
Abstract
Introduction:
The proportion of patients who are frequent attenders (FAs) varies from few percent to almost 30% of all patients. A small group of patients continued to visit GPs year after year. In previous studies, it has been reported that over 15% of all 1-year FAs were persistent frequent attenders (pFAs).
Objectives:
This study aimed to identify typical features of pFAs from the textual content in their medical entries, which could help GPs to recognize pFAs easily and facilitated treatment.Methods: A retrospective register study was done, using 10 years of electronic patient records. The data were collected from Finnish primary health care centers and used to analyze chronic symptoms and diagnoses of pFAs and to calculate the inverse document frequency weight (IDF) of words used in the patient records. IDF was used to determine which words, if any, are typical for pFAs. The study group consisted of the 5-year pFAs and control group of 1-year FAs. The main background variables were age, gender, occupation, smoking habits, use of alcohol, and BMI.
Results:
Out of 4392 frequent attenders, 6.6% were pFAs for 3 years and 1.1% were pFAs for 5 years. Of the pFAs, 65% were female and 35% were male. The study group had significantly more depressive episodes (P = .004), heart failure (P = .019), asthma (P = .032), COPD (P = .036), epilepsy (P = .035), and lumbago (P = .046) compared to the control group. GPs described their 5-year pFAs by words related to lung and breathing issues, but there was no statistical difference to the 1-year FAs’ descriptions.
Conclusion:
A typical pFA seems to be a woman, aged about 55 years with depressive episodes, asthma or COPD, and lower back pain. Physicians describe pFAs with ordinary words in patient records. It was not possible to differentiate pFAs from 1-year FAs in this way.
Keywords
Introduction
A definition of a frequent attender (FA) or a persistent frequent attender (pFA) in primary healthcare varies. The proportion of patients who are FAs varies from few percent to almost 30% of all patients.1,2 Frequent attendance is usually a transitory phenomenon, but Gill and Sharpe 3 noticed that frequent attending seems be persistent in many cases. Koskela 4 found that female gender, body mass index (BMI) above 30, and previous use of healthcare services predict persistent frequent attendance. Carney et al 5 reported that within 5 years most FAs had returned to normal consulting habits, but there was a small group of patients who continued to visit GPs year after year for 20 years.
Smits et al 6 defined pFAs as patients who continued their high utilization of GPs during a 3-year period. They reported that 15.4% of 1-year FAs were pFAs. Andersson et al 7 reported that 14% of 1-year FAs were still frequent attenders 5 years later.
More than 2 decades ago, Neal et al 8 published an editorial in which they considered why some patients attended so frequently. They had noticed that FAs caused stress to GPs and increased their workload. They concluded that substantial resources might be saved by rationalizing primary care treatment of these patients and by avoiding unnecessary referrals, investigations, and treatments.
Jörgensen et al 9 reported that gender, lifestyle (obesity, smoking, exercise, and alcohol use), and socio-demographic factors were independent determinants of frequent attendance, but due to their study design, it was not possible to discriminate between 1-year FAs and pFAs. Patel et al 10 found that pFAs in primary care had often many persistent physical and mental diseases. Smits et al 11 reported in their study that a pFA is characterized by chronic diseases, psychiatric problems, and females are more likely than males to be pFAs.
Smits et al 12 published an article reporting on their previously developed model to predict which FAs become pFAs. Their prediction model for pFAs was based on data collected solely from GPs’ electronic medical records of patients.
In this study, our aim was to determine prevalence and characteristics of pFAs in primary healthcare in the study city. Studies exist regarding how to recognize pFAs and how to predict who will be pFA;4,9-11 however, to the best of our knowledge, this is the first study to attempt to identify this population using electronic patient record entries.
