
Abstract
Purpose:
World Health Organization (WHO) defines intimate partner violence (IPV) as physical, sexual or psychological harm caused by an intimate partner or ex-partner. There are few studies describing interpersonal violence (IPV) among physicians. Our study describes IPV experienced by U.S. physicians.
Methods:
This was a multicenter survey administered to 4 physician groups in 2015 to 2016. In total 400 respondents returned survey results. Measures included current IPV, childhood abuse, mental health, professional role, and demographics.
Results:
IPV was reported by 24% of respondents. The most frequent abuses reported were: verbal (15%), physical (8%) followed by sexual abuse (4%) and stalking (4%). Logistic regression model found that IPV was more likely to be reported by older participants (aged 66–89), those who experienced childhood abuse, working less than full time, and had been diagnosed with a personality disorder. Women and Asian Americans reported slightly higher IPV rates.
Conclusions:
Our study has implications for both medical education and intervention development. Universal screening and education that addresses clinical implications when treating peers who experience IPV are needed. Workplace interventions that consider unique physician characteristics and experiences are needed, as well as programs that support sustained recovery. This is the first survey to our knowledge that confirms that physicians experience IPV at a rate consistent or higher than the national level. We developed a standardized instrument to assess IPV in male and female physicians at various career stages. We also identified significant predictors that should be included in IPV screening of potential physician victims.
Introduction
Intimate partner violence (IPV) is an increasing public health concern. 1 IPV impacts 1 in 4 women and 1 in 10 men in the United States, resulting in $3.6 trillion in costs over victims’ lifetimes. 2 The World Health Organization defines IPV as “behavior by an intimate partner or ex-partner that causes physical, sexual or psychological harm, including physical aggression, sexual coercion, psychological abuse and controlling behaviors.” 3 Early IPV research was often limited to serious physical injuries because many IPV statistics were derived from domestic abuse calls by law enforcement. 4 Many victims, however, did not acknowledge IPV as including controlling behavior, being undermined or being prevented to access their money.4,5 More current IPV research describes numerous abuser behaviors and relationship dynamics that contribute to physical, emotional, and social debilitation including verbal abuse and manipulation behavior. 5 More research is needed to understand the resulting couple dynamic and sense of demoralization that often occurs as a result of IPV. 4
IPV among physicians is seldom acknowledged or assessed.6,7 Physicians report IPV prevalence between 6% and 24% (women 7%-24%, men 6%-10%), but studies have limited generalizability due to lack of standardized and validated measures, small sample sizes, dated information, and sampling frames that combine child abuse plus partner abuse, or combine nursing, student, and physicians, or only survey women.8-12 Almost all physician IPV studies utilize self-report of self-defined partner or domestic abuse. 6
In a recent Australian study, female physician victims described significant stigma and shame from a sense of “professional defectiveness” by falling victim to IPV, which may contribute to low response rates in prior physician studies. 7 Studies of affluent women experiencing IPV reveal that they typically underutilize resources, and although they need psychosocial support, it is unclear what support will be most utilized or helpful.13,14 Physicians may be similar as a group and are also known to delay help-seeking and more data is needed to understand these issues in male physicians. 15
Screening and supporting IPV victims are critical physician responsibilities.16-19 It is reasonable that personal IPV experience has the potential to skew professional behavior by avoiding this sensitive topic with patients and impacted colleagues. 20 We do not yet understand the degree to which personal experience affects physicians. Physicians may have limited ability to provide whole person care for patients if they are preoccupied with their own experiences.6,21,22
The purpose of this study is to describe the experience of physicians, fellows, and residents who are, or have been involved, in an intimate relationship that is controlling and/or abusive. We also want to identify the characteristics or conditions associated with their IPV experience.
Materials and Methods
Study Design and Population
This was a multicenter survey administered to a convenience sample of 4 physician groups in 2015 to 2016. In total 400 respondents returned survey results. We used resident list serves in 2 states, an electronic medical journal advertisement in another state and a medical school alumni list serve representing a national sample. The Loma Linda University Institutional Review Board approved the study.
