
Abstract
Background and Purpose:
Acute viral respiratory infections (ARTIs) are among the most common reasons for a healthcare encounter throughout the industrialized world. Among the approximately100 million antibiotic prescriptions written every year for ARTI, half are prescribed inappropriately. Inappropriate antibiotic prescribing for viral illnesses poses a serious threat since many organisms have become resistant to commonly used antibiotics. The aim of this study was to develop an ARTI treatment protocol in accordance with current practice guidelines to decrease the number of inappropriately prescribed antibiotics in a primary care health clinic.
Methods:
Patient subjects were obtained using convenience sampling and data collection was completed using ICD queries in the clinic’s EHR system. A retrospective chart review analyzing antibiotic prescribing practices was conducted pre- and post- implementation of an educational session detailing current ARTI practice guidelines.
Conclusions:
The results of this project showed clinical significance in that clinician education, focused on ARTI current practice guidelines and attentiveness in antibiotic prescription practices, reduced antibiotic use for viral ARTIs by 12.0%.
Implications for Practice:
Clinician education and implementation of current practice guidelines for ARTI will assist clinicians decrease both the unnecessary adverse effects of antibiotics, as well as the threat of antibiotic resistance.
Keywords
Introduction and Background
Acute viral (upper) respiratory tract infections (ARTIs) are among the most common reasons for a healthcare encounter in the United States, with over 43 million ambulatory visits yearly for cough or sore throat. Most of these episodes are caused by viruses, and in otherwise healthy individuals, these infections are typically short-lived and resolve without any intervention except for supportive care at home. 1 Despite the resolution of these illnesses with mostly supportive care, millions of patients continue to be seen by healthcare providers and have antibiotics prescribed inappropriately and against current treatment guidelines. 2 ARTIs are defined as several conditions caused by multiple families of viruses, which include the common cold, rhinosinusitis, pharyngitis, and acute bronchitis. Most ARTIs are self-limiting and involve a variable degree of symptoms, including nasal congestion and discharge, sneezing, sore throat, cough, low-grade fever, headache, and malaise. Among healthy adults over 65 years of age, ARTIs account for hundreds of millions of days of illness and work loss, tens of millions of healthcare professional visits and antibiotic prescriptions, and billions of dollars in health care and lost productivity costs. 1
Many patients with ARTIs seek care in the emergency department or the primary care office where inappropriate antibiotic prescribing is common among healthcare providers. Among the approximately 100 million antibiotic prescriptions written every year for ARTIs, half are prescribed inappropriately for nonbacterial infections or for groups of symptoms not necessitating antibiotics. 3 Antibiotic prescribing for viral illnesses is ineffective and poses a serious threat both nationally and globally since many organisms have become resistant to commonly used antibiotics. The Center for Disease Control (CDC) and the World Health Organization (WHO) consider antibiotic-resistant bacterial infections one of the biggest public health threats and predict a day when antibiotics will no longer be useful for treatment of commonly cured and serious bacterial infections. In the United States, at least 2 million antibiotic-resistant illnesses and 23 000 deaths occur each year at a cost to the US economy of at least $30 billion. 3 Prescribing antibiotics to patients when they are not indicated also puts patients at risk for unnecessary side effects, such as headache, thrush, abdominal pain, nausea, vomiting, and diarrhea, as well as more serious complications, such as allergic reactions, clostridium difficile infections, and anaphylaxis. 1
Symptomatic therapy remains the mainstay of viral ARTIs. Symptoms for most people are self-limited and require no intervention. 4 The American College of Physicians and the CDC have released new clinical guidelines on antibiotic use in adults with acute respiratory tract infections. These guidelines state that providers should apply strict criteria to determine when antibiotics are needed and that antibiotics should not be routinely used to treat healthy adults with ARTIs at outpatient clinics. The guidelines, which cover patients with bronchitis, suspected Group A streptococcus, acute rhinosinusitis, and the common cold, should serve as a guide for outpatient healthcare providers to promote the recommended use of antibiotics for healthy adults with ARTIs. 2 Many patients with uncomplicated, self-limited ARTIs seek care in an emergency department or primary care office, which subsequently increases healthcare costs and often leads to an inappropriate antibiotic or antiviral prescription. 1
Deviation from best practice can include clinician perception of patient expectations for antibiotics, perceived pressure to see patients quickly, fear of failure to treat, or clinician concerns about decreased patient satisfaction with clinical visits when antibiotics are not prescribed. Clinician education to reinforce guidelines has been shown to increase their use and reduce the number of inappropriately prescribed antibiotics. Effective clinician education often includes reviewing guidelines for appropriate antibiotic prescribing while also addressing the psychosocial pressures that influence antibiotic prescribing practices of clinicians. 3 A recent study explored the application of standard treatment guidelines, which included information on providers’ knowledge and attitudes toward standard treatment guidelines and analyzed the effect of different levels of provider educational training before practice change. 5 Educational training has a positive impact on clinicians’ attitudes toward the change in practice as well as their current practice and environment. The participants’ positive perception of the change in practice helped promote further use of treatment guidelines, which led to increased patient satisfaction and improved outcomes.