Material and Methods
This was a registry-based cohort study. The study city is the sixth largest in Finland with c. 190 000 inhabitants, 8% of whom are immigrants. GPs worked in 13 separate public healthcare centers and the primary care emergency clinic of the city. All inhabitants can use these publicly financed services. GPs have a capitation base payroll system with c. 2300 inhabitants in their patient list. Nurses manage part of the visits for some chronic diseases. Working-age people may also receive health services from occupational health care. In the study city there were 1.1 million GP consultations in total during the study years, of which 8.9% involved FAs every year. 13 Of all patients in primary care, approximately 10% in a given year are FAs; this population uses 70% to 80% of the primary health care resources in Finland.
The primary data were collected from healthcare centers in the study city. The data for patient entry word analysis of the pFAs and their 1-year FA controls were obtained from the same healthcare centers’ electronic patient record system (Pegasos®). GPs and nurses recorded all patient entries in Pegasos® as the same system covered all healthcare centers in the city. An FA was specified as a patient who had 10 or more face-to-face consultations to a GP during 12 months. A pFA was specified as a patient who was a FA at least 3 years.
Patient characteristics: We found out how many individual FAs had visited the healthcare centers in 2001 to 2006. In this cohort, we examined the number of FAs from 1 to 6 years. A more detailed analysis was performed for the 5-year pFA group (n = 49), which formed our study group. There were 47 adults and 2 children in this subgroup. All patient record entries (10 056 pages) of this study group were manually checked (AKS) and the background variables recorded. These were age, gender, marital status, occupation or education, number of electronic patient record pages, number of referrals to secondary care, smoking habits, use of alcohol or illicit drugs, and BMI. We also sought variables that might predict which patients are at high risk of becoming pFAs. AKS also counted the number of different diagnoses entered by the GPs. The diagnoses were classified according to the International Statistical Classification of Diseases and Related Health Problems of the World Health Organization (ICD-10).
We analyzed the differences in frequencies of long-lasting symptoms and chronic diagnoses (ICD-10 codes) between the adult study group (n = 47) and the control group, which consisted of age- (±6 months) and gender-matched controls (n = 94) for each adult in the study group. The control group consisted of 1-year FAs in the 2001 to 2006 period (n = 3539). The ICD-10 diagnoses for this analysis were obtained directly from Pegasos®.
Text analysis: In the text analysis of the electronic patient entries, we used the anonymized patient entry data of 147 FAs. The data consisted patient entries of the 5-year pFAs (10 056 anonymized electronic patient record pages) and 9118 pages of their 1-year FA controls. We used only the entry remarks made by GPs or nurses. The data for text analysis were obtained from 2001 to 2010 and analysis was undertaken in 2018. We performed analysis of words to determine whether GPs and nurses used different words in describing pFAs compared to 1-year FAs.
Data Analysis: The background variables of the study group were analyzed by means and standard deviations or frequencies and percentages. We used the χ2 test to examine the difference in gender distribution between the 1-year FAs and those FAs who visited GPs for 2 to 6 years through the 2001 to 2006 study period. We used conditional logistic regression analysis to compare the ICD-10 diagnoses of long-lasting symptoms and chronic diseases between the adults in the study group and their controls. Results are expressed as odds ratios with 95% confidence intervals. P-values <.05 were considered statistically significant. Statistical analyses were conducted using the SAS System for Windows, release 9.2 (SAS Institute Inc., Cary, NC, USA).
We performed a statistical text analysis of pFA patient entries in the study group and the control group’s patient entries. In this word analysis, we calculated the inverse document frequency (IDF) weight for each word in the patient entries of both groups. 14 We extracted the words that had the largest IDF weight difference between the 2 groups. Then, we analyzed those words by using means or frequencies and meanings of the extracted words.
The research grant was awarded by the health and social services of the city of Turku. Our research data were based on mandatory health records, which are collected according to Finnish health register legislation, and which may be used in scientific study without informed consent.
