
Abstract
Background:
The present Malaysian healthcare system is burdened with increasing cases of non-communicable diseases (NCDs) and its risk factors. Health care providers (HCPs) have to provide both treatment and health education to ensure optimal outcome. Health education is a vital component in addressing and managing chronic diseases. This study intends to explore patient’s perspective on health education services received from HCPs, focusing at the secondary triage in government primary healthcare facilities.
Methods:
This qualitative exploratory study focused on the health education component derived from a complex enhanced primary health care intervention. Participants were purposively selected from patients who attended regular NCD treatment at 8 primary healthcare facilities in rural and urban areas of Johor and Selangor. Data collection was conducted between April 2017 and April 2018. Individual semi-structured interviews were conducted on 4 to 5 patients at each intervention clinic. Interviews were transcribed verbatim, coded and analyzed using a thematic analysis approach.
Results:
A total of 35 patients participated. Through thematic analysis, 2 main themes emerged; Perceived Suitability and Preferred HCPs. Under Perceived Suitability theme, increased waiting time and unsuitable location emerged as sub-themes. Under Preferred HCPs, emerging sub-themes were professional credibility, continuity of care, message fatigue, and interpersonal relationship. There are both positive and adverse acceptances toward health education delivered by HCPs. It should be noted that acceptance level for health information received from doctors are much more positively accepted compared to other HCPs.
Conclusion:
Patients are willing to engage with health educators when their needs are addressed. Revision of current location, process and policy of health education delivery is needed to capture patients’ attention and increase awareness of healthy living with NCDs. HCPs should continuously enhance knowledge and skills, which are essential to improve development and progressively becoming the expert educator in their respective specialized field.
Background
Healthcare services in Malaysia are universally accessible by its entire people. To maintain this accessibility, the Ministry of Health (MOH) heavily subsidized public healthcare (sectioned into primary, secondary, and tertiary care). In contrast, the private or Non-Governmental Organizations (NGO’s) ran the private sector (sectioned into primary and secondary care). Primary care in the public sector focuses on community-based preventive care, especially in rural areas, whereas secondary and tertiary care focussed more on curative care. 1 The private healthcare system is a full paying system. People who seek treatment in the private sector are required to pay through insurance or out of their own pocket. 2
According to the World Health Organization (WHO), non-communicable diseases (NCDs), especially ischaemic heart disease and stroke, remained the leading causes of death among people globally for the last 15 years. 3 This is related to people’s unhealthy behaviors such as not adopting a healthy lifestyle, unbalanced diet, lack of exercise, and so on. In Malaysia, there are increasing NCDs2,4; with ischaemic heart diseases is also one of the principal causes of death. 5 These situations increase burden to the healthcare system, especially at the primary care. People from various age groups and varying disease conditions went to a primary healthcare center as the first contact with a health professional. Thus, primary healthcare is overcrowded with patients, and this overstretched and overworked the healthcare workers. Therefore, over the last couple of years, the government wishes to upgrade and restructure the healthcare systems.
As a response to address the increasing NCDs cases in Malaysia, the government took the initiative to improve NCDs management for Malaysians. In 2017, the Ministry of Health introduced an intervention known as Enhanced Primary Healthcare (EnPHC). This intervention was conducted at selected public government primary healthcare clinics in the states of Johor and Selangor. The EnPHC initiatives consisted of redesigning work processes in the clinic, community intervention through community enrolment and profiling, and improving the referral system between the clinic and hospital. 6 One of the intervention components of the EnPHC is the provision of health education to attending patients. One of the aims of EnPHC is to ensure improvements in patient care experience toward a patient-centered approach using active, population-level strategies for health and wellness. The paper focuses on the experience of receiving health education services in the views of the patients as a client to the EnPHC clinics. Patient feedback is highly valuable in intervention implementation where they are the end-user of the intervention, and their needs have to be met if they are to be part of the solution.