The literature search confirmed that current guidelines in the management of an uncomplicated respiratory infection suggest avoiding the use of antibiotics. There is substantive evidence on strategies used to decrease inappropriate use of antibiotics when faced with the large influx of patients seeking care for an ARTI. The aim of this study was to develop a clear and concise ARTI treatment protocol according to current practice guidelines and provide an educational intervention for providers to decrease the number of inappropriately prescribed antibiotics in a primary care health clinic with a future impact outcome of decreasing antibiotic resistance in the community.
Methods
Design
A retrospective chart review was conducted to access medical records of patients at a primary care practice. A pre-post analysis was used to compare provider prescribing before and after an implementation from December 1, 2018 to March 1, 2019 (the time when a higher percentage of patients with viral illnesses are seen). The pre-implementation chart review was conducted over the same period 1-year prior for comparison. International Review Board approval was received with exempt status (HUM00100431).
Setting
This project was implemented in an internal medicine and pediatric practice in a small suburb in the Midwest. The primary researcher was a practicing provider at the site during implementation, and providers at the site determined that this quality improvement project would be beneficial to the site and its patients. This primary care clinic consists of 1 physician and 1 nurse practitioner, as well as 5 office staff. The clinic sees both children and adults and accepts a large variety of insurance types, including Medicaid, Medicare, and private insurance. The clinic did not have a prior ARTI protocol in place. As with most primary care clinics, these providers see a high volume of patients with viral respiratory infections throughout the year, but especially during the fall and winter months.
Sampling
Convenience sampling was utilized for this study, as the site was known to the university and a contract for precepting was already in place. Data collection was completed using ICD queries in the clinic’s EHR system. Included were any encounters from adult patients treated at the primary care clinic age 18 or older with a diagnosis of an acute respiratory illness diagnosis. ICD 10 codes included in the study were acute bronchitis (J20.9), acute bronchiolitis (J201.9), acute nasopharyngitis (J00), acute laryngitis (J04.0), acute laryngopharyngitis (J06.0), acute upper respiratory infection unspecified (J06.9), and acute pharyngitis unspecified (J02.9). Excluded from the project were any encounters from patients under age 18 and those over 18 who had a diagnosis where evidence-based practice supports use of antibiotics for treatment. Diagnoses excluded were acute sinusitis (J01), pneumonia (J15.9), acute tonsillitis (J03.9), and streptococcal pharyngitis (J02.0). Also excluded was any patient with a previous recorded diagnosis of emphysema (J43), chronic bronchitis (J42), bronchiectasis (J47), COPD (J44.9), cystic fibrosis (E84.0), or interstitial pneumonia (J84.11). Due to the above diagnoses having a more likely probability of disease complications requiring antibiotics, they were excluded. 6
Implementation
The acute viral respiratory infection protocol pilot was developed by the authors utilizing current recommendations by the CDC, American College of Physicians, US Department of Health and Human Services and recent pertinent studies. These guidelines were reviewed, and the flowchart and protocol were created with key components of all the sources incorporated. The flowchart and protocol were reviewed multiple times with revisions suggested by 2 practicing primary care providers who are also both educators of primary care clinicians in large residency and university-based programs. The flowchart and protocol were created for use by providers to reinforce current guidelines. The researchers did check in a couple of times with the providers at the clinic site and were given the feedback that the ARTI protocol was efficient to use from the providers perspective.
The provider educational program included a series of educational e-mails before the implementation of the project detailing the project aim, objectives, and key dates for project implementation and completion as well as a live educational presentation meeting. During the live meeting, an overview of current ARTI guidelines with the providers helped reinforce the providers’ comprehension of the protocol. A laminated pocket-sized copy of the ARTI protocol (Figure 1) was distributed during the educational meeting.