Survey Content and Administration
We developed a questionnaire as a largely descriptive instrument using methods outlined by Nelson and Allred. 23 Survey items were based on the authors’ teaching, psychotherapy experience, and IPV literature, deriving items from published literature wherever possible to improve validity. Table 1 presents survey items organized by type of abuse, consistent with the WHO IPV definition. 3 The survey was uploaded into Qualtrics (Provo, UT)® and pilot tested (n = 8) prior to distribution. As noted above, the survey link was emailed to 3 site administrators who shared it directly with their constituents and published in 1 electronic publication. The survey took approximately 15 minutes to complete.
IPV Variable Operationalization.

Measures
The following variables were included in the study to serve as potential predictors or correlates of IPV.
Data Analysis
We began analysis by evaluating IPV experience within the sample population. We examined IPV reports across demographic categories, professional status and previous history of childhood IPV. We applied chi-square comparisons to test for statistically significant differences between categories. Next we applied a forward likelihood ratio logistic regression model to assess the combined effect of predictive variables. SPSS 24.0 was used for both aims. 45
Prior to the planned logistic regression analyses, we evaluated for missing data and univariate assumptions. In regards to missing data, a listwise comparison across all variables in the analysis showed no more than 6.8% missing data. Therefore we used a listwise deletion prior to the logistic regression estimation. This reduced the final analysis sample to n = 373. The outcome variable was a binary measure of current IPV where 0 indicated no presence of IPV and 1 was given if any forms of IPV were noted by the respondent. Predictor variables were split into 4 planned steps. The first step included variables directly associated with the respondent (age, gender, presence of children in the home, ethnicity as well as a history of childhood abuse). For this step an enter method was used so that these demographic variables acted as a control for the rest of the model. The next steps were fit with a forward likelihood ratio method. The first step included the respondent’s current employment status as well as professional role (eg, physician, fellow, resident, retired, and administration). The third step included the respondent’s current partner relationship status (married, single, living together, etc.), and their partner’s professional role (e.g., physician, fellow, resident, retired, and administration). The final step included symptoms of mental health problems (e.g., depression, anxiety, suicidality personality disorder, etc.).
Results
Prevalence
