
Abstract
Background:
Risk assessment criteria for predicting dengue outbreak must be appropriated at village levels. We aimed to develop risk dengue village prediction criteria, predict village dengue risk, and strengthen dengue prevention based on community participation.
Methods:
This participatory research conducted in Southern Thailand included the following 5 phases: (i) preparing communities in 3 districts; (ii) developing risk dengue village prediction criteria; (iii) applying computer program; (iv) predicting village dengue risk with 75 public health providers in 39 PCUs; and (v) utilizing findings to strengthen dengue prevention activities in 220 villages. Data collecting for prediction used secondary data from primary care units in the past 5 year and current year. Descriptive statistics used calculating criteria and comparing with standard level to adjust score of risk.
Results:
Risk dengue village assessment criteria had 2 aspects: dengue severity (3 factors) and dengue outbreak opportunity (3 factors). Total scores were 33 points and cut-off of 17 points for high and low dengue risks villages. All criteria were applied using computer program (http://surat.denguelim.com). Risk prediction involved stakeholder participation in 220 villages, and used for strengthening dengue prevention activities. The concept of integrated vector management included larval indices surveillance system, garbage management, larval indices level lower than the standard, community capacity activities for dengue prevention, and school-based dengue prevention. The risk prediction criteria and process mobilized villages for dengue prevention activities to decrease morbidity rate.
Conclusion:
Dengue risk assessment criteria were appropriated within the village, with its smallest unit, the household, included. The data can be utilized at village levels for evaluating dengue outbreak risks.
Keywords
Introduction
Dengue is burdensome in several tropical and sub-tropical countries. An estimated 50 million dengue infections occur annually, worldwide, and approximately 2.5 billion people live in dengue-endemic countries. Among them, 1.8 billion live in South-East Asia and Western Pacific regions, and 500 000 dengue cases require hospitalization yearly, with a death rate of 2.5%.1-3 The main risk factors of dengue include rainfall, temperature,4,5 mosquito density, 6 density of people,7,8 dengue types, 5 non-specific treatment,1,2 no effective dengue vaccine,5,9 ineffective drugs, 5 human immunity, 10 people’s movement across areas,11,12 population density, 13 attitude toward dengue prevention,14,15 and occupation. 12 Interventions to address dengue problems combine community mobilization, entomological methods, and chemical and biological controls. 16
In Thailand, the dengue-spread of over 60 years has no specific outbreak pattern because of the several dengue virus types involved at the same time. Further, frequent outbreaks occur in the middle and southern areas of Thailand. Future predictions are necessary to prevent dengue outbreaks. Several studies on predicting dengue outbreaks are based on disease surveillance, meteorological, and socio-economic data; others were on human activities, peoples’ movement patterns, 11 epidemiology (dengue incidence), and entomology (female adult dengue vector). 17 The Department of Disease Control, Thai Ministry of Public Health (Thai MoPH) 18 used the health risk assessment criteria (recurrent endemic area, severity of disease, morbidity rate in the current year) at district and sub-district levels (including disease severity based on recurrent endemic area and incidence rate; and outbreak factors including population movement, population density, and community participation strengthening). 19 However, since these criteria excluded households in the villages, evaluation of the criteria to strengthen community participation was unclear.
A prediction report used only epidemiological data (number of dengue patients), focusing on dengue risk districts. 18 However, this report included only dengue risk areas at district level, but excluded prediction by larval indices, and approach to strengthening village activities was unclear. Community activities decrease the dengue burden 16 and alert people on dengue prevention approach including household larval indices survey. The classical larval indices included House Index (HI; percentage of houses infested with larvae; HI<10), Breteau Index (BI; number of positive containers per 100 houses inspected; BI<50), and Container Index (CI; percentage of water-holding containers infested with larvae; CI<1), and morbidity rate.1,20 Larval indices surveys, used to assess the community capacity for dengue prevention,5,21 are practical, low cost, convenient, help prevent dengue, and are used to evaluate dengue outcomes.22,23 Dengue risk prediction should include village activities (households and schools) and the larval indices surveillance system (LISS) as an innovative solution for dengue outbreak.
The Surat Thani Province, one of the provinces in Southern Thailand, has a higher infection rate than the Thai MoPH standard (<50 cases/100 000 population) with dengue incidence rates from 2013 to 2017 of 125, 154, 64, 51, and 92 cases/100 000 population, respectively. 24 Dengue outbreak trends from 2013 to 2017 show no specific pattern, but often develop rapidly, are difficult or impossible to predict, and cause a disproportionately high burden. Thus, we aimed to develop dengue risk village assessment criteria and predict dengue risk village based on community participation and strengthen dengue prevention in high- and low-dengue risk villages among 220 villages and 5 communities in Southern Thailand.
Methods
The study was approved by the Institutional Review Board (IRB), the Ethical Review Committee for Research Subjects, and the Health Science Group of Walailak University, Thailand (approval number WUEC-16-059-01 and WUEC-19-048-01). This community participatory action research (CPAR) that was conducted from August 2017 to April 2020, predicted dengue risk every January, and was divided into 5 phases: (i) preparing the community, (ii) developing assessment criteria for assessing dengue risk village, (iii) application of a computer program (http://surat.denguelim.com), (iv) predicting dengue risk villages, and (v) utilising the findings for village dengue prevention.
