
Abstract
Objective:
Aim of this survey was to assess the prevalence of cardiovascular diseases (CVD) risk factors and attitude toward self-risk assessment among cardiac care physicians (who did not have CVD history), at a tertiary care cardiac center in Pakistan.
Design:
In this survey we included cardiac care givers who had a minimum of 1 year of working experience in a cardiac care center.
Participants:
Participants with self-reported history of established diagnosis of CVD were excluded. Face-to-face interviews were conducted with the help of a structured questionnaire which consisted of demographic information, data regarding established CVD risk factors, self-awareness, and attitude toward CVD risk assessment.
Results:
A total of 126 participants were interviewed, out of which 20.6% (26) were females and mean age was 36.1±7.6 years. The most prevalent CVD risk factor was family history of CVD (33.3%) followed by smoking (14.3%) and 23.8% had body mass index of ≥27.5 kg/m2. Around 23% of the participants did not know their cholesterol levels, similarly more than 74% were not aware of their high-density lipoproteins levels. More than 76% had never assessed their CVD risk and more than 37% don’t know or don’t have any opinion about their own CVD risk.
Conclusions:
The present study reveals low prevalence of conventional cardiac risk factors and marginally higher tendency of modifiable risk factors, such as smoking and obesity, among the cardiac physicians. A large proportion of these cardiac physicians have not yet assessed their CVD risk.
Introduction
Healthcare workers act as role models for a healthy lifestyle among the general population and are largely responsible for inspiring suitable lifestyle changes affecting the prevention of these diseases.1,2 Research shows a strong relationship that exists between decisions made by healthcare workers and diagnosis/treatment made to their patients. 3 Preventing cardiovascular disease and other related metabolic risk factors among healthcare workers is therefore an important strategy for achieving a healthy workforce both in the work environment and in the society they live in. 4
The epidemiologic studies in different regions of the world show a significant difference in morbidity and mortality due to CVD. Certain risk factors are more common among certain population. With the implementation of strategies for identification and prevention of risk factors, such as hypertension, diabetes, hyperlipidemia, and particularly tobacco smoking, the Western states have shown a declining trend. However, there seems to be an increasing trend in prevalence of CVD in Asian and African countries. 5
Taking into account the health-related knowledge available to hospital workers and their easy access to healthcare provision, it is believed that the incidence of cardiovascular diseases and their modifiable risk factors would be comparatively low.1,6 However, certain risk factors associated with work, such as long shifts, mental and physical stress, which classify the hospital’s atmosphere and place health workers in a high occupational risk category for certain illnesses. Most of the time, cardiac physicians have a busy work schedule. They have an imbalanced work life making their lifestyle usually sedentary. Additionally, many of them have never assessed their cardiovascular risk. All of these factors contribute to the deteriorating and obese conditions in the cardiac physicians. 7
Therefore, it is important to find out the cardiac risk, in order to form and implement certain changes to reduce CV risk among health care professionals. 8 As far as we know, no study assessing the CV risk profiles of Pakistani cardiac physicians in tertiary care hospitals has been conducted. Therefore, the aim of this survey was to assess the prevalence of cardiac risk factors and attitude toward self-risk assessment among cardiac care physicians (who did not have a CVD history), at a tertiary care cardiac center in Pakistan.
Methods
The study was conducted at the largest tertiary care cardiac center of Pakistan, with more than 400 cardiac health care physicians who provide acute and specialized cardiac care to >0.78 million patients annually, after approval of the institutional ethical review board, the study was completed in 6 months from October 2019 to February 2020. The potential population were MBBS qualified cardiac care physicians who had a minimum of 1 year of working experience after training. Participants were recruited in the study from doctors’ office using non-probability convenient sampling technique. Participants with self-reported history of any cardiac related surgery or intervention or under treatment for any established diagnosis of cardiac disorder (valvular, ischemic, congenital, or etc.) were excluded from this study and a total of 126 cardiac care physicians were included. Prior to inclusion, consent regarding their participation in the survey and permission to use their anonymized data for research and publication was obtained. Face to face interviews were conducted with the help of a structured questionnaire.