Health education has been defined as any combination of learning experiences designed to influence an individual’s knowledge and health behavior to improve, maintain, or learn to cope with their illness. 7 Health education for a patient is widely recognized in the medical community by disseminating information, counseling, and or behavioral treatment.8-10 It is regarded as one of the primary vital elements in disease risk factor reduction; it helps patients modify their lifestyle and become self-managed of their illness.11,12 Patients who attend a structured health education session may improve their health-related quality of life compared with those who do not follow the session. 13
Health education activities in the EnPHC clinic are conducted at secondary triage, along with other procedures (the completion of NCDs care form, vital sign monitoring, health risks stratification, and other health screening procedures such as Pap smear). 4 Before this EnPHC, health education was done by doctors, mostly during the consultation time. In certain selected cases, diabetic educators will attend to the patient’s need for health education and counseling. In the post-intervention, both doctors and paramedics, including nurses, collectively known as healthcare providers (HCPs), are empowered to deliver health education to patients. Paramedics, including nurses, are trained to manning the secondary triage, whereby screening risk factors and deliverance of health education on NCDs topics, particularly Diabetes and Hypertension management, occurs.
Methods
This study is a qualitative exploratory approach to describe the patients’ view toward health education services given by the HCPs, both at the consultation room and secondary triage. 4 A semi-structured interview guideline was adapted from Karl Weick’s Sense Making Theory (SMT) Framework. The SMT looks at the process by which people give meaning to their collective. According to Weick, identity, retrospective, socialization, ongoing awareness, extracted cues, plausibility and sufficiency are the 7 properties in sensemaking toward events. 14 In this study, SMT was used to develop core questions and specific prompting questions to explore patients’ experience during the intervention implementation for participants to make sense of every intervention they could identify.15-17
The interview guideline was also developed using earlier feedback given by liaison officers (LO) at the intervention clinics through a self-reported assessment form and a structured observation checklist. The study’s interview guide was also used as part of a more extensive study assessing patients’ experience. A detail of the Interview Guideline was shown in Supplemental Appendix A.
Participants
Purposive sampling was drawn out. A total of 20 public government primary healthcare clinics in Johor and Selangor were directly involved in EnPHC intervention since 2017. 4 However, only 8 public government primary healthcare clinics have similar characteristics, such as urban and rural areas, the building’s structural size, and the secondary triage location at the site, which made these clinics eligible and suited our study criteria.
Care Coordinator (CC) is the leading player in EnPHC who engaged the community regarding their appointments, treatment, and medications. Their responsibilities included taking care of the NCD care form, the visit checklist, and the appointment and medication-refill defaulter tracking mechanisms. 4 For the purpose of this study, CC was given a task to identified 4 to 5 participants among patients who were more suited to provide relevant information based on the inclusion criteria (i) registered patient at the clinic, (ii) Malaysian citizen, (iii) attended regular NCDs follow-up appointments for at least 2 years or attended at least 3 visits (NCDs appointments) commencing July 2017, (iv) could converse in English or Malay, and (iv) no hearing or visual impairment.
Based on the above criteria, participants were approached personally only by CC. Before the study commencement, no contact occurred between research team members and participants. Once the participants agreed to participate, a semi-structured face-to-face interview was conducted individually by research team members who were trained in qualitative methods. A study concept, purpose and process were briefed to participants by the research team members before a written permission were taken from them. This process was repeated until saturation was achieved at 35th participant.
Data Collection
Data for this paper were derived from the EnPHC process evaluation study by utilizing the patients’ interview data which had been collected at the end of the 10 months intervention, which commencing April until July 2018. Notes jotted down, and an audio recording was done during the interview process upon receiving written permission from the participants. Each interview session lasted between 30 and 120 minutes. The recorded interview was transferred verbatim, and field notes were documented for easy cross-validation.