Preparing the Community
Surat Thani Province, the largest of the southern Thailand provinces, has 19 districts, with 131 sub-districts and 1028 villages. The research setting focused on the health network of the 220 villages where dengue outbreaks were addressed, including 3 districts such as Kanchanadit, Ban Ta Khun, and Phra Saeng Districts with 117, 29, and 74 villages, respectively. Three districts were higher dengue morbidity rate (2013-2017) than other 19 districts in the province. Kanchanadit District was morbidity rate from 2013 to 2017 of 214.65, 70.14, 106.29, 58.46, and 156.26 cases/100 000 population; Ban Ta Khun District was morbidity rate from 2013 to 2017 of 180.06. 37.92, 75.55, 56.41, and 87.76 cases/100 000 population, and Phra Saeng District was morbidity rate from 2013 to 2017 of 122.78, 5.93, 17.61, 18.99, and 23.29 cases/100 000 population, respectively. 24 Stakeholders who involved dengue prevention of village, local administrative organization (LAO), public health provider (PHP), community leaders in villages, all village health volunteer (VHV), heads of hospital, and the village integrated vector management for households and community were mobilized; the study objectives were provided to stakeholders, and informed consent was obtained from the participants for data collection and activity participation. The research participating of 220 villages under each district management which involved were: 18, 7, 14 PCUs; 43, 10, and 22 public health providers; 2340, 480, and 1200 VHVs of Kanchanadit, Ban Ta Khun, and Phra Saeng Districts, respectively. PCUs were taking role of center of LISS at sub-districts of each district. The setting research showed at Figure 1.
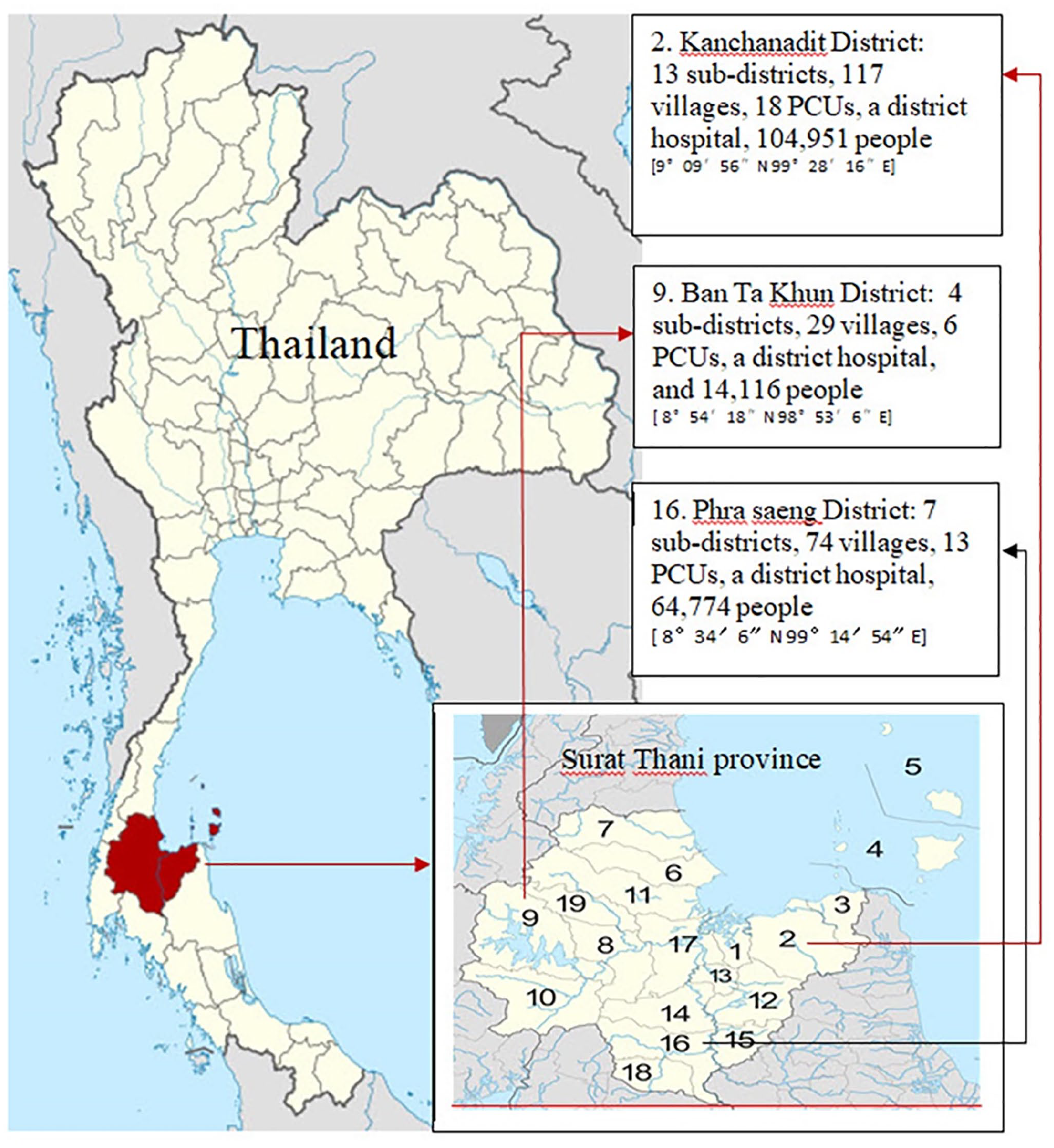
Two-hundred and twenty villages in 3 districts for predicting HRDV and LRDV.