The survey questionnaire consisted of demographic variables such as sex, age (in years) at the time of survey, last known measurement of weight in kilograms, and height in centimeters. Body mass index (BMI) was computed and categorized as per the criteria defined for Asian population. 9 In the second section of questionnaire information regarding established cardiovascular risk factors was obtained, which include, hypertension (known and currently on antihypertensive medication), diabetes mellitus (known and currently on antihyperglycemic therapy, oral or otherwise), smoking (currently smoking at least 10 cigarettes per day), and family history of premature ischemic heart diseases (in first degree blood relatives; male under 55 years and female under 65 years). Participants last known measurements on total cholesterol (mg/dL) level, high-density lipoproteins (HDL) (mg/dL), random blood glucose (mg/dL), glycated hemoglobin (HbA1c), systolic blood pressure (mmHg), and diastolic blood pressure (mmHg) were also obtained. For the participants with known parameters, 10-year risk of atherosclerotic cardiovascular disease (%) events was calculated using the Pooled Cohort Equations (PCE) and categorized as low (<5.5%), moderate (5.5%-7.5%), and high (≥7.5%) risk group. 10
The third and final section of the questionnaire was regarding participants’ self-awareness and attitude toward risk assessment of cardiovascular diseases. Participants were asked about their last intentional cardiovascular risk assessment and responses were recorder as “assessed within last 1 year, “assessed 1 to 5 years back,” “assessed more than 5 years back,” or “never assessed to this date.” Similarly, participants’ perceived opinion regarding their own categorization of CVD risk was assessed and responses were recorded as “high risk,” “intermediate risk,” “low risk,” or “don’t know/can’t say.”
Collected data were entered into IBM SPSS (version 21) and results were expressed in terms of descriptive statistics such as mean ± standard deviation (SD) and median (interquartile range [IQR]) for scalar variables and frequency and percentages for categorical variables. Participants were categorized into 2 groups based on age and appropriate Chi-square test or Mann–Whitney U test were applied for comparison. P-value ≤.05 was taken as criteria for statistical significance.
Results
A total of 126 cardiac health care providers were interviewed, out of which 20.6% (26) were females and mean age of the participants was 36.1 ± 7.6 years with majority (64.3%) between 31 and 40 years of age. The most prevalent cardiovascular risk factor was family history of CAD (33.3%) followed by smoking (14.3%), and 23.8% of the participant had body mass index of ≥27.5 kg/m2. Demographic characteristics of the participants are presented in Table 1.
Demographic Characteristics and Self-Reported Last Known Measurement of Biochemical Markers.
