
Abstract
Background:
The high prevalence of chronic diseases has been an ongoing public concern. The psychological factors, including lack of social support and perceived lack of control, were found to be highly associated with an increased risk of the diseases. In fact, the effect of disease management programs (DMP) in patients diagnosed with chronic diseases were assessed in multiple studies to measure health-related quality of life (HR = QoL), which measured in the EuroQol 5-Dimension Questionnaire (EQ-5D) index score, also known as self-perceived health.
Methods:
The study was conducted using the Korea National Health and Nutrition Examination Survey (KNHANES) from 2007 to 2012 and through descriptive statistics and multiple linear regression to investigate the association of participation in DMP and the EQ-5D index score.
Results:
The results revealed that the subjects diagnosed with hypertension were shown to have a lower quality of life to those without the diagnosis (P < .05). Moreover, in the hypertensive Korean population, DMP did not show any statistically significant impact on the EQ-5D index score (P > .05).
Conclusion:
Our study has assessed the association of DMP and EQ-5D index score in hypertensive patients only although it is still uncertain the effect of DMP on other chronic diseases therefore, further studies should be conducted to investigate the importance of DMP in Korea for the patients with such diseases in improving their quality of life.
• The psychosocial factors including lack of social support and perceived lack of control, are highly associated with increasing risk of chronic diseases. The EuroQol 5-Dimension Questionnaire (EQ-5D), one of the utility measures of HR-QoL, consists of 5 dimensions such as morbidity, self-care, pain/discomfort, usual activities, and anxiety/depression. This standardized measure of health perceptions ensures to inform about public health and health care policy.
• Using the Korea National Health and Nutrition Examination Survey from 2007 to 2012, this study results revealed that the subjects diagnosed with hypertension were shown to have a lower quality of life to those without the diagnosis. Moreover, in hypertensive Korean population DMP did not show any statistically significant impact on the EQ-5D index score.
Introduction
According to Centers for Disease Control and Prevention, chronic diseases are generally defined as conditions that last more than 1 year with having difficulties in activities and requiring continuous treatment and medical support. 1 These diseases generally include heart disease, cancer, chronic lung disease, stroke, Alzheimer’s disease, diabetes, and chronic kidney disease. 1 In the U.S., 6 in 10 adults have a chronic disease and 4 in 10 adults suffer from 2 or more. 1 In case of cancer, more than 1.6 million people in the U.S. are diagnosed and 600 000 people die each year. 2 For diabetes, more than 30 million people in the U.S. suffer from diabetes and 84 million people are at the stage of prediabetes. Lastly, 1 in 4 American adults is shown to suffer from arthritis which adds up to a total of 54.4 million adults who are affected, already. 2 The alarmingly high prevalence of the chronic diseases has alerted the nations around the globe and led to increasing health and economic expenditures. In the U.S., 90% of the country’s $3.3 trillion in annual health care expenditures were used in disease control. 2 With such a large amount of investment in prevention of chronic diseases, it is estimated to prevent 36 million premature deaths and these averted deaths would lead to the economic development, approximating an accumulated economic growth of $36 billion in China, $15 billion in India and $20 billion in Russia over the next 10 years. 3
In parallel with the situation in the U.S., Korea has experienced the high prevalence of such chronic diseases. Based on the national statistical data from the Ministry of Health and Welfare in Korea, the prevalence of hypertension, diabetes mellitus and dyslipidemia known to be the most common chronic diseases in Korea has been increasing on a steady slope. 4 For example, from 1998 to 2016 the average prevalence of hypertension is calculated as 27.5% whereas specifically in 2016 it reached 29%. For diabetes mellitus, the prevalence is calculated as about 10%.5,6 Furthermore, a study has revealed that the prevalence of diabetes mellitus, hypertension and dyslipidemia was 100.01, 175.46, and 186.43 per 1000 individuals in 2015. 7 Specifically for hypertension the total expenditure was estimated as 2850 billion Korean Won which accounts for 13.4% of the overall medical expenditures for all chronic diseases in 2018. 