The Development of the Risk Dengue Village Prediction Criteria
We developed risk dengue village prediction criteria by reviewing the literature on dengue risk assessment, dengue forecasting, and village dengue risk prediction using community participation. Risk refers to the occurrence of damage or unwanted situation, resulting in failure of specified objectives and goals. 19 Dengue outbreak risk assessment at the village level, including environmental assessment, was integrated into the district level dengue risk assessment criteria using particular district disease control manual according to the Department of Communicable Disease Control, Thai MoPH. 20
Application of the Computer Program (http://surat.denguelim.com)
The computer program for supporting village dengue risk prediction was developed based on appropriate community context. The program uses web application relating disease severity factors in the past 5 years and outbreak opportunity factors. The program modules include dengue prevention responsibility in PCUs for district public health officials and administrators. The program is easy to use by public health officers and all stakeholders in the community. The advantages of the program include the ability to record, collect, and easily report data to predict village dengue outbreak risk quickly and the potential for several dimensions of presentation at village, PCU, and district levels.
The developed program works by assessing and analyzing the needs of all stakeholders in the community and designing web application based-on Windows operation system. The developed operation system of the application uses services such as MySQL Database 5.5 for the database management system, Apache Web Server, and PHP 5.6 Scripting Language; testing system; document guide for use, and setting system and use program. The result showed that the program used by client/server architectural system is based-on the Windows operation system. For full report of the program, the user must set up the program browsers such as internet explorer or Google Chrome (Supplemental Materials 1 and 2).
Predicting High- and Low-Risk Dengue Village
From literature reviewed, the CDC, 18 and Bureau of Knowledge Management in Department of Disease Control, Thai Ministry of Public Health 19 presented the prediction criteria cut-off point 3 scale, but it was criteria in district, and sub-district level. For dengue risk village prediction, the study “Developing the active larval indices surveillance system for dengue solution in low and high dengue risk primary care units, Southern Thailand” used haft scale for setting cut-off point of high and low risk level (14 of 28 points) which successfully strengthen dengue prevention activities in the villages. 25 However, this study was developing criteria based on community activities for dengue solution changing the cut-off point high and low level were 17 of 33 points.
For predicting risk dengue village, community meeting of all district stakeholders related to dengue prevention was conducted with 43, 10, and 22 public health providers who representative from 18, 7, and 14 PCUs of Kanchanadit, Ban Ta Khun, and Phra Saeng Districts, respectively. The researcher informed of the objectives, utilities of prediction of village dengue risk and its principle, method of prediction, main data for calculation, criteria, and use of the computer program (http://surat.denguelim.com). The public health officer prepares relevant data for the computer program to strengthen the community prevention program. Furthermore, dengue morbidity and mortality rates, as well as the total population in each district were comprehensively searched. All stakeholders participated in the assessment of villages with low and high dengue risks, using half of the total score (17 of 33 points) from disease severity and outbreak opportunity factors. The risk values from the cut-off point were categorized into 2 levels, using the total risk cut-off points ≥17 (HRDV) and <17 (LRDV).
Using Prediction Results for Strengthening Village Dengue Prevention Activities
The data processed by the computer program, were shown as high and low dengue risks. The prediction was conducted between January 2019 and January 2020. Thereafter, the stakeholders considered activities for strengthening community dengue prevention involved larval indices surveillance system, garbage management, community capacity activities, and school-based dengue prevention. This phase needs participating of public health provider of PCUs, VHV, and stakeholders following CPAR approach.
Results
Risk Dengue Village Prediction Criteria (RDVPC)
The prediction criteria for village dengue risk involved 2 aspects consisting of 6 factors; disease severity aspect (3 factors) and outbreak opportunity aspect (3 factors) which integrated epidemiology, entomology, and community activities.
1. Dengue severity aspect (DSA).
1.1 Endemic village factor (EVF) was based on the village dengue incidence rate in the previous 5 years. This criterion showed several factors of dengue incidence. The weight of the value assigned to an endemic village showed that the more the number of years of dengue incidence reporting, the higher the points. For example, a village with a weight value of 3 points had dengue incidence in 3 out of 5 years.
1.2 Dengue herd immunity factor (DHIF) refers to the average morbidity rate in the previous 5 years. According to the natural course of dengue infection, the immune system is the body’s primary defence against the virus. When someone is infected with dengue, the innate and adaptive immune responses together fight the virus. The B cells produce antibodies that specifically recognize and neutralize the foreign viral particles, and cytotoxic T cells recognize and kill infected cells with dengue virus. People who are infected subsequently with a different dengue virus type may experience “antibody-dependent enhancement,” a condition that occurs when the immune response worsens dengue clinical symptoms, increasing the risk of severe dengue. 10 Antibody-dependent enhancement of dengue infection assumes a level of immunity in the community showing that the higher the outbreaks in the area, the higher is the herd immunity, compared to low level outbreak areas. Therefore, areas with high dengue risk in the past 5 years should have low outbreak in the following year. 19 For example, a weight value point in risk in a village corresponds to an average morbidity rate in 5 years of more than 200/100 000 population.
1.3 Current morbidity rate factor (CMRF) indicates the past 5-year median rate. According to the dengue outbreak based on dengue virus serotypes and the immunology in the risk area, with a low dengue incidence rate, in the following year, the area is at high-risk of an outbreak. When the current morbidity rate is less than the past 5-year median morbidity rate, the area is at high-risk of dengue outbreak. For example, the weighting risk factor value is 5 points in a village with a current morbidity rate less than the past 5-year median morbidity rate (−50%).
2. Dengue outbreak opportunity aspect (DOOA).
2.1 Population movement factor (PMF) includes factors related to tourists and/or industrial areas where movement can enhance dengue virus transmission. Movement patterns of people and spatial heterogeneity of human activities influence dengue outbreak. 11 A study devised 3 levels of risk values for villages. 19 Then, this study, gave score 3 point for a village which had “high population movements in a village with camp workers, factories, students studying outside the area, petrol stations, shops, prisons, parks, large schools, and markets,” 2 point for moderate movement of people in the village such tourist place, and a point for the village that low movement population.