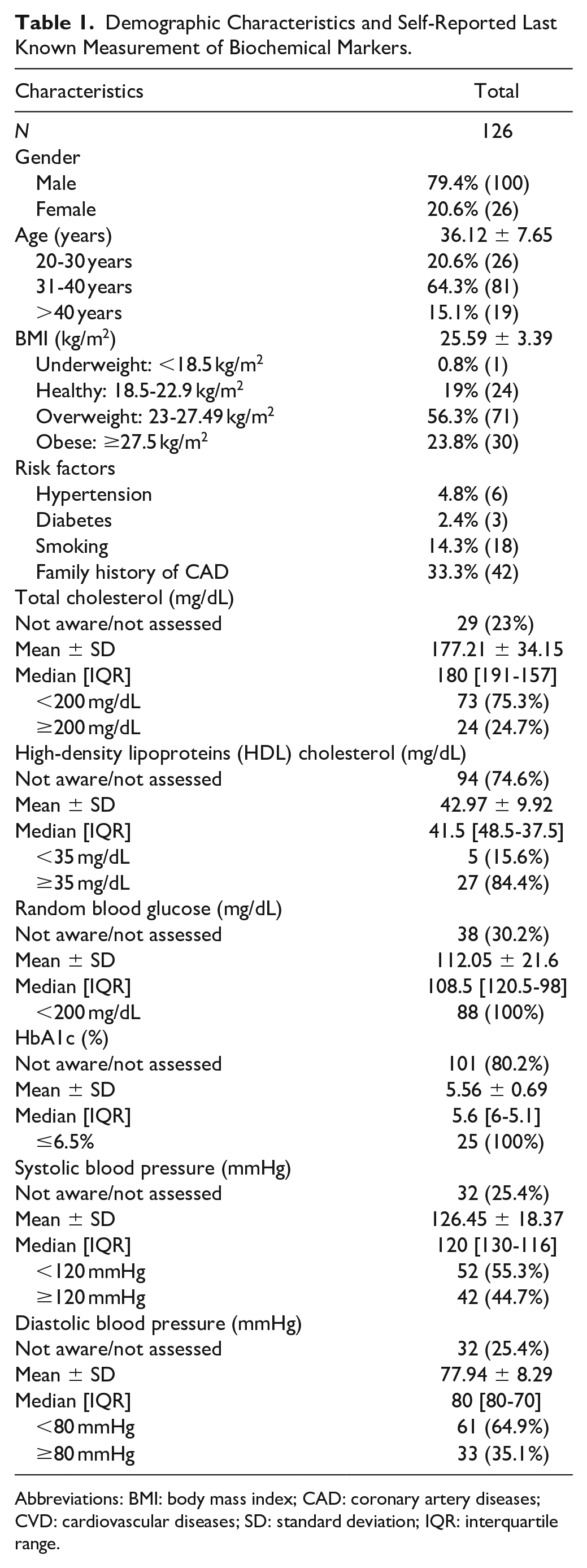
Abbreviations: BMI: body mass index; CAD: coronary artery diseases; CVD: cardiovascular diseases; SD: standard deviation; IQR: interquartile range.
Around 23% of the participants did not know their total cholesterol levels and more than 74% were not aware of their high-density lipoproteins (HDL) cholesterol. According to self-reported last known measurement of biochemical markers, 24.7% (24/97) had total cholesterol ≥200 mg/dL and 15.6% (5/32) had HDL <35 mg/dL. Similarly, around 30% have either never assessed or not aware of their random blood glucose (mg/dL) and more than 80% were not aware of HbA1c (%) level. Self-reported last known measurement of biochemical markers are presented in Table 1.
More than 76% of the participants never assessed their cardiovascular risk and more than 37% don’t know or don’t have opinion about their own CVD risk. Based on Pooled Cohort Risk Assessment Equations (PCE), 10-year risk of atherosclerotic cardiovascular disease (ASCVD) event was estimated only for 25.4% (32) of the participants out of them 78.1% had low risk (<5.5%) and 15.6% and high risk (≥7.5%) of 10-year risk of ASCVD event. There was no association between PCE based ASCVD risk assessment and participants personal opinion of CVD risk level (P-value = .08). Majority (18/25) participants classified in low risk groups also perceived their CVD risk as low risk while 6 (out of 25) low risk participants perceived their CVD risk as intermediate. Risk assessment and attitude toward self-risk assessment are presented in Table 2.
Risk Assessment and Attitude toward Self-Risk Assessment.

Abbreviations: CVD: cardiovascular diseases; SD: standard deviation; IQR: interquartile range.
Risk assessment and attitude toward self-risk assessment by gender and age are presented in Figure 1. Unawareness about CVD risk level and attitude of never to assess the CVD risk was found to be associated with female gender with Chi-square P-value of .01 and <.01 respectively. Unawareness about CVD risk level was found to be associated with younger age (P-value = .03).

Risk assessment and attitude toward self-risk assessment by gender and age.
Discussion
The present study aims to investigate the cardiovascular risk factors among Pakistani cardiac physicians. The results demonstrated the prevalence of multiple cardiovascular risk factors, including family history, elevated total cholesterol levels, smoking, and increased BMI in this low risk population of cardiac physicians. Unlike general population, the conventional risk factors such as diabetes and hypertension were not that common in this population. Positive family history was the most prevailing risk factor followed by BMI ≥ 27.5 (obesity), and smoking. A possible explanation for such ambiguous risk profile is that the majority of participants were educated and under 40 years age.