Analysis
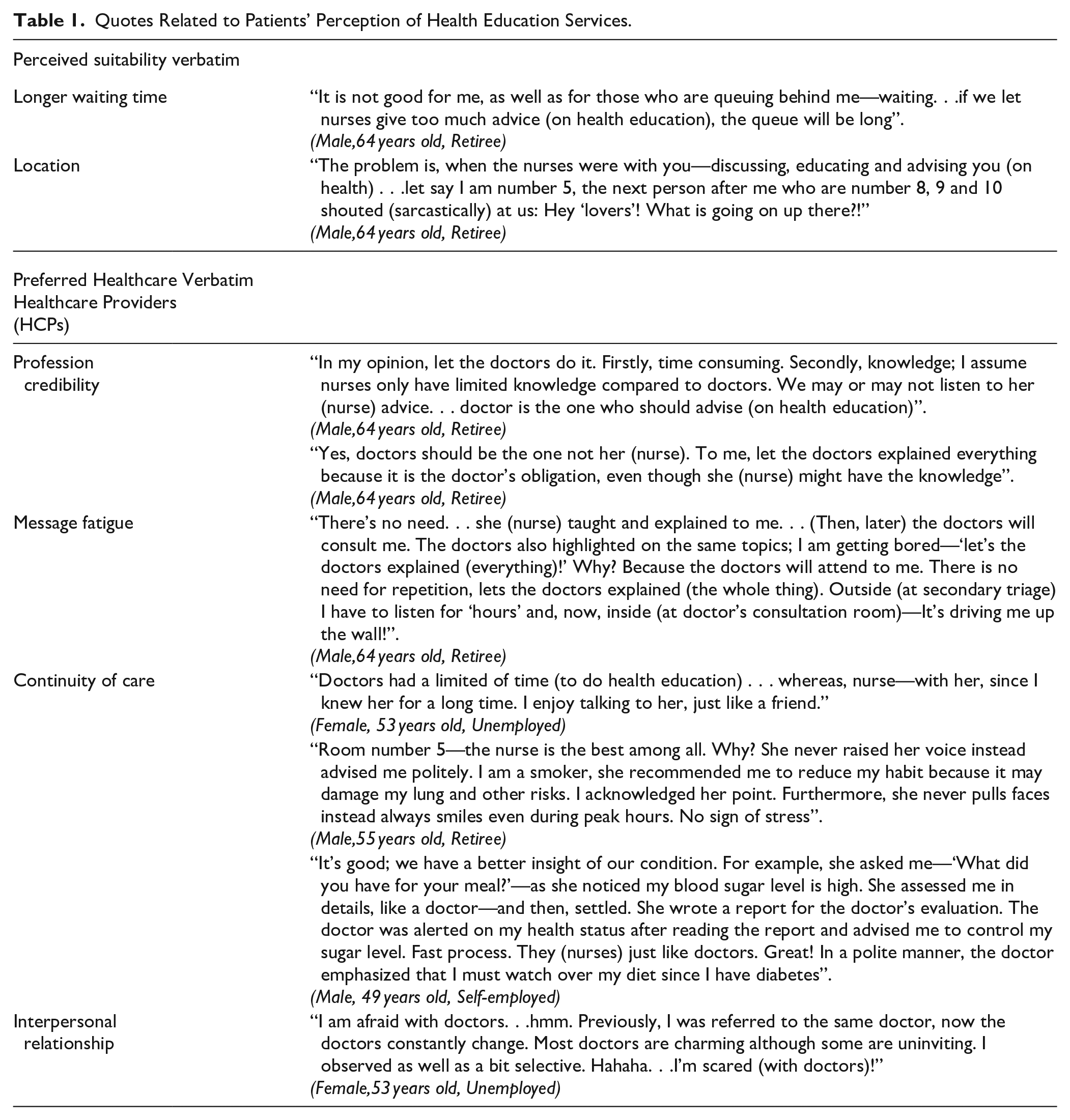
All transcripts, recorded interviews, and documents were examined by appointed neutral parties who do not hold impartial views of the study. The thematic analysis method was done by the EnPHC: PE research team members who are experts in their own research lens. 18 Multiple researchers read transcribed interviews to identify preliminary themes independently according to participants’ experiences as per EnPHC guidelines. The meaning units were reviewed, identified, and sorted into themes before classified into subgroups. Finally, through consensus, the contents of each code group were summarized and categorized into main themes. The quotes that best presented the themes were chosen and tabled to support the results (see Table 1).
Quotes Related to Patients’ Perception of Health Education Services.
Results
A total of 35 patients participated in the study. The biggest group of participants are aged between 60 to 69 years, females, retirees and completed secondary high school education. The socio-demographic of the characteristics were depicted in Table 2.
Characteristics of Participants.

Note. All participants are diabetic and/or hypertension patients.
All participants were either diagnosed with diabetes and/or hypertension from 1986 to the most recent diagnosis in 2018. Since July 2017 (implementation of the EnPHC intervention), the participants had an average of 3 to 4 visits to the clinic.
Analysis of the data revealed 2 main themes identified: (i) perceived suitability and (ii) preferred Healthcare Providers (HCPs). Under the first theme, 2 sub-themes emerged—increased waiting time and unsuitable location. Four sub-themes emerged from the second theme—professional credibility, message fatigue, continuity of care, and interpersonal relationship.