2.2 Population density in village factor (PDVF) indicates the number of people per square kilometre. This model of human population density predicted dengue outbreak8,26 because dengue virus transmission occurs between humans and mosquitoes. High population density is associated with increasing dengue incidence.13,27 A study on dengue risk assessment criteria used the population density at 5 levels. 19 A village with “very high population density (>16 400 cases/km2)” or “very low population density (<5601 cases/km2)” received 5 and 1 point, respectively, of weight value of risk.
2.3 Strengthening villages for dengue prevention activities (SVDPA) includes activities, project, or interventions for dengue prevention in participating villages. Intervention trials should measure the impact on dengue risk. 16 Five main activities related to village strengthening include:
2.3.1 Larval indices surveillance system (LISS), which collecting, analyzing, interpreting, feedback, and use of data for dengue prevention activities in a village, to show the pattern of the larval indices from households to districts. 28 For a completed system, partially conducted, or unclear and no appearance; the scores were 0, 1, and 2 points, respectively.
2.3.2 Garbage management in households and communities because most water containers with larval infestation are found outside, in household garbage. Particularly, porcelain and plastic wastes are more conducive for Ae. aegypti reproduction. 29 Such garbage management system should reuse, recycle, and reduce. For a completed project, partially conducted, or unclear and no appearance; the scores were 0, 1, and 2 points, respectively.
2.3.3 Larval indices lower than the standard level (BI < 50, HI < 10, and CI < 1). For village larval indices value of 3 points lower than the standard level, dengue outbreak depends less on mosquito density than on environmental temperature. 11 Entomological indices are used to measure dengue vector infestation in and around structures (such as, homes and buildings). However, these indices are seldom sensitive to precisely estimate dengue transmission risk or predict impending outbreaks.6,19,30 The values were lower than the standard mean of the larval indices levels in March and August as reported by the Thai MoPH (BI < 50, HI < 10, CI < 1). We estimated the larval indices at 3 levels as follows: “3 larval indices lower than the standard value = 0 points,” “1 or 2 of 3 larval indices lower than the standard value = 1 point,” and “3 larval indices higher than the standard values = 2 points.”
2.3.4 Community capacities activities refer to the village member activities for increasing the capacity for sustainable dengue prevention, at least 1 project per village. In an intervention study for dengue prevention 22 there were 3 values for the activities for enhancing community capacity for disease prevention. For a completed project, partially conducted, or unclear and no appearance; the scores were 0, 1, and 2 points, respectively.
2.3.5 School-based dengue prevention activities refer to dengue prevention activities taking place in schools, conducted by teachers, students, and stakeholders. Schoolchildren have high incidence rate of dengue infection as a “sentinel population,” 26 and the school is a high-risk area. The larval indices criteria for schools, CI = 0. For schools in a village where children learn either a full dengue prevention project, partially conducted, or unclear and none had the scores of 0, 1, and 2 points, respectively.
The total weight value of community participation according to the 5 main community participation activities to assess the village dengue risk was 10 points.
The RDVPC consisted of DSA (3 factors) and DOOA (3 factors) are also shown in Table 1.
Risk Dengue Village Prediction Criteria (RDVPC) Consisted of 2 Aspects and 6 Factors.
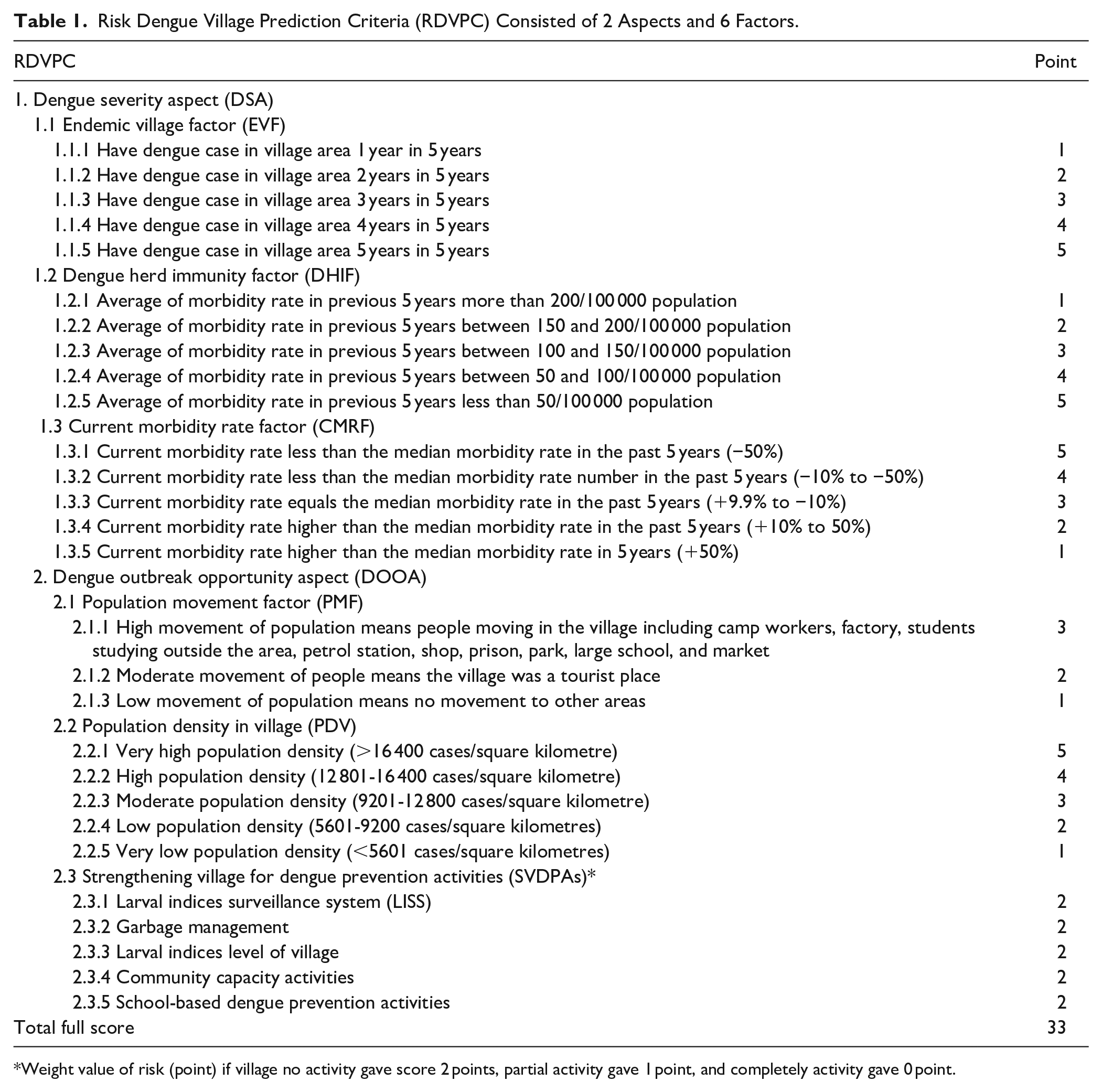
Weight value of risk (point) if village no activity gave score 2 points, partial activity gave 1 point, and completely activity gave 0 point.