Of the 400 respondents, 96 (24.0%) reported some form of IPV (see Table 2). The most frequent form of IPV was verbal abuse (14.8% of respondents). Physical (7.5%) was the next most common form of IPV followed by sexual abuse (4.0%) and stalking (3.8%). Asian Americans reported slightly higher rates of IPV (31.7%). Females and males both reported IPV with female reports being higher than male reports by 8.2%. Respondents who did not have a child living at home were significantly more likely to report current IPV, and individuals who are not currently in a relationship or who experienced childhood abuse were the most likely to report IPV. There was no notable difference between the various professional roles or work settings.
Prevalence of Intimate Partner Violence by Demographic Groups.
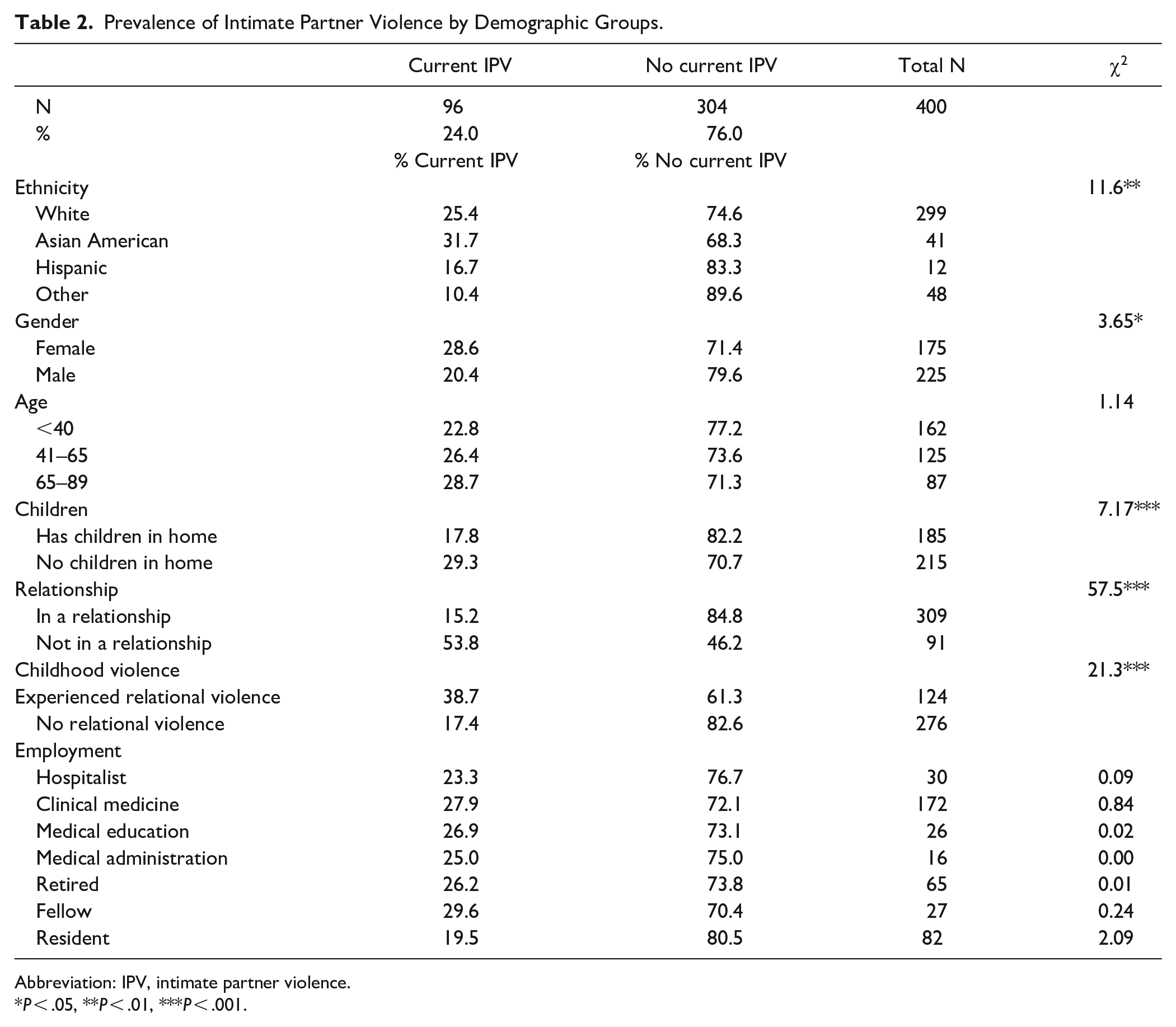
Abbreviation: IPV, intimate partner violence.
P < .05, **P < .01, ***P < .001.
Logistic Regression Models
Using the variables outlined in the methods section, a final logistic regression model was constructed (see Table 3). Given that first demographic block of variables was fit with the enter method, all variables are included in the model. For steps 2 to 4, only the statistically significant variables are presented in Table 3. In this model, individuals within a current relationship were significantly less likely to report current IPV. IPV was more likely reported by older age cohorts (ages 66-89), in comparison to younger cohorts (ages 18-40). Within the model, and after controlling for relationship status and age, the variables of gender, children in the home, and ethnicity did not significantly change the odds of current IPV. Rather, being a victim of childhood abuse, working less than full time and being diagnosed with a personality disorder significantly increased the odds of a respondent reporting current IPV.
Summary of Logistic Regression Analysis for Predicting Presence of Intimate Partner Violence.

Abbreviation: eB = exponentiated B.
Variables n.s. not reported in table include: partner’s professional role and level of employment, respondent’s professional role and other mental health symptoms.
P < .05. **P < .01. ***P < .001.
Variables that did not achieve significance in the model included: the partner’s professional role and level of employment, the respondent’s professional role and other mental health symptoms (e.g., depression, anxiety, suicidality, eating disorders, etc.).
Discussion
Our survey explored 2 research questions: What is the experience of physicians, fellows, and residents who are, or have been involved in an intimate relationship that is controlling or abusive and what characteristics or conditions are correlated with IPV experience? Results confirmed that 24% of physicians reported personal experience with IPV. Unlike many other physician IPV surveys to our knowledge, our sample reported psychological, physical, sexual abuse, stalking, and controlling partner behaviors. Our findings on physical and sexual abuse are similar to other national studies showing 22.3% for women and 14.0% for men reporting at least 1 IPV incident in their lifetime. 24 Our measures included controlling relationships and emotional abuse, unlike most national studies. Physicians also reported subsequent relationships marked by IPV (7%).