4 Given the situation, by developing and improving the treatment methods or activities to encourage the patients with hypertension this will reduce the expenditure burden in society and improving the quality of life. 4 Moreover, for the management of chronic diseases, in 2011 the Korean government has implemented a new cost sharing enactment to lower the general hospital visiting of patients with mild symptoms including hypertension by increasing all out-of-pocket medical expenses from 50% to 60% for unnecessary outpatient visits to general hospitals in 2009 and increasing the coinsurance rate from 50% to 70% in general hospitals.8,9 By doing so, the government has encouraged the patients with minor diseases to utilize local primary clinics instead of general hospitals because 85% of the general hospital outpatient services were unnecessary and so that such hospitals can be capable of treating patients in urgency with decrease in the unnecessary visit.9,10 For hypertensive patients, the effect of such enactment showed statistical significance to encourage them to visit primary clinics instead of general hospitals. 8 Furthermore, a study published in 2014 was conducted to compare the effect of disease management program in hypertensive patients who visited primary care compared to non-participants and in fact, within the hypertensive group the knowledge level among the participants in the disease management program was significantly larger compared to non-participants. 11
According to World Health Organizations (WHO), the psychosocial factors including lack of social support and perceived lack of control, are highly associated with increasing risk of chronic diseases. 3 In addition, the parameter “self-perceived health” has been recognized as effective measure of overall health status. 12 This parameter is a subjective and relative measure that includes overall physical, mental and social well-being of patients. 12 When considering multiple factors such as incipient disease, severity of disease, physiological and psychological reserves, and social function, the clinical assessment might have difficulties with making a clear distinction to produce results related to patients’ behaviors and health care costs. 12 In a study with noninstitutionalized seniors, the subjects with positive self-perceived health showed a low mortality rate compared to those with negative perceptions.12,13 Due to the global burden of chronic diseases, understanding his/her own well-being and health status has become an important perception for the public to prevent the diseases. 14
Thus, to facilitate the prevention of such diseases, social, mental, and medical aspects should be considered altogether. 15 Health-related quality of life (HR-QoL) is capable of doing so. HR-QoL has been widely used to measure and assess self-perception on own health status.15–17 It provides physical and mental perceptions, health risks and conditions, functional status, social support, and socioeconomic status for individuals. 15 Moreover, it also includes community-level resources, conditions, policies,and practices. 15 The EuroQol 5-Dimension Questionnaire (EQ-5D), one of the utility measures of HR-QoL, consists of 5 dimensions such as morbidity, self-care, pain/discomfort, usual activities, and anxiety/depression. 16 This standardized measure of health perceptions ensures to inform about public health and health care policy.16–18
The ultimate role of the disease management programs (DMP) is to provide patients with techniques and knowledge about carrying daily activities along with their physiological impairment and severity of the diseases by lifestyle adaptation. 19 For example, after completion of DMP, a study involving patients diagnosed with and without diabetes mellitus showed that after a 5-year period of follow-up, the patients diagnosed with diabetes mellitus showed a more gradual drop to those without in the EQ-5D index score. 20 Through the DMP, patients would accept their diagnosis, start to perceive their own health status, and realize that the changes in behaviors are necessary for active participation in treatment. 21
The objective of this study is to investigate the association of participation in DMP and HR-QoL expressed in EQ-5D index score in hypertensive Korean population by using the Korea National Health and Nutrition Examination Survey (KNHANES) IV and V, and further conduct research on the relationship between the participation and other health-related parameters.
Methods
Source of Data
The Korea National Health and Nutrition Examination Survey (KNHANES) is a nationwide cross-sectional survey conducted by the Korea Centers for Disease Control and Prevention to inform about generalized health and nutritional status in Korean population by using stratified multistage probability sample design. First started in 1998, this survey is carried out every year, and thousands of noninstitutionalized Korean citizens are surveyed with a questionnaire about health-related information, including the diagnostic status of chronic diseases via household interviews and physical examination at medical centers. 22 This study was approved by the Ethics Institutional Review Board of Yonsei University (7001988-201912-HR-737-02E), which waived the requirement to obtain informed consent because of the de-identified nature of the data.
