
Abstract
Introduction:
HealthPathways is a clinical information portal developed in New Zealand that enables general practitioners to manage and refer their patients in a local context. We analyzed specialist outpatient appointment costs in Mackay, Queensland before and after HealthPathways implementation.
Methods:
We retrospectively examined specialist outpatient costs for patients referred by Mackay general practitioners for conditions with varying levels of HealthPathways implementation. Ranked from most clinical pathways available to none, chronic diabetes, cardiology, respiratory, and urology visits from January to March 2015, pre-pathways, and January to March 2017, post-pathways, were assessed. Monte Carlo simulation was used to estimate cost changes. Per-visit costs were multiplied by visit numbers to estimate policy impact.
Results:
The mean cost per visit increased from $220 to $305 for diabetes and $270 to $323 for respiratory, and decreased from $296 to $257 for cardiology and $444 to $293 for urology. The policy impact for each disease group over 3 months after accounting for visit numbers was a likely saving of $30 360 for diabetes and $10 270 for cardiology, and a likely cost increase of $24 449 for respiratory and $20 536 for urology.
Conclusions:
We observed that conditions with more comprehensive clinical pathways cost Mackay HHS substantially less following implementation. Costs for low and no pathway implementation referrals increased slightly over the same period.
Keywords
Introduction
HealthPathways is a web-based health information system that guides clinicians through complex referral decisions in local healthcare settings. It was developed in New Zealand by the Canterbury Initiative in 2008 for 550 clinical pathways and continues to grow. 1 The pathways are designed to assist with primary patient care and are jointly developed between general practitioners (GPs), specialists, nurses, and allied health professionals across all sectors. They provide the current best practice, as determined by the local health service, for diagnosis, management, and referrals across a variety of disease groups. The main benefits purported by HealthPathways are improved clinical confidence in referral appropriateness and an overall improvement in service integration.2-4
Referral patterns are influenced by a variety of factors, especially in complicated cases or when GPs are uncertain of the latest guidelines, referral contexts, and whether an escalation in care is required. 5 Informally, GPs often seek advice through “curbside” consultation, in which GPs briefly discuss patient care with specialists prior to or in lieu of a formal referral, 6 and around half of all GP-to-specialist referrals in a 2002 study were due to GPs seeking specialist advice. 7 HealthPathways can potentially serve as a substitute for some of these consultations, providing support when referral decisions are complex. This can potentially improve health service delivery, but economic evidence of clinical pathways is minimal. 8
This economic analysis of HealthPathways examines referral patterns and specialist consultation costs in Mackay, Queensland from 2015 to 2017. The primary research question was whether a clinical knowledge and referral appropriateness portal could reduce the costs of referred specialist outpatient appointments. We examined 4 clinical pathways at varying stages of implementation by comparing pre- and post-HealthPathways costs using Monte Carlo simulation.
Methods
Setting
Mackay HealthPathways went live in June 2015. It was jointly implemented by the Northern Queensland Primary Health Network (NQPHN) and the Mackay Hospital and Health Service (HHS). The patient population included all Mackay HHS patients who had been referred by GPs to specialist outpatient facilities for the following 4 conditions: cardiovascular disease, diabetes, urological disease, and respiratory disease. Mackay is a regional city on the eastern coast of Queensland with a catchment of over 90 000 km2. Its HHS serves over 182 000 patients per year as of 2018, of which around 5% are Aboriginal and Torres Strait Islander. 9
HealthPathways Implementation
Pathway components included clinical knowledge and referral information. Clinical knowledge pathways provided GPs with up-to-date evidence on a variety of medical conditions including best practice for assessment, diagnosis, and management, such as diagnostic thresholds or risk factors. Referral advice pathways displayed the local health service map to help select a referral destination appropriate for the patient.
By January 2017, the diabetes pathway was regarded as virtually complete. It featured 19 different clinical knowledge pathways and comprehensive referral information within Mackay HHS. The cardiology pathway included 11 completed clinical knowledge pathways and comprehensive referral information and was regarded as mostly complete. The respiratory pathway featured 9 completed clinical pathways, but did not include referral information, and was regarded as mostly incomplete. The urology pathway was not available until after the evaluation period, and serves as the counterfactual (Table 1). No other referral quality interventions were undertaken in Mackay during this period unless they went through HealthPathways. We used the total budget allocated by Mackay HHS and NQPHN to developing and maintaining HealthPathways as the implementation costs over this period.
Implementation Date and Availability of Various HealthPathways Portals for Mackay HHS From 2015 to 2017.