HRDV and LRDV in 3 Districts
The results showed HRDV and LRDV using CPAR of 220 villages in 3 districts of Surat Thani Province, Southern Thailand.
Kanchanadit District, Surat Thani Province, with 117 villages in 13 sub-districts, a district public health officer, and 18 PCUs, was a high dengue risk district. Based on RDVPC and CPAR, the district predicted risk dengue villages for the 2019 prediction using the past 5-year (2013-2017) dengue morbidity rates for the 5 previous years (2013-2017) and the current (2018) prediction. The health leaders at the Kanchanadit District health network participated in dengue risk village assessment. The total number (percentage) of HRDV and LRDV were 71 (60.68%) and 46 (39.32%), respectively. The 2020 prediction used the past 5-year dengue morbidity rate (2014-2018) and the current (2019) of dengue risk village showed a number (percentage) of HRDV and increasing LRDV, 50 (42.74%) and 67 (57.26%), respectively. The program (https://surat.denguelim.com) showed the comparing percentage of HRDV and LRDV in 18 PCUs (Figure 2a and b).

High-and low-dengue risk villages at Kanchanadit District in 2019 (a) and 2020 (b) based on the 18 PCUs in the district.
Ban Ta Khun District has 29 villages for dengue risk prediction. Virtually none of the villages showed any of the 5 activities for community strengthening of dengue prevention. They especially did not participate in the LISS and dengue project in each village. For the 2019 prediction, all villages used the past 5-year (2013-2017) dengue morbidity rates for the 5 previous years (2013-2017) and the current (2018) prediction. The total number (percentage) of HRDV and LRDV in 2019 were 22 (75.86%) and 7 (24.14%), respectively. The 2020 prediction used the past 5-year dengue morbidity rate (2014-2018) and the current (2019) showed a decreasing number (percentage) of HRDV and increasing LRDV, 10 (34.48%) and 19 (65.52%), respectively. The program (https://surat.denguelim.com) showed the comparing percentage of HRDV and LRDV in 7 PCUs (Figure 3a and b).

High-and low-dengue risk villages at Ban Ta Khun District in 2019 (a) and 2020 (b) based on the 7 PCUs in the district.
The Phra Saeng District in the Surat Thani Province, has 74 villages in 8 sub-districts. The district has 14 PCUs that participated as leaders for the district’s dengue prevention. Based on RDVPC, the 2019 prediction used the past 5-year dengue morbidity rate and the current (2018). The number (percentage) of HRDV and LRDV were 34 (45.95%) and 40 (50.05%), respectively. The 2020 dengue risk village prediction used the past 5-year dengue morbidity rate (2014-2018) and the current (2019) showed a decreasing number (percentage) for HRDV and increasing LRDV, 24 (32.43%) and 51 (67.57%), respectively. The program (https://surat.denguelim.com) showed the comparing percentage of HRDV and LRDV in 14 PCUs (Figure 4a and b).