The KNHANES contains 3 components in each year’s survey: a health interview, health examination, and nutrition survey. Through mobile examination centers, the health interview and health examination of the subjects are conducted by trained medical staffs and interviewers. Afterwards, dieticians visit the subjects’ houses for filling out the questionnaire that contains socioeconomic status, health behaviors, quality of life, healthcare utilization, anthropometric measures, biochemical profiles, parameters related to dental health, vision, hearing and bone density, X-ray test results and nutritional parameters. 22
Complex survey design analysis
The KNHANES is a complex, stratified, multistage, probability-cluster survey that involves non-institutionalized Korean citizens.22,23 There are 2 methods to perform survey design analysis: simple survey design and complex survey design analysis.22,23 Mostly used by researchers, the simple random sampling method is performed on the stratified multistage survey; however, this method might yield biased point estimates of population parameters, cause underestimation of the standard error for point estimates and produce a small range of confidence intervals on population parameter, and result type I error with underestimation of standard error or variability of statistics. 23 Moreover, the results obtained by analyzing the data using this simple method fail to represent the entire Korean population because it does not consider sampling weights. 23 Thus, to perform analysis by using the KNHANES, the complex survey design analysis, which sampling weights were applied to account for, is highly advised. 23
Data Collection
From the KNHANES IV and V, the data including age, sex, height, weight, waist circumference, body mass index, region of residence, individual income, household income, level of education, occupation, marital status, health insurance type, type of family structures, current smoking status, frequency of alcohol consumption in the past year, current obesity status, self-perception of own health status and body shape, impairment of body function in last weeks, changes in weight in past year, maintenance of weight in past year, self-perception on stress, continuation of depression for more than 2 weeks, thoughts about suicide and actual suicide attempts in past year, psychological counseling in past year, participation in DMP, 5 dimensions of EuroQoL (including mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), and EQ-5D index score.
The KNHANES calculated EQ-5D, one of health-related quality of life (HR-QoL) measures, by performing a survey for selected 5 dimensions. EQ-5D index score ranges from 0 (health status with no better than death) to 1 (perfect health status). The questionnaire for the index contains 3 possible choices: 1 = no difficulties, 2 = some difficulties and 3 = severe difficulties. The formula for the EQ-5D index score is as follows: EQ-5D index = 1 – (0.05+0.096*M2 + 0.418*M3 + 0.046*SC2 + 0.136*SC3 + 0.051*UA2 + 0.208*UA3 + 0.037*PD2 + 0.151*PD3 + 0.043*AD2 + 0.158*AD3 + 0.05*N3)
where M2 is morbidity “level 2” = 1; otherwise, 0; M3 is morbidity “level 3” = 1; otherwise, 0; SC2 is self-care “level 2” = 1; otherwise, 0; SC3 is self-care “level 3” = 1; otherwise, 0; UA2 is usual activities “level 2” = 1; otherwise, 0; UA3 is usual activities “level 3” = 1; otherwise, 0; PD2 is pain/discomfort “level 2” = 1; otherwise, 0; PD3 is pain/discomfort “level 3” = 1; otherwise, 0; AD2 is anxiety/depression “level 2” = 1; otherwise, 0; AD3 is anxiety/depression “level 3” = 1; otherwise, 0; N3 is only one “level 3” = 1.
Study Population
Figure 1 explains the process of selecting the study population for the purpose of this study. From the KNHANES IV and V, a total of 50 405 subjects (24 871 from KNHANES IV and 25 534 from KNHANES V) was identified. For the subjects who were diagnosed with hypertension, the diagnosis twas est carried out by medical doctors. A total of 1876 subjects was found to be diagnosed with hyperten,sion and 89 subjects were confirmed as non-hypertensive.
