
Abstract
Background:
Inhaled corticosteroids (ICS) are the foundation of asthma management. However, ICS non-adherence is common. Black adults have lower ICS adherence than white adults, which likely contributes, in part, to the asthma disparities that Black adults experience.
Objective:
To explore how Black adults with uncontrolled asthma and their primary care providers communicated about ICS non-adherence and used shared decision-making to identify strategies to increase ICS use.
Design:
Eighty routine clinical visits for uncontrolled asthma were audio recorded and inductively analyzed using methods adapted from grounded theory methodology.
Participants:
Study participants included 80 Black adults (83% female) largely low-income (83% Medicaid) and their 10 primary care providers. The study settings were 2 Federally Qualified Health Centers.
Key Results:
Three overarching themes were identified: (1) ICS misuse and lack of knowledge; (2) external influences informed personal misconceptions about ICS; and (3) patient-provider communication to individualize plan of care.
Conclusions:
Reasons for ICS non-adherence in Black adults with uncontrolled asthma offer potential targets for interventions that facilitate enhanced adherence. Future research should include PCP training on strategies that support patient-centered care, such as communication, shared decision-making and patient engagement.
Introduction
As many as 63% of patients diagnosed with asthma demonstrate suboptimal adherence to inhaled corticosteroid (ICS) medication. 1 ICS use is widely acknowledged as the most effective approach to gaining asthma control and reducing preventable hospitalizations and death. 2 Despite being the first-line treatment for asthma management, ICS non-adherence is one of the primary causes of uncontrolled asthma, increasing a patient’s risk of adverse effects and mortality. 3
Compared to white adults, ICS non-adherence rates are higher in Black adults. Data from over 5000 adults in the 2006 to 2010 Medical Expenditure Panel Survey shows that Blacks have reduced odds (28%-51%) of ICS adherence compared to white adults 4 even when access to care and prescription coverage are held constant. Black adults are nearly 4 times more likely than white adults to fail to fill an ICS prescription. 5 This is alarming as, relative to white adults, Black adults have higher rates of asthma and 2 to 3 times higher morbidity and mortality. 6 If ICS adherence was higher among Black adults, 25% of asthma exacerbations leading to hospital care could be averted.7,8
Barriers to ICS adherence in Black populations have been well-documented in the literature and reflect access issues, a preference for non-prescription treatments, suboptimal communication between patients and providers, and erroneous or negative medication beliefs.2,9-11 A recent systematic review identified the absence of tailored interventions for increasing ICS use specifically for Black populations.8,12 What is not well understood is how self-management decisions are identified and addressed during clinical encounters. Determining if and how providers discuss obstacles to ICS adherence with their adult patients could be useful to identify targets for tailored interventions. The purpose of this study was to explore if/how Black adults with uncontrolled asthma and their primary care providers (PCPs) communicate about reasons for ICS non-adherence and strategize to increase ICS use.
Methods
This qualitative study was a part of a larger clinical trial that has been reported elsewhere. 13 The study was conducted in 2 Federally Qualified Health Centers in Philadelphia. The patient population within these 2 sites are largely uninsured, receiving Medicaid, or dually eligible (Medicare/Medicaid). All PCPs actively managing a panel of adult asthma patients were eligible for study enrollment. These included physicians and nurse practitioners. Adult asthma patients were eligible if they self-identified as Black, had been prescribed an ICS in the prior 12 months, had uncontrolled asthma as assessed by the Asthma Control Questionnaire (ACQ)14,15 and reported erroneous asthma and/or ICS beliefs. Patients who were non-English speakers or who had serious mental health conditions, as determined by the PCP, were excluded.
The ACQ is a widely-sued validated 6-item survey that uses a 7-point Likert response scale (positive predictive value = 88% in identifying uncontrolled asthma in clinical trials) 14 to measure nighttime and daytime symptoms, breathlessness, wheeze, activity limitations, rescue medication use; and reported as a mean (range 0–6). A score of 1.5 or higher indicates uncontrolled asthma; lower scores indicate better control.