1. Perceived Suitability
There are certain loopholes identified in health education deliverance at secondary triage from the participants’ lens. Setbacks include time management and strategic location, which mismatched health education’s suitability at secondary triage.
1.1. Increased waiting time
Participants reported longer waiting times before consultation as compared to before the intervention. This consequently contributed to discomfort and frustration among patients. While health education is the core business at the secondary triage, this situation was unfortunately seen as the leading reason for bottleneck disputes, especially those in the queue.
1.2. Perceived unsuitable location
Due to space limitations in the primary healthcare facilities, most health education activities were conducted in an open area (secondary triage). This practice—made compulsory as a preintervention guide is conducted before entering the doctor’s consultation room. It was highly visible and can be visually seen but not heard by patients sitting near the waiting room. Unfortunately, it causes patients to perceive the visible health education activity adversely, consequently delaying the treatment process and adding more to the waiting time. Nurses were mis-observed as chatting with patients, although the actual activity was provided health information with the attended patient.
2. Preferred Healthcare Providers (HCPs)
2.1. Professional credibility
Most participants preferred accepting health education counseling from doctors. Some perceived nurses as less-knowledgeable compared to doctors. Thus, they hesitated to listen to advice from nurses. To some, only doctors were perceived to be more trustworthy in delivering health education.
2.2. Message fatigue
Nurses and doctors have repetitively given the same messages to the participants during health education at the secondary triage and consultation room. The intention is done to create greater awareness for patients. However, participants felt that nurses don’t have to carry out health education since doctors will repeat the same messages during the consultation. Some patients claimed that they are tired and exhausted due to prolonged exposure to similar messages, which eventually caused a lack of interest in the given messages.
2.3. Continuity of care
Having tolerant, thoughtful, and friendly healthcare providers, especially among the nurses, benefited patients during their frequent visits to the clinic as it signifies positive ambience. It helps to establish a good relationship between both and allows for the continuity of healthcare. Simultaneously, patients’ detailed assessments were performed at secondary triage, facilitating the assessment procedure at the consultation room.
2.4. Lack of interpersonal relationship
High turnovers of doctors at the clinic somehow allow other HCPs like nurses and paramedics to establish a good rapport with patients. Moreover, negative attitudes among doctors build gaps between them and patients. Hence, some patients were more comfortable dealing with nurses and paramedics than doctors due to the high turnover.
Discussion
This study was conducted to explore patients’ perceptions of health education services given by the healthcare provider at the secondary triage during EnPHC’s intervention. 4 Patient-provider communication is seen as an essential element in health education. Effective communication will be able to help patients to receive and understand important messages deliver by healthcare providers. This will empower and enable patients to be responsible for their care. 8
Our study revealed most participants felt health education received at the secondary triage during EnPHC’s intervention is inappropriate and contributes to longer waiting time in the waiting area. A study in primary healthcare services in Saudi Arabia found that 12.8% indicated that the health education sessions were long enough, and 16.2% of the respondents claimed that the waiting time was utilized for health education. 19 During the intervention, health education and health risk stratification were conducted mostly by a female nurse. Most secondary triage is placed in an open space in the waiting area due to the existing clinic layout. During peak hours, patients and family members tend to linger around the waiting area because of lacking seating places. Participants highlighted how uncomfortable they felt when others observe the process of health education that is meant to be done privately and discreetly; without prying eyes that sometimes raises eyebrows—believing nurses are fraternizing with patients instead of working. Some patients felt that exposing themselves (eg, hands and feet for diabetic education) to the opposite gender during the health education’s session culturally and religiously is also inappropriate. Therefore, to release discomfort, it is necessary to set up secondary triage in a room instead of open space. Options to receive health education from male or female healthcare providers should be given to the patient. Although health education is essential in ensuring patients understand the importance of prescribed treatment adherence, one should not overlook body language, voice tone, and mannerisms that contribute to the health education delivery process’s success. In this study, when patients are pressed for time, they are in a more vulnerable condition and lesser emotional control than usual. Their focus is more toward the intention of wanting to see the doctor. To resolve this conflict at the secondary triage, healthcare providers should carefully observe patients’ verbal and non-verbal communication cues even before the first verbal exchange. Establishing eye contact, exchanging appropriate greetings according to local culture and, addressing patients formally or informally depending on circumstances are as important as to what is spoken (health education) or documented. These social interaction methods enable patients to relax before engaging (patient-doctor communication) with the healthcare provider. Being attentive, helpful and having an affirmative interaction helps to develop the element of trust, and this will result in the patient being more attentive toward the communication exchange during health education. 20