Results
We found 4392 individual FA patients in 2001 to 2006. There were 288 (6.6%) patients whose frequent attendance persisted for 3 years and 49 (1.1%) for 5 years. Only 29 patients (0.7%) were FAs over the 6-year follow-up period. The change in the number of individual FAs in 2001 to 2006 is presented in Table 1. Female FAs outnumbered male FAs throughout the study period. On average, 35% (range 32.6%-37.3%) were male and 65% (range 62.7%-67.3%) were female FAs, and the proportions remained the same throughout the study years.
Individual Frequent Attenders by Number of the Years Frequent Attendance Persisted in 2001 to 2006.
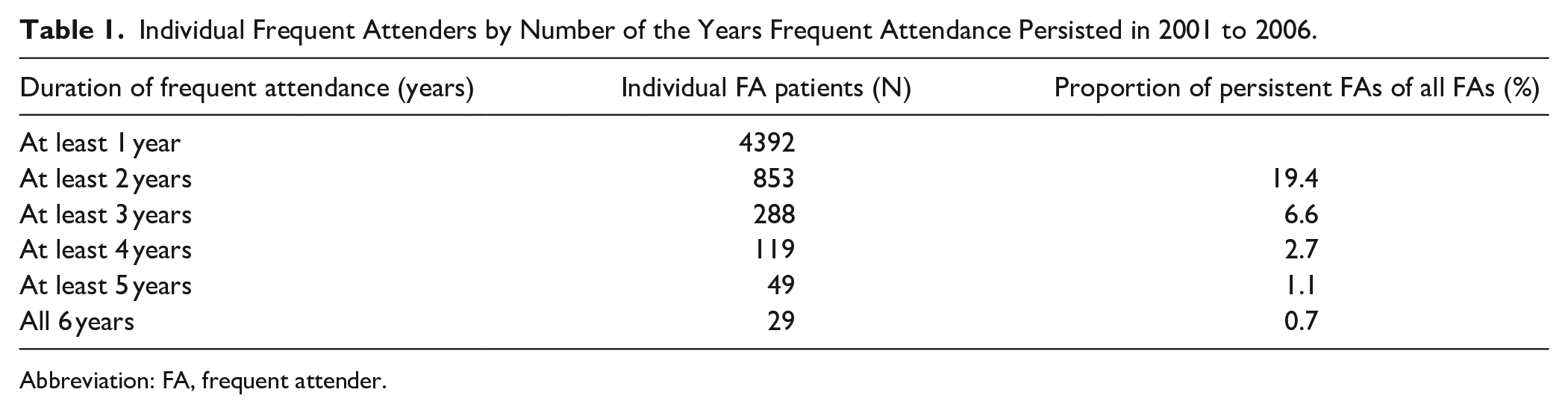
Abbreviation: FA, frequent attender.
In the study group there were 37 females and 12 males. Their average age was 51.7 years when the 2 children aged 5 years were included. The average age of males was 48.5 (SD 13.6) years and among females 55.4 (SD 17.2) years. Their background variables were recorded inadequately. There was no entry regarding occupation or education for 31.9% of the adults. The use of alcohol, smoking habits, and BMI were also poorly recorded. All background variables are listed in Table 2.
Background Variables of 47 5-Year Adult pFAs.

Abbreviations: BMI, body mass index; pFAs, persistent frequent attenders.
The adults in the study group had, on average, 15.3 (SD 3.1) self-initiated visits to a GP every year (range 11-30 visits). They were referred for secondary care, on average, 20.1 (SD 11.0) times per person (range 4-51 times) during the 5-year period. The mean number of different diagnoses in the adult study group was 21.2 (SD 5.3) per person (range 10-32).
In the adult study group versus the control group, there were statistically significantly more depressive episodes (P = .004), epilepsy (P = .035), heart failure (P = .019), asthma (P = .032); chronic obstructive pulmonary disease (COPD), including acute lower respiratory infections, other specified and unspecified COPD (P = .036); and recurrent lower back pain, lumbago, and unspecified dorsalgia (P = .046; Table 3). There were no differences in the occurrence of fibromyalgia, somatization, irritable colon or personality disorders, but this may have been due to the small number of these diagnoses.