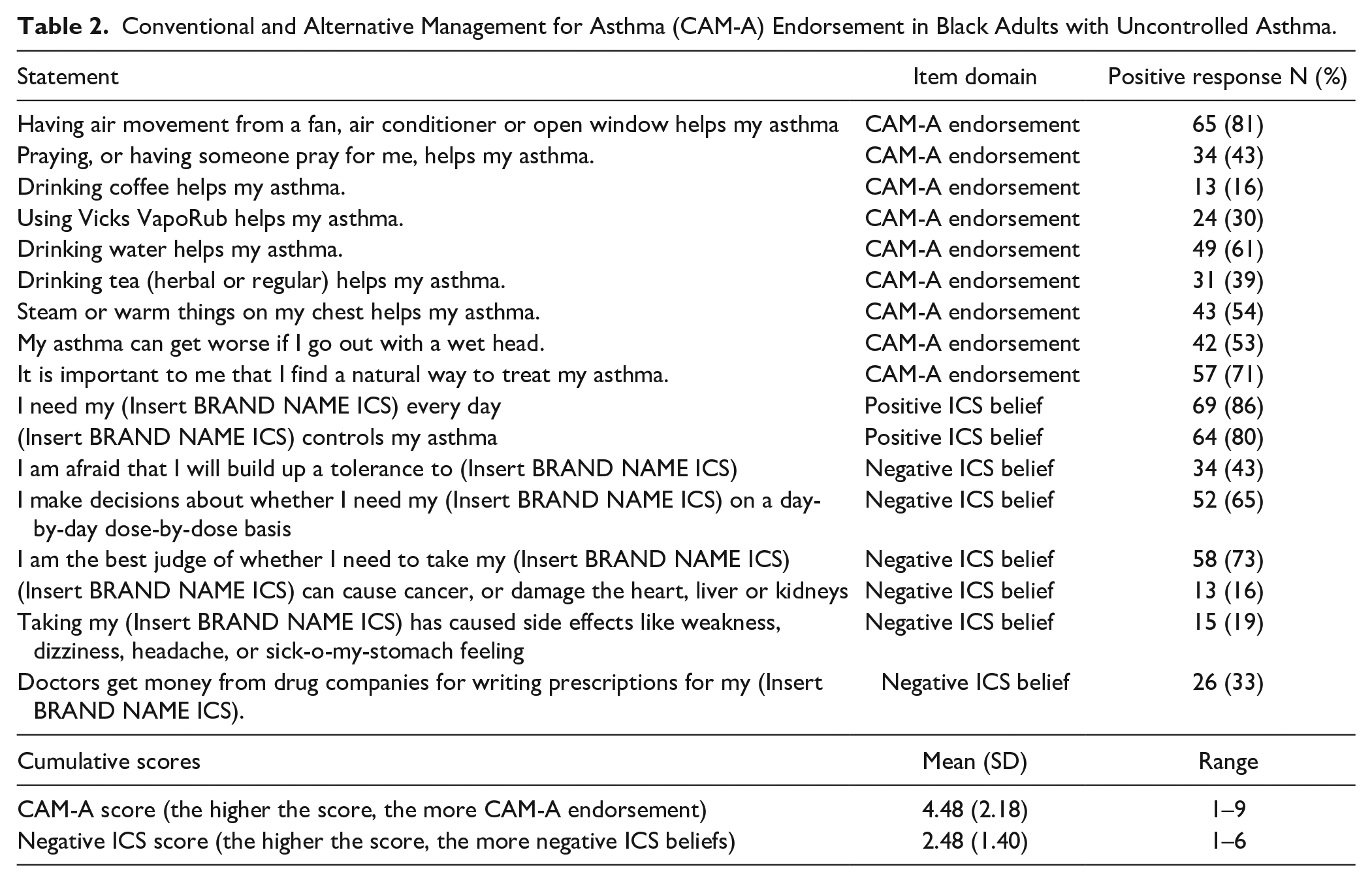
Data collection occurred from December 2017 to February 2019. Patients self-reported their ICS adherence on the Medication Adherence Report Scale for Asthma (MARS-A), a 10-item instrument (5-point response scale) with high reliability (Cronbach’s alpha = 0.85). 16 Self-reported adherence was calculated as the average of the 10 questions. Higher self-reported adherence was defined as a MARS-A score of 4.5 or higher. Patients were asked to complete the Conventional and Alternative Management for Asthma (CAM-A) 10 a 17-item tool to measure ICS beliefs (Cronbach’s alpha = .79) and CAM-A endorsement (α = .77). We calculated a cumulative CAM-A score (the higher the score, the more CAM-A endorsement) and the cumulative negative ICS score (the higher the score, the more negative the ICS beliefs).