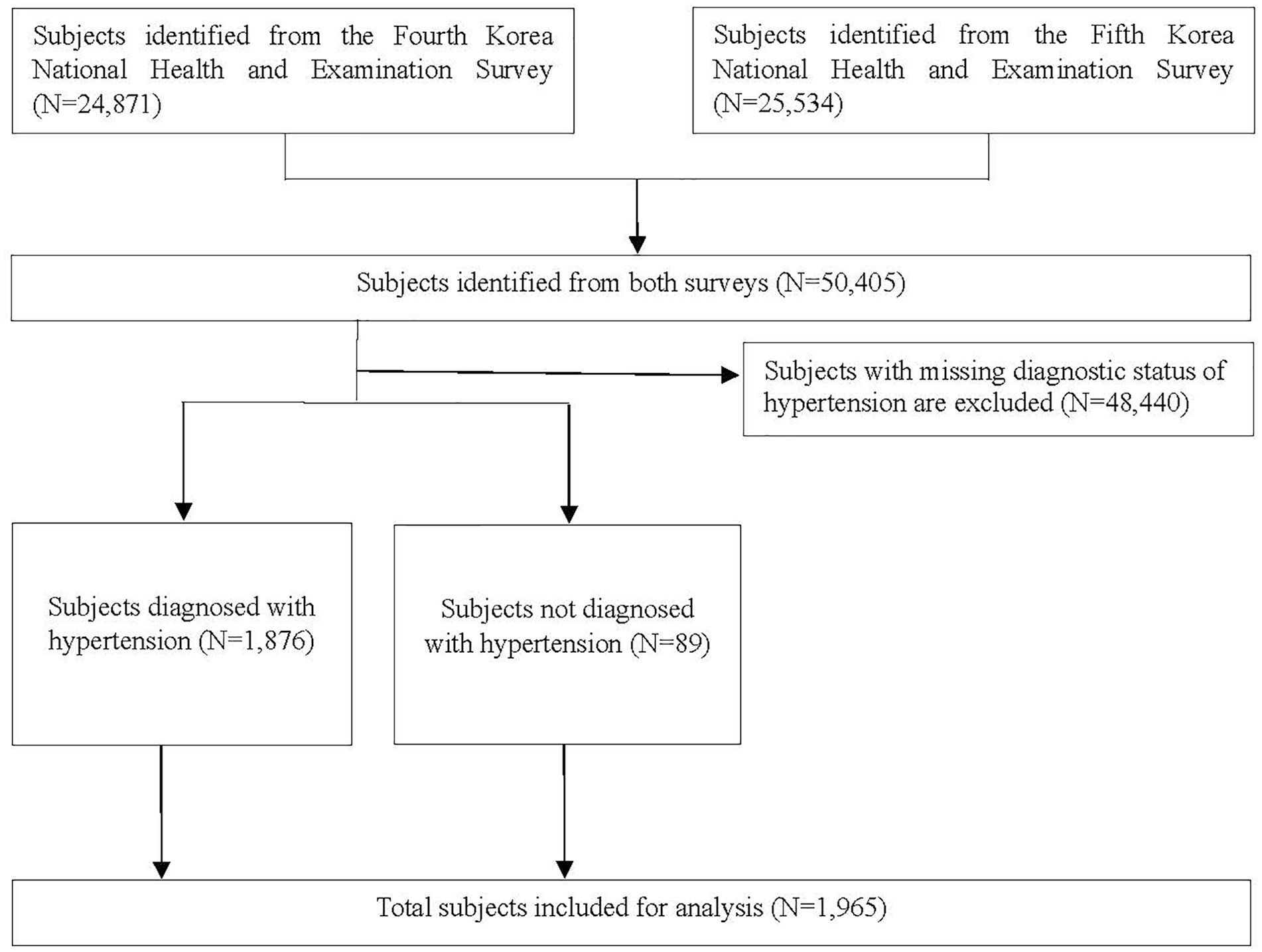
Selection of study population for the purpose of this study.
Statistical Analysis
To facilitate the analysis, subjects with missing values for certain parameters were excluded. The baseline characteristics of the population diagnosed with hypertension were collected by performing descriptive statistics. Data were presented as number of subjects and percentage (%) in parenthesis for categorical variables and estimated mean ± standard deviation or standard error for continuous variables. Moreover, to find the association of the participation of patients in DMP and other included health-related variables with EQ-5D index, this study performed multiple linear regression model with 95% confidence interval (CI). Standardized beta coefficient (β) was included in this study with P-value lower than .05 indicating statistical significance. All the statistics were calculated using SAS ver. 9.4 (SAS Institute, Cary, NC, USA).
