
Abstract
Introduction/objectives
Aging brings deterioration in many organs involving in swallowing, such as, oropharyngeal muscle weakness, decreased salivation, multiple teeth loss, decreased oral sensation, and delayed swallowing response. There are no official statistics and systematic records of swallowing problems in Thailand’s healthy elder populations. Therefore, this study aimed to determine the prevalence of swallowing problems among a Thai healthy elder population.
Methods
A survey of 874 elders was conducted at Community Hospitals in region 7 of the Thai National Health Security Office from September to November 2019. All participants were interviewed using a questionnaire focused on, screening for swallowing problems using a 10-item Eating Assessment Tool (EAT-10) and questions about participants’ physical and oral health behaviors.
Results
Sixty-six percent of the participants were women and 34% were males, with mean age 69.70 ± 6.79 years. Of these, 11.4% had swallowing problems. The most common swallowing problems were food sticking in the throat, effort on swallowing and choking. Age and having an underlying disease were found to be statistically significantly associated with dysphagia, whereas gender was not associated with dysphagia.
Conclusions
The prevalence of swallowing problems among Thai healthy community-dwelling elders was assessed as about 11%. Early identification and early intervention for swallowing problem is necessary for promoting health and quality of life of our growing elderly population.
Introduction
Dysphagia or difficulty swallowing is a common condition in the elderly. Aging brings deterioration in many organs involving swallowing, such as oropharyngeal muscle weakness, decreased salivation, multiple teeth loss, decreased oral sensation, and delayed swallowing response.1-5 Furthermore, difficulty swallowing can also be a consequence of comorbidities such as cerebrovascular accident, Parkinson’s disease, dementia, and laryngeal or esophageal cancer. 6 Dysphagia in the elderly can cause aspiration of a bolus or saliva resulting in lower respiratory tract infections, such as pneumonia, lung abscesses, and mortality.6,7 Swallowing problems may also lead to malnutrition and dehydration causing poor physical status and quality of life
In a Spanish study, 69.6% of the elderly in nursing homes had difficulty swallowing, and 38% required to tube feeding because of this condition. 6 Madhavan et al 8 reviewed 15 studies regarding the swallowing disorder in elderly living in the community. They demonstrated that 5% to 72% of the community dwelling elder had swallowing difficulty. Prevalence of dysphagia among community dwelling elderly in Japan was 13.8%. 9 In Thailand, there are no official statistics or systematic records for swallowing problems in the healthy elder populations. Collecting this sort of data may lead to early resolution of these problems reducing severe consequences, enhancing rehabilitation effectiveness, and decreasing complications. Therefore, this study aimed to initiate a database on swallowing problems among healthy Thai community-dwelling elders to facilitate future planning for promotion, prevention, treatment, and rehabilitation of dysphagia in the elderly.
Material and Methods
This study was a cross-sectional questionnaire survey to investigate the swallowing status of 874 elderly individuals in region 7 of the Thai National Health Security Office (NHSO 7). NHSO 7 includes Kalasin, Khon Kaen, Maha Sarakham, and Roi Et Provinces in Northeastern Thailand. Data was collected at Community District Hospitals and Sub-district Health Promotion Hospitals from September to November 2019.
The sample size was calculated by estimating a finite population proportion formula. The proportion of the elderly, who had difficulty swallowing (40%) 10 at a confidence level of 95%, was based on the population in NHSO 7, aged 60 years and over. The population data was obtained from the Thai Health Data Center on December 11, 2018, and showed there were 712,717 elderly individuals in NHSO 7. Therefore, a minimum sample size of 738 people was required, and the data was collected in proportion to the population of each province.
Multi-stage Random Sampling was conducted in all 4 provinces. A number of districts were randomly selected in each province based on the province population. In Khon Kaen Province, 6 districts were involved: Nam Phong, Ban Fang, Muang, Sam Sung, Phu Wiang, and Nong Ruea. In Roi Et Province, 4 districts were involved: Muang, Phon Thong, Suvarnabhumi, and Phanomprai. In Maha Sarakham Province, 3 districts were involved: Kantarawichai, Yang Si Surat, and Wapi Pathum. In Kalasin, 3 districts were involved: Kamalasai, Kuchinarai, and Huai Mek. In each district, 2 sub-districts were randomly selected and 25 elderly individuals, who were receiving services at each sampling Sub-district Health Promotion Hospital, were recruited for the study.
The inclusion criteria were persons who were 60 years of age or over, able to live independently and who had been receiving services at the Community Hospital, or, the sub-district Health Promotion Hospitals in the survey areas. Individuals who could not speak Thai, or, Isan, or who had a history of neurological disease such as stroke, Parkinson, dementia, or head and neck cancer which affected swallowing were excluded.