At each clinic visit, study staff set up 2 audio recorders, left the room and collected the recordings at visit completion. Audio recordings were transcribed verbatim. Inductive data analysis was performed using adapted grounded theory methodology. 17 Two team members (AN, AB) independently listened to the audio recordings to gain an overall understanding of the content being captured during the patient visit. Each recording was then inductively coded through an iterative process where codes were “chunked” into categories and subsequent emergent themes. Emerging thematic findings were discussed at weekly meetings until consensus on coding and interpretation was reached. A third team member (MG) reviewed findings. Emergent themes were cross-checked to ensure consistency across data sources, coherence of domains, and to assess for any variation in findings.
Rigor
We used several strategies to maximize trustworthiness and minimize bias associated with the analysis of the qualitative data. 18 Two team members coded data independently and subsequently reviewed categories until agreement was reached. A third team member served as a peer reviewer to determine plausibility of findings and uncover potential biases. Using multiple coders working independently allowed for triangulation of a strategy to address concerns about the credibility of a study’s finding. 19 We also purposively sampled Black adults with persistent asthma, fostering transferability. 20 Dependability and confirmability criteria were met by the creation of an audit trail documenting data collection and analysis decisions.
Ethics
This study was approved by the Columbia University and University of Pennsylvania Institutional Review Boards. Informed consent was obtained by a member of the research team in person prior to the patient visit.
Results
Eighty Black adult participants were enrolled. Most were female (83%) and government insured with 98% reporting Medicaid, Medicare, social security disability or being dual eligible (Medicaid/Medicare). Mean age was 45 years (SD 13). (Table 1). The 10 PCPs that participated in the study consisted of 4 NPs and 6 physicians across the 2 clinical practice sites. Half of the PCPs had less than 4 years of practice experience and 40% of PCPs saw more than 30 patients with asthma each month. The clinical visits ranged from 8 to 28 min. The CAM-A endorsements are found in Table 2.
Participant Demographics and Baseline ICS Adherence.

Abbreviations: ACQ, asthma control questionnaire; MARS-A, medication adherence report scale for asthma.
ICS adherence (N = 23) noted at or above the 4.5 score threshold.
Conventional and Alternative Management for Asthma (CAM-A) Endorsement in Black Adults with Uncontrolled Asthma.
Three themes emerged from the qualitative analysis of the audio-recorded visits: (1) ICS misuse and lack of knowledge; (2) external influences yielding personal misconceptions; and (3) patient-provider communication to individualize plan of care (Table 3).
Thematic Findings of Barriers and Facilitators to ICS Adherence in Black Adults with Uncontrolled Asthma.

Abbreviation: ICS, inhaled corticosteroid.
ICS Misuse and Lack of Knowledge
Various knowledge deficits were identified including incorrect ICS use (eg, frequency of dosing) and a failure to connect ICS non-adherence with uncontrolled asthma. A 45-year-old female said, “I didn’t know that it is prescribed for twice a day. I just use it when I am short of breath. Other times I go through an inhaler a day.” Similarly, another patient said, “I only take it when my body says I’m going to fall over, and I can’t breathe.” Many patients reported being unable to differentiate between ICS and quick-relief medications, were confused as to the prescribed frequency of doses, were skeptical about the necessity of regular ICS dosing, and signs of an exacerbation. One newly diagnosed patient failed to properly use her ICS for control and expressed frustration when her short acting relief inhaler did not resolve her symptoms. “I was taking my albuterol up to 8 times a day and nothing was helping until I ended up at the hospital.” This confusion was not limited to patients with newly diagnosed asthma. A patient with a 28-year asthma history admitted, “I don’t usually take my [brand name ICS] until I take the albuterol a few times and see if it slows down [my symptoms]. If not, then I take it.” Some patients were unfamiliar with how to recognize worsening asthma symptoms. “I just keep coughing. I’m always catching a cold.” Unfortunately, for many patients a severe exacerbation requiring hospitalization was the necessary incentive to understand proper ICS use and asthma management. “The exacerbation made me insecure [about asthma management] . . . an eye-opening experience,” said 1 patient.