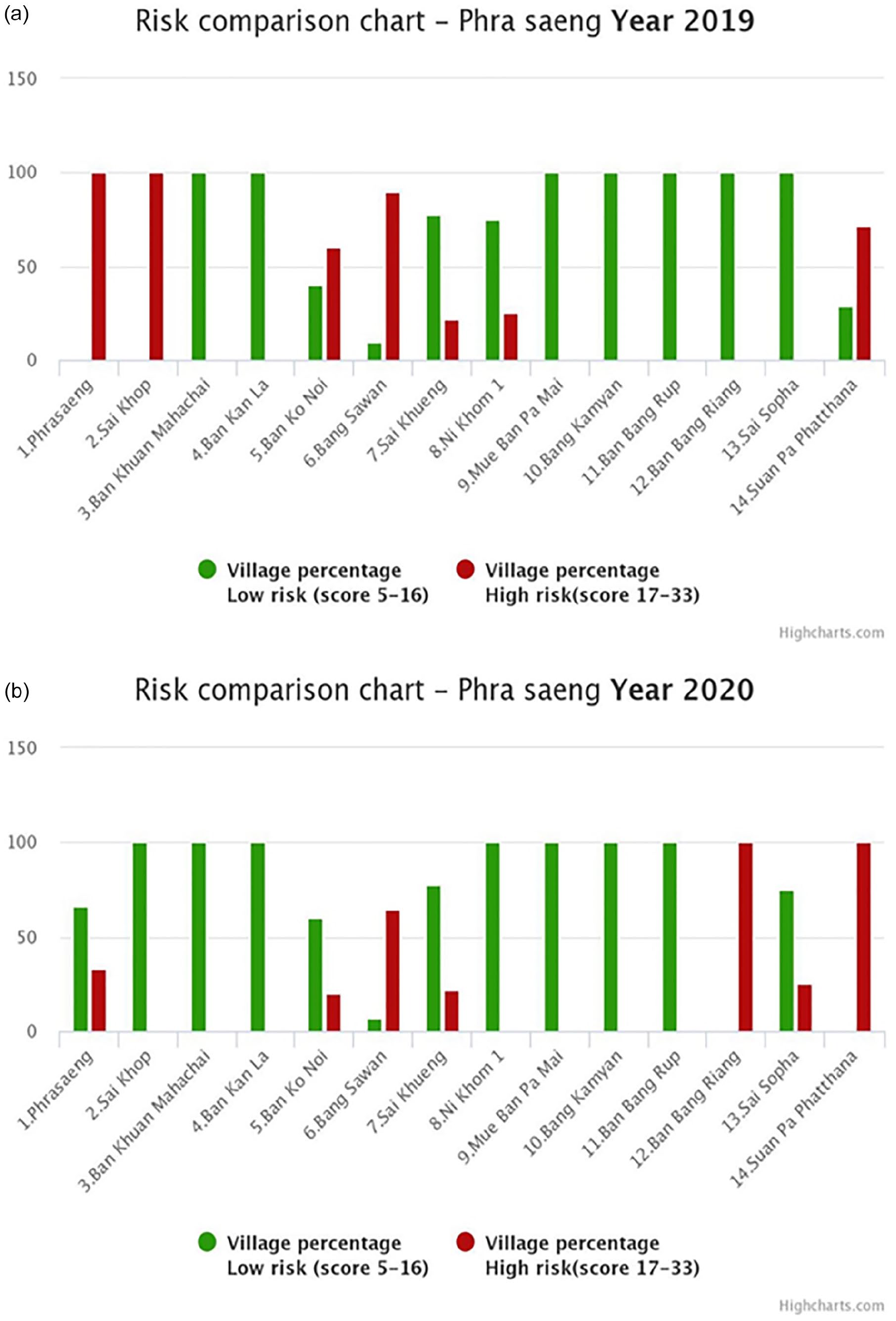
High-and low-dengue risk villages at Phra Saeng District in 2019 (a) and 2020 (b) based on the 14 PCUs in the district.
Strengthening Village for Dengue Prevention Activities (SVDPAs)
The 3 districts used the results for the villages’ dengue prevention activities. Village mobilizations were promoted based on the dengue risk village predictions. Public health officer and PCUs in the districts used the results of risk prediction to conduct all dengue prevention activities via community leader, village health volunteer (VHV), school, local administration government, and others.
Kanchanadit District, 43 public health providers who representative of 18 PCUs used the 2019 prediction results for strengthening the dengue prevention activities, based on the community estimations including LISS values in villages at 117 (100%); garbage management in villages, integrated with household and local government administrations at 50 (42.75%); for the level of village larval indices lower than the standard level (BI < 50, HI < 10, and CI < 1), at least two-thirds indices were 65 (55.56%); community capacity activities of village members to increase the capacity for sustainable dengue prevention by at least 1 project per village, which was 30 (25.64%); and school-based activities on dengue prevention in 52 schools conducted by teachers, students, and stakeholders occurred in 30 schools (57.69%). Additionally, dengue morbidity rate decreased in 2018, 2019, and 2020 at 175.56, and 64.71 cases/100 000 populations, respectively (Table 2).
Strengthening Dengue Prevention Activities in 3 Districts.
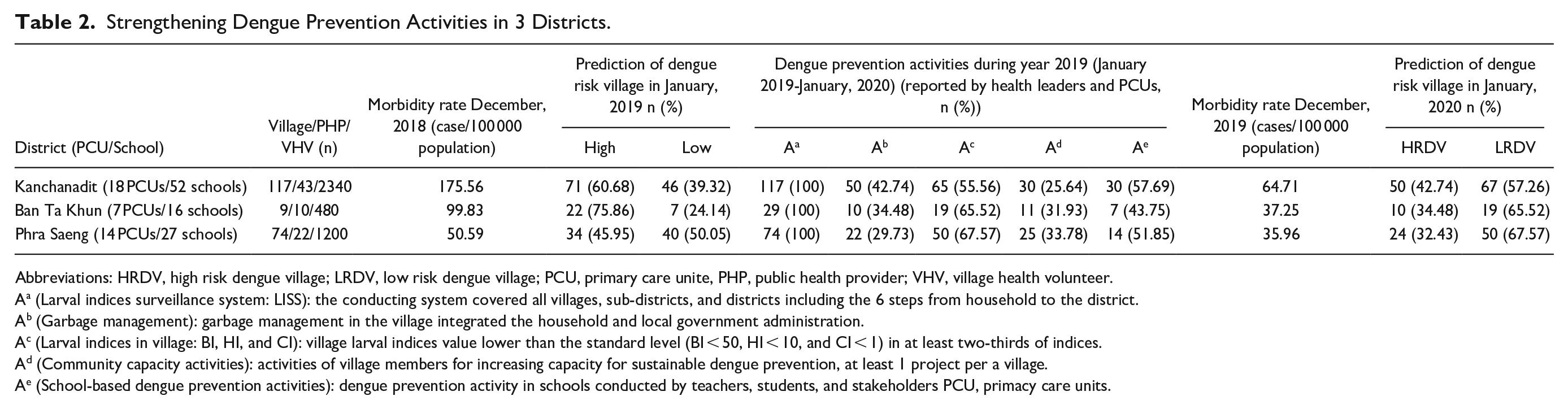
Abbreviations: HRDV, high risk dengue village; LRDV, low risk dengue village; PCU, primary care unite, PHP, public health provider; VHV, village health volunteer.