All participants were interviewed using a 2 parts questionnaire. Part 1 was the 10-item Eating Assessment Tool (EAT-10), 11 which was used to screen for oropharyngeal dysphagia. It consists of 10 questions with a total score of 40 points. If EAT-10 score of 3 or more was obtained, the participant was categorized as having a swallowing problem. The internal consistency of the EAT-10 is 0.960, whereas the test-retest intra-item correlation coefficients is from 0.72 to 0.91. 11 Part 2 of the questionnaire consisted of questions about the physical and oral health behaviors of the participants such as underlying disease, denture wearing, and regular tooth brushing.
Data analysis was carried out by using the software program SPSS version 17, and the data was presented in descriptive statistics with percentages, means, standard deviations, medians, and minimum-maximum range. The Chi-square test/Fisher Exact probability test was used to assess for correlations between the factors affecting dysphagia.
This research was reviewed and approved by the Human Research Ethics Committee of the Department of Health of the Thai Ministry of Public Health (Research project code 335, 26 August 2019).
Results
The majority of the 874 participants were female (66.2%), while 33.8% were male. The ages ranged from 60 to 100 years (mean age 69.70 ± 6.79 years). In addition, 47.7% had a medical history of hypertension and diabetes (Table 1). The proportions recruited from each province were, from Khon Kaen (37.5%), Roi Et (25%), Mahasarakham (19.3%), and Kalasin (18.2%).
Demographic Data (n = 874).

It was found that 11.4% (100/874) of the elderly had likely swallowing problems. The top 3 statements selected in the interviews were: (1) “When I swallowed food, it felt like I had food stuck in my throat.” (2) “I have to make more effort than usual to swallow food.” and (3) “I cough when swallowing food.” (Table 2).
Number of Responders for Each Item of EAT-10.

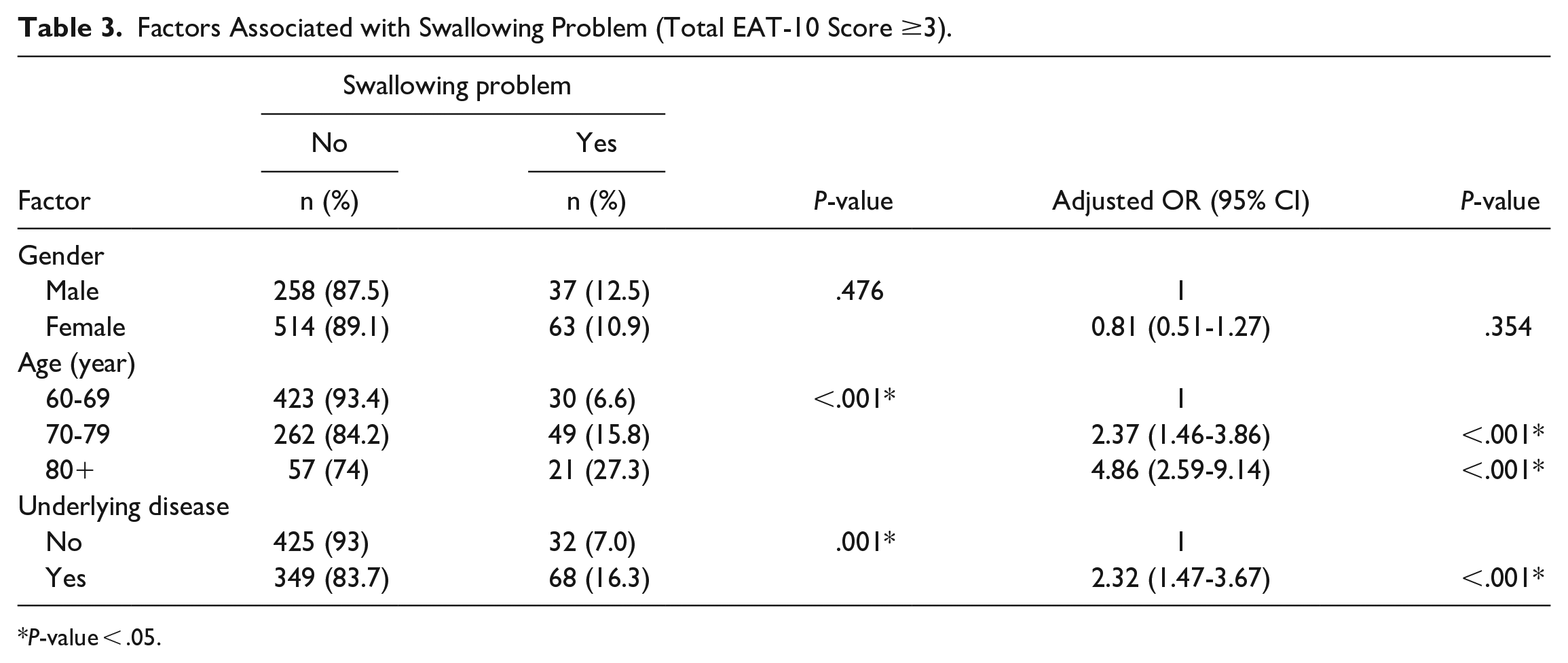
Correlations between personal factors and the dysphagia revealed that gender was not associated with dysphagia, but age and having an underlying disease were statistically significantly associated with dysphagia (Table 3). However, there was no statistically significant association between having swallowing problem and hypertension (P-value = .783), diabetes (P-value = .594), dyslipidemia (P-value = .347), heart disease (P-value = .191), and cancer (P-value = 1.00). Moreover, no statistically significant association between swallow problem and denture wearing was detected (P-value = .328).