As the multiple linear regression model is used, the following formula for the model is implemented for the results:
(1) Multiple linear regression model
E(y) = β0 +β1x1 + β2x2 + β3x3 +. . .+ ε
where β0 is the y-intercept of the regression line, β1 is the slope, ε represents the error term, and E(y) is the mean or expected value of y for a given value of x. For clarity, the multiple linear regression considers that more than one independent variable altogether estimates the value of the dependent variable.
Results
Baseline Characteristics
In both surveys, the subjects diagnosed with hypertension were older (54.79 ± 0.59 years in KNHANES IV, 58.37 ± 0.52 years in KNHANES V), shorter in height (162.72 ± 0.45 cm in IV, 161.65 ± 0.34 cm in V), and less heavier (66.38 ± 0.57 kg in IV, 65.36 ± 0.50 kg in V) compared to non-diagnosed subjects (P < .05) (Table 1).
Baseline Characteristics of the Subjects Diagnosed with Hypertension from the Korea National Health and Nutrition Examination Survey (KNHANES) IV and V. a
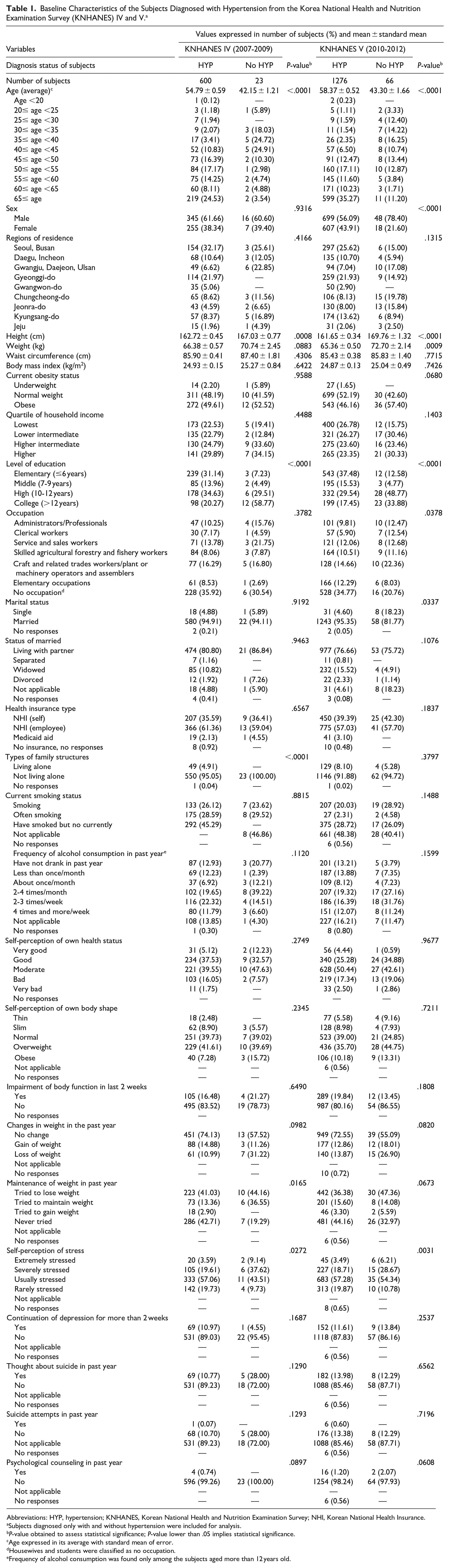
Abbreviations: HYP, hypertension; KNHANES, Korean National Health and Nutrition Examination Survey; NHI, Korean National Health Insurance.
Subjects diagnosed only with and without hypertension were included for analysis.
P-value obtained to assess statistical significance; P-value lower than .05 implies statistical significance.
Age expressed in its average with standard mean of error.
Housewives and students were classified as no occupation.