Study Design and Statistical Analysis
We used a retrospective pre-post study design to investigate the impact of HealthPathways. January to March 2015 utilization (pre) was compared to January to March 2017 utilization (post), with 2016 serving as a wash-out period as GPs became acquainted with the program. Specialist outpatient costing data was provided by Mackay HHS using the Transition 2 cost system, an accounting software that aggregates itemized overhead, staffing, imaging, and pathology costs for each patient visit. All specialist referrals in Mackay that were referred by a GP for each disease group were included in our dataset.
We used Monte Carlo simulation to estimate the likely changes to specialist visit costs and quantify uncertainty. 10 Monte Carlo simulation is a technique that uses random samples drawn from probability distributions. We selected this method because our data were highly skewed and multi-modal, likely due to the itemized nature of the accounting software and the costs it reported. We wished to make our findings generalizable to other health services which may not use the same costing methods.
As costs were positive and non-zero with significant right skew, we applied Gamma generalized linear models assuming a log link. Resulting estimates for pre- and post-HealthPathways costs for each disease group were used as model inputs for our Monte Carlo simulation to assess parameter uncertainty over 10 000 simulations. Policy impact was assessed by multiplying expected costs and number of visits. All costs were valued in 2017 $AUD using a 3% discount rate.
Ethics Approval and Funding
This study was approved by the Townsville Hospital and Health Service Human Research Ethics Committee (HREC) and Queensland University of Technology HREC (approval numbers HREC/17/QTHS/243 and 1700001131, respectively). Funding for publication of this paper was provided by the Mackay Institute for Research and Innovation.
Results
Specialist Outpatient Visit Costs
Pre- and post-implementation costs are shown in Table 2. From 2015 to 2017, costs increased for diabetes and respiratory visits, but declined slightly for cardiology and substantially for urology visits. Overall number of visits declined for diabetes and cardiology, but increased for respiratory and urology. The number of unique patients decreased from 121 to 73 for diabetes and 287 to 183 for cardiology, and increased from 84 to 97 for respiratory and 60 to 113 for urology, though these populations are likely to overlap. This led to a reduction in visits per patient for the diabetes and respiratory groups, but an increase for the cardiology and urology groups.
Visit Numbers and Monte Carlo Simulation Results for Pre- and Post-HealthPathways Outpatient Specialist Appointment Costs.

Abbreviations: IQR, interquartile range; SD, standard deviation.
Policy Impact
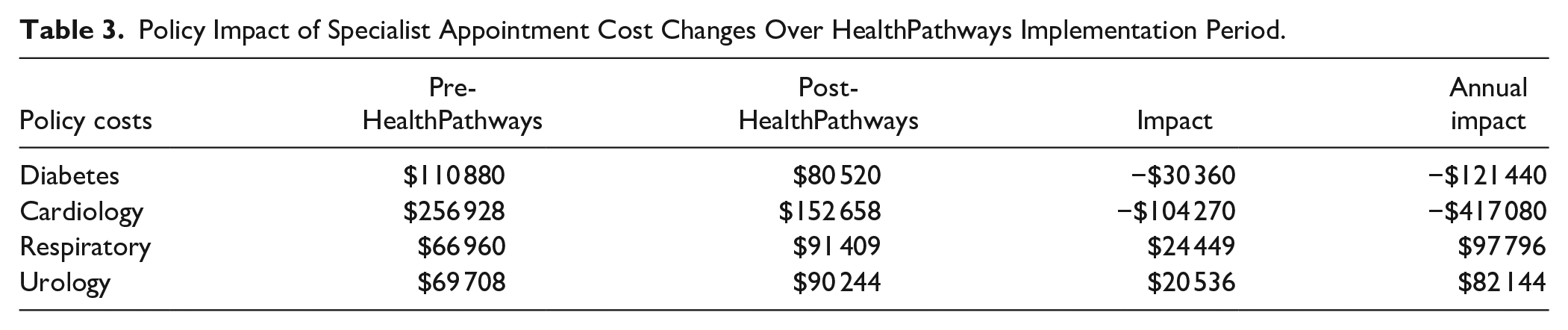
Applying cost findings to the overall utilization of specialist appointments, HealthPathways implementation was associated with a savings of $134 630 when including only pathways with referral information available, and a savings of $110 181 when including all 3 clinical pathways. These figures can be multiplied by 4 to summarize annual impact (Table 3), though annual results may be underestimates as utilization may increase in winter.
Policy Impact of Specialist Appointment Cost Changes Over HealthPathways Implementation Period.