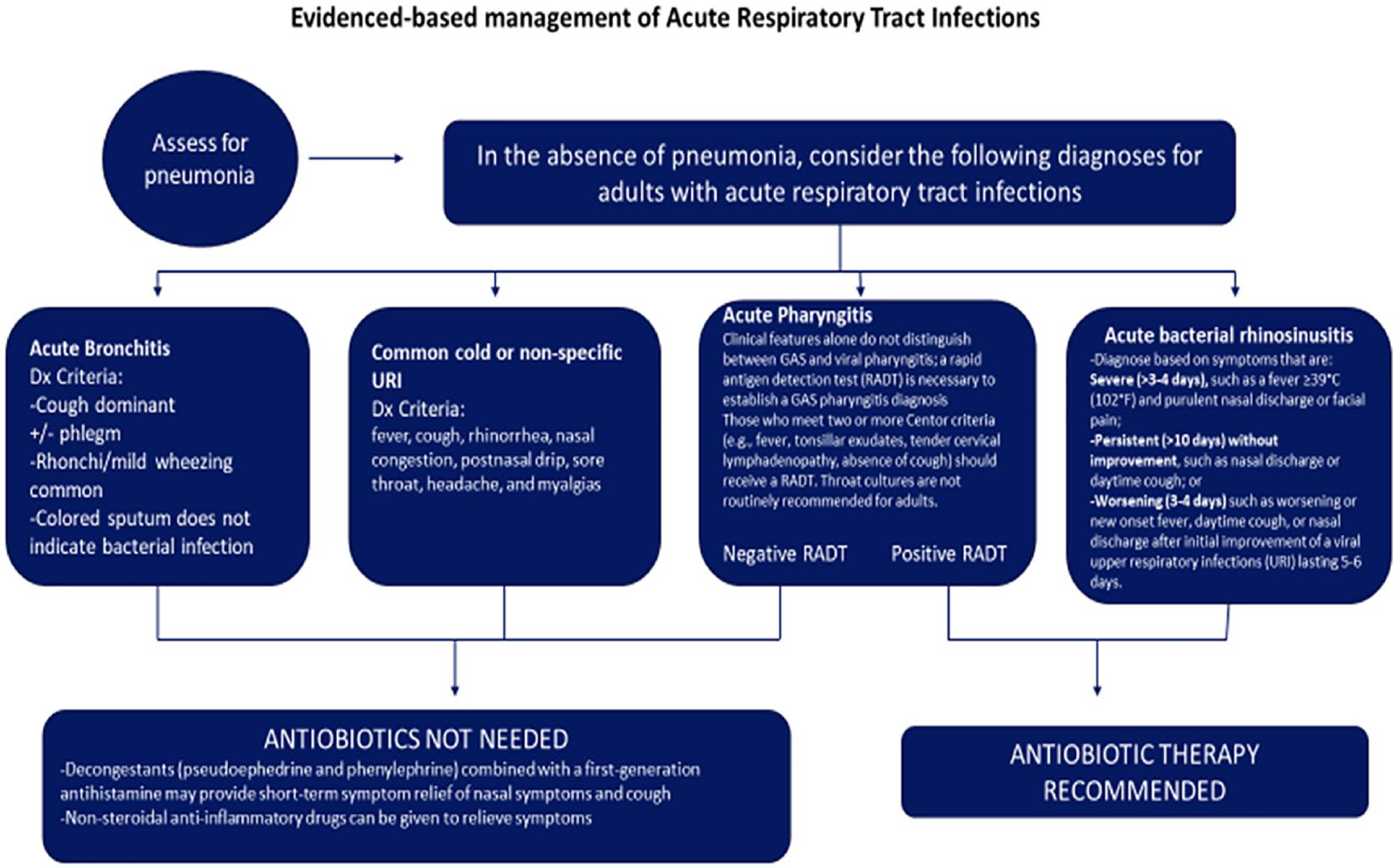
ARTI protocol given to providers.
Data on antibiotic prescribing practices was collected for 8 weeks. Retrospectively, similar data was collected in the prior year for the same 8 weeks. Antibiotic prescription practices between pre- and post-intervention were compared for a change in proportion using chi-square analysis. Additionally, subgroup analysis explored if there was a change in antibiotic prescription practices by key demographics (age group and gender) before and after the educational intervention using a chi-square analysis. Finally, chi-square analysis was used to compare subjects before and after the education intervention on key demographics. 7
Results
A total of 71 patients were eligible for the analysis and included 35 patients in the pre-implementation period and 36 patients in the post-implementation period. There was no difference in demographic characteristics between the pre- and post-implementation periods (Table 1).
Comparison of Demographic Variables between Pre- and Post-implementation Periods.

Abbreviation: SD, Standard deviation.
The mean age for the pre-implementation period was 46.29 years with a standard deviation of 19.93 years. The mean age for the post-implementation period was 48.14 years with a standard deviation of 18.57 years. There were no significant differences in age between the 2 groups (t = 0.41, df = 69, P = .69). There were 16 men (45.7%) in the pre-implementation period and 19 women (54.31%). There were 9 men (25%) in the postimplementation period and 27 women (75%). Degree of association was measured by chi square test, with significance level set at P = .05. There were no significant differences in gender distribution between the pre- and post-implementation groups (Pearson, P = .068). To accurately compare the groups, it was important to provide a subgroup analysis of age and gender. The groups were without significant variations in these areas.