Aa (Larval indices surveillance system: LISS): the conducting system covered all villages, sub-districts, and districts including the 6 steps from household to the district.
Ab (Garbage management): garbage management in the village integrated the household and local government administration.
Ac (Larval indices in village: BI, HI, and CI): village larval indices value lower than the standard level (BI < 50, HI < 10, and CI < 1) in at least two-thirds of indices.
Ad (Community capacity activities): activities of village members for increasing capacity for sustainable dengue prevention, at least 1 project per a village.
Ae (School-based dengue prevention activities): dengue prevention activity in schools conducted by teachers, students, and stakeholders PCU, primacy care units.
The Ban Ta Khun District, 11 public health providers who involved dengue prevention of 7 PCUs used the results for village activities for strengthening village dengue prevention activities based on community estimates such as LISS value of 32 (100%); garbage management in villages, integrated with household and local government administrations at 10 (34.48%); for village larval indices levels lower than the standard (BI < 50, HI < 10, and CI < 1), at least two-thirds indices were 19 (65.52%); community capacity activities of village members to increase the capacity for sustainable dengue prevention by at least 1 project per village, which was 11 (31.93%); and school-based activity on dengue prevention conducted by teachers, students, and stakeholders were 7 of 16 schools (43.75%). Additionally, the dengue morbidity rates decreased in 2018, and 2019 at 99.83, and 37.26 cases/100 000 populations, respectively (Table 2).
The Phra Saeng District, 22 public health providers used the prediction results for setting up village activities for strengthening villages for dengue prevention, based on the community estimations including LISS values of 74 (100%) and garbage management in villages, integrated with household and local government administrations at 22 (29.75%); for the level of the village larval indices lower than the standard level (BI < 50, HI < 10, and CI < 1), at least two-thirds indices were 50 (67.57%); community capacity activities of village members to increase the capacity for sustainable dengue prevention activities by at least 1 project per village, which was 25 (32.78%); and school-based activity on dengue prevention conducted by teachers, students, and stakeholders was 14 of 27 schools (51.85%). Additionally, dengue morbidity rate decreased in 2018, and 2019 at 50.59, and 35.96 cases/100 000 populations, respectively (Table 2).
Discussions
Risk dengue village prediction criteria were appropriated 3 districts because these were developed based on the integrated knowledge of dengue transmission,2,10 dengue prevention and control, and CAPR approach for strengthening dengue prevention. 1 Regarding the hypothesis of dengue virus in recurrent outbreak areas, the endemic areas refer to villages with more than 1 dengue virus serotype. A population might contract dengue virus, then experience dengue infection several times. 31 Dengue morbidity rate in the current year for each village was compared with the past 5-year median rate, which was the criteria for high density dengue virus when the incidence rate was low for the subsequent year. Immunity against dengue virus lasts for 6 to 12 months; thus, the severity factor criteria were accepted by the Thai MoPH. 19
For village, the opportunity factors of dengue outbreak were 3. The population movement criterion was affected by people flow, wand is likely to enhance virus circulation in specific areas. 11 The appropriate population density affected dengue communicability from the larva in mosquitoes; the higher the population density, the higher was the risk of exposure to dengue virus. In this study, almost all the villages had low density population, which was consistent with the study on population density, water supply, and the risk of dengue fever in Vietnam and the risk factors associated with dengue transmission in Colombia.26,27
Important criteria of this study included village activities for strengthening the stakeholders for dengue prevention in each village. The 5 sub-criteria consisted of activities (10 points) that were also reported in previous studies such as LISS in all villages where such a system existed. The LISS consisted of 6 steps: (i) VHVs survey of the larval indices in 10 to 15 households on 25th of each month was recorded in the “violet book,” (ii) the head of the zone collected data from VHVs in the “blue book” on the 28th and divided the data into 3 to 4 zones per village, (iii) the head of the village collected total data from the head of each zone in the “yellow book” on the 30th, (iv) PCUs collected and recorded all data in the program (http://surat.denguelim.com) monthly, (v) the reports were used at VHVs meeting on the 13th of each month, and (vi) the information was communicated to all stakeholders at village, sub district, and district levels. 28 Three districts (220 villages) conducted the LISS, and these villages had values less than the standard larval indices level of the Thai MoPH.