The up-front investment cost of establishing Mackay HealthPathways was $282 400. The subsequent annual cost to support a team that updated best practices, referral networks, and new disease groups was $369 400 as of 2017, though this was expected to decline as more pathways were completed and attention shifted to mostly maintaining existing networks rather than developing new ones.
Discussion
Findings and Policy Impacts
The 2 disease groups with comprehensive referral information coincided with a reduction in costs for the HHS overall, while the disease groups with clinical knowledge pathways only and no pathways at all saw increased expenditure. The relatively unchanged respiratory costs and visits suggest that the clinical knowledge pathway may not be as important as the referral pathway, though it may offer other benefits that are not borne out in this analysis.
We noted significant uncertainty in our Monte Carlo results, with cost savings largely driven by the reduction in visit numbers rather than per-visit costs. Diabetes and cardiology patients in particular experienced a notable drop in visits per patient, while respiratory visit rates remained unchanged and urology rates increased. These findings indicate that these clinical pathways may have enabled GPs to manage more patients outside of specialist care, though this assumption requires further testing.
This is the first quantitative analysis of HealthPathways using economic outcomes. An evaluation on the same program reported potential cost savings, albeit with significant assumptions about the quality of referrals. 11 An evaluation report on referral rates and quality following HealthPathways implementation in Sydney found mixed results, likely due to the complex and multifactorial nature of primary care referrals and questions around GP engagement. 12 While several studies have been published on the engagement of primary care users,2,13-15 which may begin to explain the mechanism of cost reductions noted here, substantially more research is required to validate our assumptions and results.
Limitations and Implications for Evaluating Cross-Disciplinary Programs
We were made aware that a new urologist began working in Mackay in 2016; the urology pathway may therefore reflect pent-up demand from before 2016, compromising the group’s validity as a counterfactual.
Clinical advice, direct management, pre-surgical consults, or patient demand can all account for a GP’s referral decision. 5 We were unable to comment on the reason for observed changes in referral patterns and whether these changes were positive or negative for patients. Increased management within the primary sector may be a net positive if patients do not require escalation, but it may be undesirable if it leads to under-referral of patients that should be managed in a higher acuity setting. Prior research has shown that primary care can act as a substitute for low-acuity specialist care in a targeted intervention, 16 but linked patient data is required to validate this assumption in the Australian context.
We attempted to collect primary patient health indicators to determine whether shifting to primary care had any outcomes on patient health. The NQPHN’s GP database, Pen Clinical Audit Tool, was incomplete, only containing a small percentage of Mackay practices in 2015. In addition, patient outcomes were only collected at the clinical practice aggregate level. It was not feasible to use the aggregated data to evaluate changes to the 4 disease groups reviewed in this evaluation.
Future analysis of clinical pathways must also account for implementation-specific factors at the practice level, such as GP uptake. This is to gauge the treatment effect of HealthPathways and compare practices with strong adherence to practices with weak or no adherence to the program.
Due to data availability, this paper is an observational analysis of costs over the implementation period of HealthPathways, rather than a comprehensive evaluation. Other quality improvement programs across diabetes and cardiology care in Mackay may have impacted these figures, and epidemiological factors may have also played a role. Diabetes and cardiology may represent disease groups that are better suited to primary care management or HealthPathways intervention.
Research to establish the economic basis for clinical pathways is important to justify continued support from both primary and outpatient/acute funders. Input from the HHS, which does not provide primary care, was required to ensure HealthPathways was feasible, however from a balance sheet perspective there was little incentive to do so. This is the first study that investigates whether investing in primary care pathways can generate cost savings for secondary and tertiary care providers.
Conclusions
We observed outpatient visits over a comparable 3-month period before and after HealthPathways implementation. We found it likely that HealthPathways coincided with a reduction in outpatient spending, with potential savings in the hundreds of thousands for the HHS. However, we were not able to link this with a change in patient outcomes or an evaluation of whether HealthPathways was cost-effective.
Inability to link primary utilization with secondary and tertiary utilization limits the impact that can be demonstrated, with significant implications for public health. While having perfect data is not feasible, improved data linkages and more granular primary care data could improve the viability of comprehensive evaluations in the future.
Footnotes
Acknowledgements
Sara Baniahmadi for ethics application support; Bianca Cross for PenCAT data extraction and interpretation; Emma Moohin for assistance with data collection and communications support; and Silas Lui for epidemiological consultation on population statistics.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors at the Mackay Hospital and Health Service and the Northern Queensland Primary Health Network receive a salary from the 2 institutions that partnered to implement HealthPathways in Mackay.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Publication funding was provided by the Mackay Institute of Research and Innovation.