Factors Associated with Swallowing Problem (Total EAT-10 Score ≥3).
P-value < .05.
Discussion
To the best of our knowledge, this survey was the first intended to determine swallowing problem prevalence among the well community-dwelling elderly in Thailand. Although swallowing problems are a common problem leading to insufficient food and fluid intake and aspiration pneumonia, the epidemiology of swallowing conditions among healthy elders is scarcely reported. The findings of this study revealed that 11.4% of the participants had swallowing problems. Whereas, a previous study 12 using subjective questionnaire that found 16% of their 977 subjects had dysphagia. Likewise, Madhavan et al 8 reported that estimated prevalence of swallowing disorder among 6 high quality studies was 15%. Further, Roy et al 13 found 37.6% of community living elder had swallowing problems during their lifetime. The lower prevalence in our study than previous studies,8,9,12,14,15 may have been due to elders who had chronic disease such as stroke or cancer being excluded from our this study. The average age in this study was also lower than in other studies, and the swallowing screening tool for each study was different. However, an Australian study has reported similar findings, with 11.4% of their healthy elderly having swallowing problem. 16
We also found similar correlations between age and having underlying disease with dysphagia as previous studies.13,16,17 Physical changes in aging, reduction in tongue strength, decreased oral sensation, delayed swallowing reflex, poor hyolaryngeal elevation, loss of teeth, and loss of tissue elasticity together with underlying disease may result in swallowing problems.1,5,18 The prevalence of swallowing disorders is increasing with an increasingly aging population. Advancing age increases susceptibility for medical conditions such as stroke, neurodegenerative disease, and head and neck cancer, and such medical conditions may contribute to dysphagia. Previous studies19,20 have reported a gendered effect on swallowing function with females having a longer oropharyngeal transit duration, pharyngeal clearance, and upper esophageal sphincter duration than male. However, there was no correlation between gender and dysphagia in the present study, similar to the study of Abdul Khader and Mubeena. 15
The present study showed that top 3 problems the elderly complained of in the interview were: (1) “When I swallowed food, it felt like I had food stuck in my throat.” (2) “I have to make more effort than usual to swallow food.” and (3) “I cough when swallowing food.” Similarly, Khader reported the common swallowing problems among elderly were “Difficulty in swallowing solid food” and “Feeling of lump of food stuck in throat.” These problems were caused by age-related changes in pharyngeal phase; reduced hyolaryngeal elevation, weakness or poor coordination of the pharyngeal muscle, and impairment in the opening of the upper esophageal sphincter.5,18 Consequently, some food residue remains in the pharynx post swallowing, and elders feel like food stuck in the throat, have difficulty swallowing and a higher risk of aspiration.
Despite, elders reporting swallowing problems, none of them had sought healthcare professional help. Most of them overlooked the swallowing problem, accepting it as an inevitable part of advancing age. However, dysphagia can affect quality of life in both patients and the general population. Patients with swallowing problems, especially the elderly, are at risk of malnutrition and susceptible to respiratory infections. Due to the aging-related weakness, the elderly should be assessed for primary swallowing conditions in order to determine the causes and provide early management. Knowledge regarding swallowing disorders including complication prevention should be introduced to elderly to reduce the risk of aspiration, the development of possible complications, and support a better quality of life. In turn, this could also reduce mortality rates and medical expenses.
Clinical evaluation of swallowing could not be done in this study, so there was no confirmatory evidence for swallowing disorder, nor was swallowing pathology and physiology identified.
The prevalence of swallowing problems among Thai healthy community-dwelling elders was assessed as about 11%. As this study was conducted only among healthy elders who visited the Sub-district Health Promotion Hospitals the full magnitude of problem in the community may be underestimated. Swallowing disorders have a negative effect on health and quality of life, so early identification early intervention is necessary for lifestyle support for elderly persons.
Footnotes
Acknowledgements
The authors would like to thank dentists and dental health staff from NHSO 7 office for data collection. We would also like to acknowledge Professor John F. Smith for English editing the manuscript via the Publication Clinic of Khon Kaen University, Thailand.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Regional Health Promotion Center 7 Khon Kaen, Department of Health, Ministry of Public Health.