The village activities for dengue prevention used less information for dengue risk village prediction. The results showed that almost all the village projects for dengue prevention were less than 50%. Particularly, the dengue prevention project for dengue risk prediction including herbs to combat mosquitoes, bank fish for the larvae, a household environmental visit, school-based activities, and garbage management were used as community participatory activities. Their risk scores for dengue outbreak showed constant high levels in some villages because their projects were based on several factors including capacity activities of the village members and community leaders;22,23 the knowledge, attitude, and behavior of public health professionals; 32 schools (teachers and students); authorities of sub district administrative organization and local government organization in the district and province. 33
The utilities of the prediction results were village activities for strengthening the community for dengue prevention activities and consisted of PCU activities for HRDVs and LRDVs, which had different activities. 25 Differences in dengue risk villages for the 3 districts were based on contact with each village, sub district, and district. The PCUs were the coordinating units for each sub district covering the villages because the 3 districts set up the LISS, as reported in the Lansaka model. 28 The professional PCUs supported dengue prevention activities and monitoring and evaluation of the HRDVs and LRDVs differently after January 2019 prediction, as well as the level of dengue risk village when repeated for January 2020 prediction. The dengue morbidity rates differed but decreased from 2018 to 2019. The dengue risk village prediction and village activities for strengthening the community for dengue prevention activities are consistent with the concept of integrated vector management of the World Health Organization (WHO). 1
Limitations
First, the RDVPC was focusing on the dengue severity aspect that referring the output of dengue outbreak, herd immunity, and dengue infection and dengue outbreak opportunity aspect which specially motivated 5 activities of village strengthening. The prediction results need people’ activities for decreasing dengue risk. However, future research need to explore the involving factors such as type of larval indices that breeding from type of mosquito, temperature, rainfall, type of water container, season, etc.
Second, the study used the CAPR approach that appropriated within the context of village in Southern Thailand. Then, the implementing the RDVPC and predicting dengue risk village process needed the participation of all stakeholders for dengue prevention in villages, sub-districts, and districts.
Third, the 5 activities or projects in villages wherein important risk dengue village criteria were, required all stakeholders in the community to participate in the prediction such as school-based dengue prevention activities, and garbage management in household.
Conclusions
The prediction criteria of dengue risk village were developed from 2 aspects consisting of 6 factors: disease severity (3 factors) and outbreak opportunity (3 factors), which integrated epidemiology, entomology, and community activities. The risk prediction process utilized the CAPR method, which included village, sub district, and district stakeholders. Moreover, the criteria were applied using a computer program (http://surat.denguelim.com). The prediction of dengue risk village and village activities for strengthening the community for dengue prevention was consistent with the concept of integrated vector management which included: LISS, garbage management, larval indices levels lower than the Thai MoPH standard, community capacity activity for dengue prevention, and school-based activity on dengue prevention. The risk assessment criteria and process mobilized villages to create dengue prevention activities to decrease the morbidity rate.
Supplemental Material
sj-pdf-1-jpc-10.1177_21501327211013298 – Supplemental material for Developing Risk Assessment Criteria and Predicting High- and Low-Dengue Risk Villages for Strengthening Dengue Prevention Activities: Community Participatory Action Research, Thailand
Supplemental material, sj-pdf-1-jpc-10.1177_21501327211013298 for Developing Risk Assessment Criteria and Predicting High- and Low-Dengue Risk Villages for Strengthening Dengue Prevention Activities: Community Participatory Action Research, Thailand by Charuai Suwanbamrung, Cua Ngoc Le, Supreecha Kaewsawat, Nirachon Chutipattana, Patthanasak Khammaneechan, Supaporn Thongchan, Orratai Nontapet, Cherd Thongsuk, Suphap Laopram, Chamaiporn Niyomchit and Ruchira Sinthu in Journal of Primary Care & Community Health
Supplemental Material
sj-pdf-2-jpc-10.1177_21501327211013298 – Supplemental material for Developing Risk Assessment Criteria and Predicting High- and Low-Dengue Risk Villages for Strengthening Dengue Prevention Activities: Community Participatory Action Research, Thailand
Supplemental material, sj-pdf-2-jpc-10.1177_21501327211013298 for Developing Risk Assessment Criteria and Predicting High- and Low-Dengue Risk Villages for Strengthening Dengue Prevention Activities: Community Participatory Action Research, Thailand by Charuai Suwanbamrung, Cua Ngoc Le, Supreecha Kaewsawat, Nirachon Chutipattana, Patthanasak Khammaneechan, Supaporn Thongchan, Orratai Nontapet, Cherd Thongsuk, Suphap Laopram, Chamaiporn Niyomchit and Ruchira Sinthu in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We acknowledge all participants including the district public health officials and the representatives of the public health officials from all PCUs and 220 villages in the 3 districts, Surat Thani Province. The authors would like to thank the Excellent Centre for Dengue and Community Public Health (EC for DACH), The Institute of Research and Development, School of Public Health, and Walailak University. National Research Council of Thailand (NRCT) (Grant number 56/2017 and 68/2019 from September 2017 to May 2020) supported this work. This research was financially supported by the new strategic research project (P2P), Walailak University. Special thanks to the Elsevier Language Editing Services (Serial number: LE-197866-1DEE07A62E90) for language editing. They did not have any role in the study design, data collection analysis and interpretation, and in writing the manuscript.
Author Contributions
All the authors have read and approved the manuscript. Charuai Suwanbamrung participated in the main roles of all 5 criteria; Cua Ngoc Le, Supreecha Kaewsawat, and Patthanasak Khammaneechan; Nirachon Chutipattana, Supaporn Thongchan, Orratai Nontapet, Cherd Thongsuk, Suphap Laopram, and Chamaiporn Niyomchit participated in the following 5 criteria: (1) made a significant contribution to the work, that is, conception, study design, execution, data acquisition, analysis, and interpretation, in some or all these areas, (2) drafted, wrote, or substantially revised or critically reviewed the article, (3) agreed on the target journal, (4) reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage, and (5) agreed to take responsibility and accountability for the content of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Research Council of Thailand (Grant number 56/2017 and 68/2019 from September 2017 to May 2020) and the Excellent Centre for Dengue and Community Public Health, Walailak University (under Grant [WU-COE-63-004]), supported this work.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.