External Influences Yielding Personal Misconceptions
Patients voiced suspicion of their prescribed medication, including its effects on their overall health and their provider’s intent when prescribing the medication. Several patients acknowledged that their ICS misuse and non-adherence was due to concerns about building up a resistance to the medication’s salutary effects. A female (aged 20) with a long history of asthma said, “the more you take something you get immune to it. That’s why they kept upping my asthma medication.” Other patients were concerned that ICS use weakened their health. “I think I started getting pneumonia from [brand ICS]. Every time I take it, I get sick.”
Suspicions were reinforced by content seen on television and websites. Online information prompted fear of side effects or suspicion that a provider was financially incentivized to prescribe ICS medication. One 49-year-old with a recent diagnosis of asthma explained, “I see all these medicines on TV. This causes this and that one causes gangrene. I rather go through what I have than risk that.” A 58-year-old said, “What are they doing to us? I asked Google and YouTube and then watched a video all about it [side effects].” A 50-year-old told his provider, “that’s what you hear on the news all the time, you [provider] write a prescription, you get paid.” Another participant similarly expressed distrust saying, “[ICS brand name] is only prescribed by companies to make money.”
Patient-Provider Communication to Individualize Plan of Care
One recurring discussion between patients and providers focused on leveraging patient’s individualized preferences and home environment to improve ICS adherence. This involved mitigating negative beliefs or misunderstandings such as concerns about PCPs being paid by industry for writing prescriptions, side effects seen online or in television advertisements, the role of complementary and alternative therapies, or confusion about ICS versus quick-relief medication. For example, a female patient expressed she was “scared of the side effects she heard on tv.” The physician took time to explain, “I understand where you are coming from. I will tell you that the side effects of the inhalers are minimal, and the risk of uncontrolled asthma is a lot worse.”
Providers also engaged in tailored goal setting for improved ICS adherence and healthy lifestyles. For example, a NP asked, “How can we improve this [ICS use] in the future for you?” and “What techniques are you going to use at home as a reminder to take your inhaler the same way and time each day?” Questions about individualized ICS adherence plans prompted both patients and PCPs to determine what strategies would be most effective. One patient said, “I always have my cell phone with me.” Her PCP responded, “In that case, why don’t we set up an alarm that goes off on your phone at the same time every day to remind you to take your medicine.” Another patient decided to take her ICS when she administered her grandchild’s inhaler.
PCPs also inquired about the patient’s home environment and plans for avoidance of environmental asthma triggers. One physician inquired when a patient’s asthma worsened in her home and determined that it was in the evening when she was in her bedroom. After further prompting, the patient reported that she had multiple pets sleeping in her bedroom despite her dog and cat allergy and expressed reluctance to removing the pets. This prompted the physician and patient to create a plan to keep the pets out of the bedroom. The patient responded saying, “I’m not giving up my pets, but I didn’t know I can do things to help not get so sick from being around them.”
When additional consults with outside providers were warranted, PCPs often inquired about a patient’s preference for location and hospital affiliation. “If for some reason you needed to get to a hospital or be hospitalized, which hospital is easiest for you to get to and which 1 do you prefer?” The preferred hospital of a patient prompted the PCP to refer to an asthma specialist affiliated with that practice. PCPs further inquired about transportation access and ability to travel to specialist appointments to eliminate patient burden. One patient said, “It’s much easier for me for jump on the bus and go across the city to that location than find a ride to an office downtown.” Finally, PCPs prompted discussion about caregiver and family involvement in the patient’s asthma management. One patient mentioned that she was motivated by a desire “to be able to play with the kids outside without getting short of breath. I need to keep up with them.” Another patient talked about relying on her adult children for follow-up care, “My daughter takes me to all my appointments. If she can’t go, I can’t go.” Almost all visits resulted in a verbalized agreement with the plan of care and targeted goals individualized to fit the patient’s educational and psychosocial needs.