While 7 viral illness diagnoses were included in the project, only 5 were seen in the chart audit and included acute sinusitis (J01), pneumonia (J15.9), acute tonsillitis (J03.9), and streptococcal pharyngitis (J02.0) (see Comparison of diagnoses between pre- and postimplementation periods Table 2). There was no significant difference in the diagnosis breakdown between the pre- and post-implementation groups (Pearson, P = .066). Two clinical providers saw the patients in the pre-implementation period and the same 2 providers in the post-implementation period (see Comparison of providers between pre- and postimplementation periods). There was a significant difference in the providers between the 2 time periods (Pearson, P = .023). Eleven antibiotic prescriptions (31.4%) were given to patients in the pre-implementation period, while 7 antibiotic prescriptions (19.4%) were given to patients in the post-implementation period. There was no statistically significant difference in antibiotic prescriptions between the 2 groups (Pearson, P = .246) (Table 3).
Comparison of Diagnoses between Pre- and Post-implementation Periods.

Number and Percentage of Antibiotics Prescribed for Viral Illness Diagnoses by Provider.

Discussion
The purposes of this project were to improve provider knowledge and develop an ARTI treatment protocol to decrease the number of inappropriately prescribed antibiotics in a primary care health clinic. The pre- and post-implementation groups were similar in age, gender distribution, and diagnosis, with no significant differences between these groups, thus the results effectively represent similar groups.
The clinicians at this primary care health clinic decreased their prescribing of antibiotics for viral illness diagnoses by 12.0%, a decrease of 4 prescriptions written in the postimplementation group. While this decrease was clinically significant, it was not statistically significant. Several reasons could account for the lack of significance. The most likely factor was the small sample size considering the effect size. The differences between the diagnoses and providers in the 2 groups could also account for some of the lack of statistical significance in the antibiotics given.
When primary care providers (PCPs) adhere strictly to guidelines when treating patients with ARTIs, inappropriate antibiotic prescriptions can be decreased. 3 It was clear that provider education utilizing the ARTI was effective in positively impacting the provider prescribing for viral respiratory infections. What was not as clear was that the health status of the patients in the practice varied. For example, when the results of the study were discussed with the providers, it became clear that some of the patients were more vulnerable than others. One provider described prescribing antibiotics for a 73-year-old diabetic patient with bronchitis and a long history of pneumonia and smoking. Such intricacies are not depicted in the results but certainly occur in most primary care clinics. Inappropriate antibiotic prescribing was defined as writing an antibiotic prescription for a viral illness diagnosis. Unfortunately, many PCPs prescribe antibiotics inappropriately, despite knowing that prescribing guidelines exist. 8 In addition, it has been shown that variability in provider understanding and awareness of antibiotic stewardship impact inappropriate antibiotic prescribing.9
Other barriers that lead to a deviation from best practice can include clinician perception of patient expectations for antibiotics, perceived pressure to see patients quickly, or clinician concerns about decreased patient satisfaction with clinical visits when antibiotics are not prescribed. Clinician education has been shown to increase the use of clinical guidelines and reduce the number of inappropriately prescribed antibiotics. 3 Limitations of this study include the lack of randomization and the small sample size. Additionally, patient comorbid conditions that may impact the decision to prescribe were not measured nor were provider clinical acumen or the art of medicine in prescription decisions. Even using such clinical reminders, without rapid and accurate in-office testing to definitively discern viral from bacterial infection, antibiotic prescriptions for viral infections are likely to continue.
While the findings in this small pilot study are not generalizable in themselves, it is anticipated that the ARTI protocol and this study design can produce similar results in other clinics. Because study was completed using an easily replicable design, and documented ARTI protocol, it is anticipated that this study and the results could be transferable to other primary care settings. 10 Several other studies, many cited in this article have found similar outcomes with a clear decrease in antibiotic prescribing for ARTIs with increased provider education regarding practice guidelines and an increased awareness of antibiotic stewardship.1,3,9
Conclusion
Although not statistically significant, the results of this project are clinically significant and showed that clinician education focused on ARTI current practice guidelines and attentiveness in antibiotic prescription practices reduced antibiotic use for viral ARTIs by 12.0%. Additional studies with larger sample sizes will help validate the intention of this pilot study, which can be easily replicated at other primary care health clinics. Sustainability was addressed with continuing communication with the project mentor who is committed to maintaining the ARTI protocol as standard practice at this primary care health clinic. ARTIs are among the most common reasons for healthcare encounters worldwide with approximately 50 million antibiotics inappropriately prescribed per year. Clinician education and implementation of current practice guidelines can assist clinicians to decrease both the unnecessary adverse effects of antibiotics, as well as the threat of antibiotic resistant bacterial infections. In addition, it is also suggested that increased education and awareness of antibiotic stewardship for healthcare providers could be beneficial.
Footnotes
Acknowledgements
We would like to acknowledge Dr. Barbara Kupferschmid, Associate Professor School of Nursing, University of Michigan, Flint, for her assistance with data analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.