Results indicated that female physicians experienced more IPV than men. This is consistent with national studies showing IPV affects 1 in 4 women and 1 in 10 men in some form or another.24,46 Children in the home may increase vulnerability to IPV, both because child caring responsibility may fall more to women, who may delay taking action to leave out of desire to protect children. 39 Some qualitative studies have implied that this might be true, but our results did not necessarily support this issue indicating more research is needed. 47 Our model indicated that part-time employment is also a predictor of IPV. This is consistent with studies linking unstable or lack of full-time employment to increased risk of IPV injury, which was also more common for women. 48
Our model identified early childhood abuse as a significant predictor of reporting IPV later in life. This finding is supported by several studies.49-51 Narayan et al. found that exposure to inter-parental violence during infancy and preschool was correlated with reported IPV at age 23. 50 Afifi et al. found that even a lower “threshold” of harsh punishment in childhood was linked to higher victimization as adult. 51 There is a need to screen for early exposure to violence in all patients, and physicians are not immune from these risks.
Study results showed that being older (65-89 years of age) was a significant predictor among physicians. This finding is inconsistent with a large US study whereby the biggest age group reporting IPV was 18-24. 24 Recent studies, however, have documented a growing trend in IPV among the elderly. 52 We speculate that while physicians are not immune to experiencing IPV, the stigma related to reporting is so strong that it may suppress reporting until physicians are more established or even retired from their careers. Haselschwerdt and Hardesty discussed this stigma in their study of IPV in affluent communities. 14 Women of affluence described a “secrecy management process” rooted in “shame, self-blame for their choice of husband and the violence, fear for their own and their children’s safety. . .not wanting to burden others with their ‘personal problems’” (p. 563). 14 Lifetime IPV prevalence is highest in populations with incomes below the poverty level; however, the group with the third highest IPV prevalence is from the highest income brackets. 52
Our findings also varied from the general population regarding race in that race/ethnicity was not predictive. Hispanic IPV prevalence is between 30% and 34% and Asian/Pacific Islander prevalence between 14% and 18%. 53 In a more recent study, Hispanics were the third highest prevalence to report IPV to police, after Whites and Blacks. 54 However, that study combined Asian Americans, Native Americans, and biracial participants into 1 category; prevalence of Asian American victimization was unknown. It is unclear why Hispanic physician prevalence is lower than Asian American physician prevalence in our data. More research is needed to understand how stigma within cultural contexts affects lived experience and potential correlation of socio-economic and minority status in earlier studies.
IPV odds increased for physicians reporting a history of personality disorder. Personality and mental health disorders are well-documented predictors of IPV perpetrators but few studies examine the relationship for victims.55-57 Willie et al. found that adverse childhood events (ACEs) directly predicted IPV severity in women as well as depression and post-traumatic symptoms. 58 This highlights the need to support physicians carrying both mental health challenges and IPV victimization.
Our study has implications for physician training. We hypothesize that many medical trainees do not identify IPV as a public health issue for physicians who may be their future patients. Physicians should be taught efficacious screening models and the implication for applying those models to their peers.6,18 Interactive case studies about physician IPV should be offered to all residents, such as is provided by the American College of Surgeons. 59
Physician struggles with IPV certainly influences ability to deliver patient care. 60 We only begin the discussion of how to help physicians effectively treat patients while tormented by events at home. To our knowledge, few resources exist that address these unique concerns. Workplace interventions are needed to support physicians while protecting their license, reputation, and physical/emotional safety. Physicians also need to understand that domestic abuse shelter helplines and personnel offer education and encouragement, including attorney recommendations and ways to improve personal safety.
Our findings indicate that both men and women physicians experience IPV. Strengths of the study include development of a standardized instrument to assess IPV and the inclusion of physicians at various career stages from more than 1 institution. Our study also asked about specific experiences and did not rely on just 1 IPV measure or participant definition. Limitations include self-report, which may have led to under-reporting due to non-response bias which limits generalizability of our results. 61 We included men in our sample; however our study did not specifically assess the experiences of transgender or same-sex relationships.
Continued research is needed to describe the experience of physicians in order to identify ongoing needs to develop appropriate interventions.
Conclusion
IPV is a seldom discussed but salient public health concern for physicians. We hope this study improves recognition that physician IPV is an unfortunate but common threat to physician wellbeing. Continued research is needed so that physicians are not relegated to silent suffering while they care for the wellbeing of their patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.