Discussion
This study examined the types of conversations that patients and PCPs have when asthma is uncontrolled. It was evident that many patients lack knowledge about correct ICS use, including its purpose, appropriate frequency, and potential side effects. Our findings illuminate how crucial it is to inquire about ICS dosing and frequency regardless of the number of years since diagnosis or ICS initiation. There is a substantial body of evidence about the importance of patient education on asthma management.21-23 Unfortunately, education is poorly reimbursed and primary care visits are too brief to support the type of tailored education that patients may require. This is an important target for payers and policymakers to consider if the gap in asthma outcomes for Black adults is to be narrowed.
The second theme to emerge, external influences influencing personal misconceptions, demonstrated how vulnerable patients are to external influences such as direct-to-consumer (DTC) ads and the internet. Recent research indicates that patients receive conflicting information from commercials when their medications are widely advertised. 24 Until now, the influence of external sources such as DTC ads and media have not previously been reported in regards to ICS non-adherence. This finding is alarming and consistent with existing evidence that suggests drug commercials contribute to poor medication adherence due to patient fear of medication side effects and potential problems their providers might not have disclosed. 25 Considering the extent to which Black patients distrust the medical systems due to their experiences with institutional racism, 26 the potential for DTC advertising to exacerbate this distrust cannot be overstated. Moreover, erroneous beliefs about providers being incentivized to prescribe inhalers must also be addressed. By actively discussing patient’s fears, providers may be able to disabuse patients of erroneous beliefs that could present potent barriers to ICS adherence and proper asthma management.
Our findings also highlighted the need for effective patient-provider communication to individualize a patient’s plan of care. The ability of providers and patients to develop partnerships over time that are patient-centered and involve more shared decision-making shows promise to improve ICS adherence and subsequently improve asthma management. As seen in our study, when providers inquired about individual patient fears, psychosocial needs, and lifestyle, patients were likely to agree to a mutual plan of care. There is a growing body of evidence that shared decision making improves asthma outcomes. 27 Less is known about the utility of shared decision-making in diverse adult populations with asthma. More research is therefore warranted to answer these important questions. Previous literature has noted that shared decision making is often difficult to not only conceptually define but to measure. 28 Our grounded theory approach to investigate care delivery in this study allowed us to assess shared decision making from an observer perspective. Since there is no gold standard for the measurement of shared decision making, 29 more research is needed to validate observer measurement in comparison to patient or provider perspectives during a patient visit.
Study Limitations
The collection and analysis of audio-recorded visits in real-world settings provides the ability to capture unique data about the provider-patient interaction. However, it is likely that the presence of the digital recorders had a Hawthorne effect prompting participants to be their “best” communicators. Still, this unique approach presented advantages to understanding the patient-provider interaction and related content during asthma care discussions. Similar to simulated patient-provider encounters that are increasingly being used to enhance the delivery of patient-centered care, 30 audio-recordings of real-world interactions may inform future research focused on the development and testing of tailored interventions to increase medication adherence. In addition, our findings may be unique to clinical encounters between Black (mostly female) adults with uncontrolled asthma and their primary care providers; future research should include a diverse population by age, sex, race ethnicity, and practice settings.
Conclusion
This research revealed common themes that help to explain suboptimal ICS adherence among Black adults with uncontrolled asthma. While it is evident that more asthma education is needed generally, we specifically identified DTC ads and online source as contributing to distrust that undermines ICS adherence and are important new targets for future interventions aimed at increasing ICS adherence. Providers should address misconceptions about the goals of treatment, side effects, and purpose of prescribed medications as a critically important first step to increasing ICS adherence which may have the significant effect of narrowing health disparities experienced by Black adults with asthma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Center for Advancing Translational Sciences, National Institute of Health (grant number TL1TR001875) and National Institute of Nursing Research, National Institutes of Health (R21 NR016507).