stability of potentially benign findings cannot be assessed. 38 As a result, there will be a bump before subsequent normalization in false-positive recalls at whatever age a woman starts screening.

Flow chart demonstrating the frequency of false-positive recalls and biopsies based on 1000 screening mammograms.
About 15% of women undergoing a diagnostic exam after a screening recall will be recommended for biopsy and approximately 1 quarter of these biopsies will identify cancer. 37 The remaining biopsies are considered false-positive biopsies as they identify benign tissue or atypical/pre-cancerous cells (Figure 1). Modern core needle biopsy devices sample a sufficiently large amount of tissue that a needle biopsy will not indicate malignancy when the lesion is actually benign. Furthermore, the complication rates following a needle biopsy are less than 1%. 39 The rates of false-positive recalls (~10%) and biopsies are driven by benchmark targets recommended by the ACR and Agency for Health Care Research and Quality.40,41 Countries such as the UK with lower recall rate targets (~3%) have concomitant lower false-positive recall and biopsy rates. 42
Anxiety
Anxiety is commonly reported following a screening recall or biopsy due to the possibility of breast cancer. 43 Women report that time seems to pass slowly and may use coping mechanisms to combat their uncertainty. 44 Anxiety is often cited as a harm of breast cancer screening because it is considered unnecessary when most women undergoing screening are healthy. Although the emotional experience following recall or biopsy can be intense, these feelings are short-lived, with no measurable long-term anxiety.43,45 Women are typically able to undergo additional diagnostic imaging or a biopsy in a timely fashion and view these subsequent tests as an “acquittal.” 44 Furthermore, after a false-positive mammogram women report an increased awareness of the possibility of developing breast cancer and a greater desire for future screening, as it gives them a sense of safety and reassurance.43,44 This in turn leads to an appreciation of life and devotion to healthy lifestyles.44,46 Some studies reported that following the anxiety of a false-positive mammogram there was a reinforced belief in the benefits of screening, imaging technology, and risk reduction.43,45 Fortunately, educational interventions aimed at providing information about breast cancer screening and offering emotional support can be implemented to help ameliorate the acute anxiety associated with breast cancer screening. 43
Radiation Injury
Exposure to radiation is cited as a potential harm of screening mammography. 5 Federal law sets a regulatory limit of 3.0 mGy for each mammogram view of an average sized breast, and a typical screening mammogram includes 2 views of each breast. 47 Modern digital mammography and digital breast tomosynthesis typically uses radiation doses far less than the mandated upper limit. 48 It is estimated that a woman undergoing annual screening mammography from age 40 to 49 will develop a fatal radiation-induced breast cancer on average once every 76 000 to 97 000 years. 49 Radiation safety in radiology overall is very important, but the extremely low risk of radiation-induced injury from mammography should not deter screening.
Screening Interval
Breast cancer screening interval recommendations for women aged 40 to 49 vary between annual and biennial (Table 1). Ideally, the screening interval should be shorter than the lead time for cancer detection. Because breast cancers in younger women are more aggressive, the lead time for women aged 40 to 49 years (1.7 years) is shorter than older women (3.3 years for women aged 50-59; 3.8 years women for aged 60-69 years; and 2.6 years for women aged 70-74).50,51 Consequently, younger women who undergo biennial versus annual screening are more likely to have larger tumors, positive nodes, and later stage disease.38,52,53 Women in their 40s undergoing annual rather than biennial screening mammography have a higher percentage of Stage I (55.5% vs 48.3%) and lower percentage of Stage III/IV (10.1% vs 14.9%) breast cancers. 38 Differences in breast cancer stage based on screening interval are less pronounced among older women due to the slower cancer growth.
Mammography breast cancer screening recommendation for average risk women by professional societies and organizations.
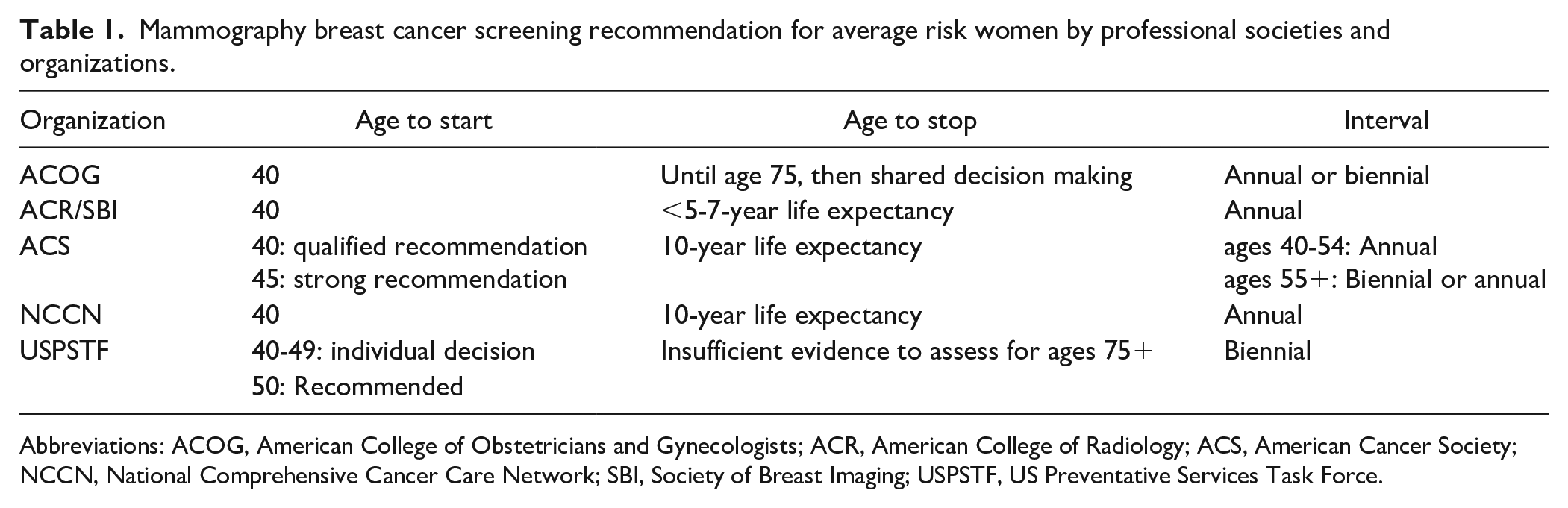
Abbreviations: ACOG, American College of Obstetricians and Gynecologists; ACR, American College of Radiology; ACS, American Cancer Society; NCCN, National Comprehensive Cancer Care Network; SBI, Society of Breast Imaging; USPSTF, US Preventative Services Task Force.
Conclusion
The benefits and risks of mammography screening for women in their 40s are different than for older women due to their longer life expectancy, reduced comorbidities, and greater likelihood of more aggressive breast cancer. The primary benefits are mortality reduction, number of years of life saved, and improved treatment morbidity. Compared to older women, younger women have more false positive recalls and biopsies causing transient anxiety. Concerns regarding radiation induced malignancy and overdiagnosis are minimal in this age group. All medical decisions should be personalized via shared decision-making between patients and providers. For women in their 40s, efforts to ameliorate the risks of screening mammography can notably tilt the risk-benefit ratio favorably and provide improved outcomes for patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.