The growing health literacy amongst patients nowadays led to the preference of healthcare providers in giving health education. Doctors and nurses are responsible to provide information and opportunity for patients to make their own decisions regarding their care and treat them fairly and equitably. According to general belief, nurses are expected to play an educational role in health-related issues since they spend more time with patients. However, in this study, most participants desired doctors to deliver health education rather than other healthcare providers. Negative perception nurses lack physicians’ expertise in conducting health education is one of the reasons for this low confidence. 21 A study done in India showed almost one-third of patients perceived nurses not serving adequate explanation and information for their treatment in hospitals, home care, and follow up advice. 22 According to several studies, the doctor serves as a powerful influencer in giving health education to patients; to achieve desired health goals and better health treatment compliance.23-27 Even though society’s perception and portrayal of doctors are the most credible and trustworthy source of health information, some participants in this study prefer to deal with nurses due to a long-standing mutual trust between them. Participants claimed they felt freer to discuss their condition and medical concerns with nurses as they are seeing the same nurses all the time; increasing bonded familiarity.21,28 Due to the EnPHC intervention of introducing health education at the secondary triage, doctors in the consultation room tend to confirm the health education given. However, participants perceived this dual nature of health education as repetitious. Repetition may be beneficial in increasing familiarity over various messages addressing a common health concern, but once it reached a certain threshold point, it will worn out the participants, and decreased the effectiveness of the messages. 29 They felt that nurses should skip that consultation part and leave it to the doctors to recommend instead. A study in 2011 also drew the same conclusion when the patients think they can minimize their risk when someone like doctors, whom they rely upon more, are giving them advice. 30
Conclusion
In this study, we explored patients’ views toward health education services given by the HCPs at primary healthcare. Our result concluded that patients willing to engage with health education when their perceptions and beliefs are adequately addressed. Revision of current location from an open space to a more private space (ie, closed room for health education), process and policy of health education delivery is needed to capture patients’ attention and increase awareness of healthy living with NCDs. Healthcare providers should continuously enhance their knowledge and skill, which is essential to improve health education development, progressively to become the expert educator in their respective specialized field.
Supplemental Material
sj-docx-1-jpc-10.1177_2150132720980629 – Supplemental material for Patients’ Perception Towards Health Education Services Received at the Enhanced Primary Healthcare Facilities: A Qualitative Exploration
Supplemental material, sj-docx-1-jpc-10.1177_2150132720980629 for Patients’ Perception Towards Health Education Services Received at the Enhanced Primary Healthcare Facilities: A Qualitative Exploration by Norrafizah Jaafar, Komathi Perialathan, Mohamad Zaidan Zulkepli, Zaikiah Mohd Zin, Patricia Elisha Jonoi and Mohammad Zabri Johari in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The paper would like to thank the Director General of Health Malaysia in the support of publishing this article. A special thanks to the EnPHC: PE Study Team, HCPs at all 20 clinics and participants of the study. A huge thanks to Dr Low Lee Lan, the principal investigator of this project, for successfully leading the huge task of conducting this study.
Author Contributions
NFJ, KP, MZJ, MZZ, and ZMZ were responsible for the concept, development, interview conduct, and supervision of the research. NFJ, KP, MZZ, and MZJ analyzed the data. NFJ, KP, MZZ, ZMZ, and PEJ constructed the draft manuscript. All authors contributed to the preparation of the manuscript, reviewing and approving the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research and publication of this article is funded by the Ministry of Health Malaysia via the National Institutes of Health Malaysia research grant under the following research registration number NMRR-17-295-34771. Funder is also the stakeholder of the study but does not participate in the study process.
Ethical Approval and Consent to Participate
This study has been approved by Malaysia Research Ethics Committee and supported by the grant from National Institutes of Health, Ministry of Health, Malaysia (NMRR NUMBER:17-295-34771). Informed written consent was taken from all participants at the beginning of the study.
Availability of Data and Materials
The dataset that support the findings of this article belongs to the EnPHC study. At present, the data are not publicly available but can be obtained from the authors upon reasonable request and with the permission from the Director General of Health, Malaysia.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.