Frequency of alcohol consumption was found only among the subjects aged more than 12 years old.
More than 80% of the subjects without the diagnosis of hypertension were found to be highly educated (more than 9 years of education), whereas the diagnosed subjects only showed about 50% (P < .05). In addition, a higher percentage of the subjects in the diagnosed group from both surveys attempted to lose or maintain weight and, furthermore, had thoughts about suicide in past year more frequently in comparison with the opposed group (P < .05).
Five dimensions in EuroQoL and EQ-5D index score
EuroQoL, expressed in EQ-5D index score, includes 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. First in Table 2, for mobility, usual activities, and pain/discomfort, statistically significant differences were found in the distribution of the subjects between ones with and without the diagnosis of hypertension (P < .05). Next, for self-care the diagnosed and non-diagnosed groups of hypertension from both surveys exhibited statistically significant differences in-between (P < .05).
Health-Related Quality of Life (HR-QoL) in the Subjects in the Korea National Health and Nutrition Examination Survey (KNHANES) IV and V.

Abbreviations: CI, confidence interval; EQ-5D, EuroQoL-5 dimensions; HYP, hypertension; QoL, quality of life.
Effect of health-related variables and DMP on EQ-5D index score.
Subjects in the fourth and fifth surveys were included as a whole and displayed as ‘Number of subjects’, implying the total number of the subjects in each disease.
The 5 dimensions of EuroQoL include mobility, self-care, usual activities, pain/discomfort, and anxiety/depression.
P-value obtained to assess statistical significance; P-value lower than .05 implies statistical significance.
EQ-5D index score ranges from 0 to 1; 0 for death and 1 for perfect health.
Furthermore, more than 80% of the subjects diagnosed with hypertension had no problems with walking or changing clothes alone, performing usual activities, and feeling anxious or depressed. Also, about 5% to 8% of the total subjects were incapable of performing usual activities, suffering from severe pain or discomfort, and anxiety or depression.
The subjects diagnosed with and without hypertension obtained the EQ-5D index score of 0.944 (95% CI 0.939-0.949) and 0.980 (95% CI 0.97-0.99) with statistical significance (P < .05). In other words, being diagnosed with hypertension would cause statistical significance differences in quality of life among the subjects.
Supplement 1 shows the baseline characteristics of the subjects included and excluded for the purpose of this study.
Through performing multiple linear regression, the association of health-related variables and EQ-5D index score was assessed and expressed it in standardized beta coefficients (β), referring to Table 3.
Association of Health-Related Variables and EQ-5D Index Score Expressed in Standardized Beta Coefficients (β) Obtained from Multiple Linear Regression Model with Corresponding Standard Error and P-Value in Subjects Diagnosed with Hypertension.

Abbreviations: β, standardized beta coefficient; REF, reference; SE, standard error.
Standardized beta coefficient (β) obtained from multiple linear regression model with P-value found from t test.
P-value obtained to assess statistical significance; P-value lower than .05 implies statistical significance.
Diagnosis of the subjects with hypertension by medical doctor.
Types of family structures categorized into ‘living alone’ and ‘not living alone.’
Obesity status categorized into body mass index (BMI) as underweight (BMI < 18.5), normal (18.5 ≤ BMI < 25), and overweight (25 ≤ BMI).
The results revealed that for hypertension, the subjects who lived alone had feelings of depression and obesity status of underweight (BMI < 18.5), and answered with moderate or bad for self-perception of own health status, showed statistically significant associations with the EQ-5D index score (P < .05). In detail, among the subjects the β of .052 was found for types of family structures, represents that living alone would have a positive relationship with the index score (P < .05). Moreover, the self-perception of own health status as bad was found to cause the index score to reduce more significantly in its value in comparison with those who answered moderate (P < .05). Furthermore, the association of participation in DMP and the EQ-5D index score was assessed among the subjects diagnosed with hypertension; however, no statistically significant effects were found (P > .05).