Long-Lasting Symptoms or Chronic Diseases Diagnosis of 5-Year Adult pFAs and Controls.

Abbreviations: CI, confidence interval; FAs, frequent attenders; ICD-10, WHO international statistical classification of diseases and related health problems 10th revision; OR, odds ratio; pFAs, persistent frequent attenders.
In the text analysis, there were, on average, 79.5 words per patient entry in the study group; in the control group, this figure was 78.9. The most frequent words in the study group’s patient record entries were related to lung and breathing issues (“COPD,” “asthma”) and medications. In the control group’s patient record entries the most frequent words were related to various laboratory tests. GPs used very ordinary words for their 5-year FAs, with the most common words in patient entries being: “general state,” “40 mg,” “times per day,” and “mg per pill.” Phrases such as “nothing special,” “no fever,” “during 1 week,” and “nothing by auscultation” were also frequently used. In the 1-year FA control group, patient entries consisted of phrases like “male who had,” “-year-old male,” “during the year,” “during the month,” “ml,” “patient not,” and “female who had.” Gender was mentioned more often in the control group’s patient entries, but no statistical difference was found.
Discussion
Summary of Main Findings
The main findings of this study are as follows: (1) Incidence of pFAs, defined as FAs who continued frequent attendance for 3 years, was 6.6% and for 5 years was 1.1%. (2) pFAs were more often females than males (65% vs 35%), and they were middle-aged (51.7 years). The background variables concerning health habits were poorly recorded, and it was not possible to reliably identify the features of 5-year pFAs. (3) The following long-lasting symptoms and chronic diseases were statistically more common among 5-year adult pFAs than among 1-year adult FAs: asthma, COPD, depressive episodes, epilepsy, heart failure, and recurrent lower back pain/lumbago. (4) GPs and nurses used ordinary words when making entries into pFAs’ medical records. Therefore, it was not possible to differentiate 5-year pFAs from 1-year FAs in this way.
Comparison with the Current Literature
We found that most pFAs were female (65%). Koskela 4 and also Pymont and Butterworth 15 found that the female gender predicts persistent frequent attendance, which is consistent with our findings.
The number of pFAs approached 0 during the 6-year follow up time of our study. This agrees with Carney et al, 5 who found that most FAs returned to the normal consulting habit within 5 years.
Almost half (47%) of the 5-year adult pFAs made appointments with their GPs for recurrent back pain. To the best of our knowledge, this has not been reported in previous studies. Whether this relates to the diagnostic criteria used or to other reasons, such as differences in the culture of recording symptoms or to the diagnosis related to lower back pain, cannot be ascertained from the present data.
In contrast to our study, Koskela 4 did not identify that chronic diseases predict persistent frequent attendance, but his cohort consisted of patients younger than 65 years, with a very homogenous set of chronic disease diagnoses. Consistent with our findings, Carney et al 5 and Smits et al 6 reported that chronic psychiatric problems and chronic somatic diseases are an important contributor to persistent frequent attendance. In our pFA study group, there were moderate or heavy users of alcohol; in contrast Koskela 4 reported that abstinence predicted persistent frequent attendance. In a Danish study and in the study of Smits et al in pFA patient group there were persons who used alcohol over the recommended level.6,9 Smits et al 11 found that panic disorder, other anxiety disorders, negative life events, illness behavior, and lack of mastery were associated with persistent frequent attendance. We could not confirm these findings in our study by performing statistical word analysis. Like Patel et al 10 and Smits et al, 11 we found that pFAs often had long-lasting mental conditions (especially depressive episodes) and persistent physical diseases.
Reho et al 16 reported that musculoskeletal disorders are associated with persistent frequent attendance of working-age FAs. This agrees with our finding that the average age of the 5-year pFAs was 51.7 years and no <47% had recurrent back pain or lumbago.
Strengths and Limitations
The primary strength of this study is that we obtained data directly from electronic patient records; hence, we analyzed the actual patient entries. The size of our FA-cohort was substantial (4392 patients). Even though the 5-year pFA study group was quite small all their patient entries were analyzed, and their profiles were based on analysis of 10 056 electronic patient record pages. Statistically, we found some chronic diagnoses or long-lasting symptoms of pFAs, which could help to recognize them better. The text analysis considered almost 20 000 anonymized electronic patient entry pages. There were no organizational changes in the Finnish health care system between 2001 and 2020 that could have affected the number of FAs. Moreover, the legal basis of the electronic patient recording has not been changed either. Our previous study verified that frequent attendance as a phenomenon is very stable in the study city.
The size of the study group may constitute a limit of this study. Our data were probably insufficient to establish a reliable model to predict patients who might become pFAs. Another reason may be that GPs used such general words in the patient entries that those words did not differentiate pFAs. The health behavior habits of pFAs also were documented quite poorly in the electronic patient records; hence, we could not compare our findings with other studies or establish new features of pFAs. We did find some suggestions that being overweight could be a characteristic feature of pFAs (BMI > 30), but our data were not sufficient to establish this. Occupation was recorded in 68% of the patients, and half were retired despite an average age of only 51.7 years. Thus, persistent frequent attendance may be associated with work incapacity.
We also performed statistical analysis of the words in electronic patient entries of 5-year pFAs. There were some differences between the patient entry data of pFAs and 1-year FAs, but we were unable to identify specific words that could clearly help GPs or nurses in recognizing pFAs.
Conclusions
In primary healthcare persistent frequent attenders are a notable patient group. However, GPs described their pFAs using unexceptional words. It appears to be difficult to find information or even diagnoses from the electronic patient record narratives of pFAs. Thus, entries need to be more comprehensive and an electronic patient record system should be able to help GPs to identify pFAs better than today. Text mining and analysis procedures may be worthwhile to develop, but they need large data sets and comprehensive records.
More research is needed so that an easy and reliable algorithm can be developed for recognizing primary care patients at risk of becoming pFAs. The results of previous studies and the present study suggest that female gender, middle age (approximately 55 years), chronic diseases or long-lasting symptoms, especially depressive episodes, asthma, COPD, heart failure, and lower back pain are features linked to persistent frequent attendance. When patients with these characteristics consult a GP, it might be reasonable to spend some time with them and construct a treatment plan together, register it in the electronic patient entry, and follow-up on the visit frequency of the patient.
Footnotes
Acknowledgements
We thank Virpi Rantanen (MD, PhD adjunct professor in Obstetrics and Gynaecology at University of Turku) for her help in conducting the literature review.
Authors’ Contributions
AKS collected the data and drafted the manuscript. AS, SL, TV, HM, SS, and PR participated in the conception and design of the research and revised the manuscript for intellectual content. TV and HM performed the statistical analyses. All authors have read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Turku City Healthcare Centre in 2009 and 2010. Funding was also provided by the funding of the Finnish Government for University Level Health Research in 2019.
Ethics Approval and Consent to Participate
Finnish law does not require ethics committee review for registry-based studies; as this is a retrospective registry study, ethics approval was not required.
Consent for Publication
The medical record data used in this research were obtained with permission from the Health and Social Services of Turku. This authority also evaluated the legality of providing and using the data in accordance with the law. The use of register data is possible after the data keeping organizations have authorized the use of their data.The legal basis for processing personal data for public interest and scientific research is the EU General Data Protection Regulation 2016/679 (GDPR), Article 6(1)(e), and Article 9(2)(j); Data Protection Act, Sections 4 and 6.
Availability of Data and Material
The data that support the findings of this study are available from the Health and Social Services of Turku, but restrictions apply to the availability of these data, which were used under license for the current study. They are not publicly available. Data are, however, available from the authors on reasonable request and with permission granted by the Health and Social Service of Turku.