Discussion
Although the impact of DMP on improvement of QoL has been documented in multiple studies, the relationship between DMPs, QoL, expressed in EQ-5D index score, and other sociodemographic variables based on Korean population were not yet investigated. Through this study, the sociodemographic variables such as types of family structures, current smoking status, alcohol consumption, self-perception of own health status, body shape, and stress impairment of body function, and current obesity status, were included to document any statistically significant association between them.
The results showed that participating in DMP would improve QoL in subjects diagnosed with hypertension. If the entire population included in the surveys were considered, the subjects diagnosed with hypertension significantly observed EQ-5D index score get worsen.
In fact, the conclusion drawn was consistent with other studies; however, some studies included other chronic diseases not dealt in this study.24,25 Interestingly, a study with heart failure patients found that HR-QoL was a strong predictor of outcome in younger patients (<65 years); however, for more elderly patients (≥80 years) it was not useful in predicting outcome. 24 Our results also suggested that the subjects diagnosed with DM were 59.47 ± 0.44 years old in KNHANES IV and 61.10 ± 0.46 in V.
In other studies, other measures were implemented such as cardiovascular deaths, rehospitalization, emergency room visits, all-cause mortality to assess QoL in ill patients.26,27 Unfortunately, the KNHANES did not involve such variables and thus, other available data sets should be searched for further research on the association between them.
The present study has important strengths with using the KNHANES. This survey is a nationally representative sample that includes a wider range of health-related variables created through physical examination or visiting households by health professionals. Moreover, as the Centers for Disease Control and Prevention in Korea strongly suggested, the complex survey design was implemented throughout the entire process of analysis to better represent the entire Korean population by applying sample weights for each sample person. On the contrary, the KNHANES had several limitations. In this cross-sectional nationwide survey the causal inferences about the relationship between the variables could be precluded. Due to the characteristics of the survey, the subjects included in a certain year of survey could not be followed-up for longer duration. Also, the survey only contained noninstitutionalized population, excluding potential subjects who were not included in the survey. Moreover, it lacked the information to make an association of disease progression or recovery and changes in EQ-5D index score. Another limitation would be low number of the patients diagnosed without hypertension; however, if any of the patients included in the KNHANES was diagnosed with diabetes mellitus, arthritis or asthma which were one of the variables provided from the KNHANES were excluded for the purpose of this study to precisely investigate the association of DMP in hypertensive or non-hypertensive patients. Although the number of the patients without hypertension is low, it would not infer the effect one of the diagnosis status of chronic diseases in patients and would rather provide the meaningful data to represent the positive effect of the participation in DMP in hypertensive patients compared to non-hypertensive patients.
Conclusion
In conclusion, the present study manifested the positive association between participation in DMP and EQ-5D index score in the subjects diagnosed with hypertension. Moreover, the diagnostic status of hypertension caused a lower QoL in hypertensive patients. Therefore, the government authorities or community should acknowledge that it is important to encourage hypertensive patients for their participation in DMP and develop organized and detailed programs accordingly. Although other chronic diseases are not investigated through this study, further studies that involve other health-related measures focusing on the association of such diseases with globally high prevalence and patients’ QoL, should be conducted to inform the public. Thus, to help them recover from the diseases and complications, new policies and management should be implemented for Koreans to achieve a better QoL.
Supplemental Material
sj-pdf-1-jpc-10.1177_21501327211012185 – Supplemental material for Association of Participation in Disease Management Programs and Health-Related Quality of Life in Korean Population: Results from the Korea National Health and Nutrition Examination Survey IV and V (2007-2012)
Supplemental material, sj-pdf-1-jpc-10.1177_21501327211012185 for Association of Participation in Disease Management Programs and Health-Related Quality of Life in Korean Population: Results from the Korea National Health and Nutrition Examination Survey IV and V (2007-2012) by Wonkyung Lee, Euna Han and Junjeong Choi in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was part of research projects funded by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (NRF-2018R1A6A1A03023718 and NRF-2020R1A2C1003378).
Ethics Statement
The study was approved by Ethics Institutional Review Board of Yonsei University (7001988-201910-HR-737-01E) which waived the requirement to obtain informed consent from the subjects included in the study because of incapability to identify the included subjects by any means.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.