Positive family history was found to be the most common risk factor in cardiac physicians. It is a non-modifiable risk factor, which cannot be completely eliminated through any medical procedure. Inadvertently, family predisposition seems to make a significant contribution to the burden of CHD in our community. 5 A study was conducted on the general population in Punjab, Pakistan, in which it was noted that 72.9% of males and 79% of females developed the disease because of genetic predisposition. 11 Siblings of patients with CVD have about 40% risk increase, while offspring of parents with premature CVD have a 60% to 75% risk increase. 12 Consequently, family history is an independent risk factor for CVD and it can used as a screening tool to identify individuals who have an elevated risk of CVD, especially asymptomatic young adults. 13
WHO states, decrease in physical activities and high intake of fat are the most common causes of obesity/overweight, 14 leisure-time sedentary behavior is also strongly associated with larger waist circumference (and BMI) and risk of obesity. 15 Long-term Framingham study indicates that being overweight is proportionate to the rate of cardiovascular disease progression. 4 Using the WHO BMI classification for Asians, in hour study 56.3% (71) of the participants were overweight and 23.8% (30) were obese. A BMI of ≥23 kg/m2 was observed in 80.2% of participants, but again, this can be expected to have been overstated because the study group is primarily from a good socioeconomic background considering their occupation.
Our results suggests that, out of 126 cardiac physicians only 18 were smokers. In the 2015 report of WHO, 22.2% of men and 2.1% of women smoke in Pakistan. 1 According to WHO, tobacco use is one of the major risk factors for developing multiple cardiovascular disorders. 16 The link between CVD and smoking is clear; it is a major health problem in the world today, 50% of these deaths would be from the age group between 35 and 69 years. 6 A linear association was shown between cigarette smoking and CVD by INTERHEART and other studies in Pakistan. People who smoke 40 or more cigarettes per day are 9 times more likely to develop cardiovascular problems than those who have never smoked. 2
According to our study, 71.0% and 96.2% of males and females, respectively, have not assessed their cardiovascular risk factors. This suggests decreased self-care among healthcare givers which may lead to high probability of developing CVD. Given the due respect of heart disease in low- and middle-income countries, the prevention of risk factors for cardiovascular diseases in South Asia, especially in Pakistan, is given minimal attention. 8 A majority of our study participants were under the 40 years of age and mostly within the critical cutoff of body mass index (BMI < 27.5), this may be possible explanation for our participants not pursuing the clinical risk assessment of development of CVD. However, this study did find in low risk cardiac physicians, persistent CVD risk factors.
In our results, 4.8% of participants had hypertension. Hypertension alone is a significant risk factor for heart diseases and can multiply the hazard 2 to 3 times. 17 In a study conducted by Iqbal et al. 18 only 40% of the candidates had controlled hypertension due to the fact that compliance toward medication is not emphasized adequately with the essential lifestyle changes. Annually, 13.5% of the total deaths are due to high blood pressure. 2 In recent years, there has been a surge in the reported cases of hypertension in the South Asian region. The definitive etiology for these cases are not known, however, high sodium diet, obesity and inaccessible timely health care are the cardinal causes. 19
About 2.4% of participants had diabetes in our study as against the estimated prevalence of 14.62% in general in Pakistan. 20 Among various other factors such as ageing population, growing prevalence of obesity, hypertension, and family history, 20 self-negligence, improper control of blood glucose levels, poor diagnosis, decrease in physical activity mainly due to urban lifestyle which includes sedentary behavior and poor diet balance are also attributed to the growth is prevalence of diabetes mellitus.14,21,22
Limitations: A small sample size was taken from only one urban tertiary care setup, which doesn’t display the whole picture of what this population is facing and no conclusion could be drawn about the health care providers working in sub-urban/rural areas. The respondents were apparently healthy medical doctors who did not report any symptoms or signs of ill health; however, no blood work was done to prove that they were within all normal healthy parameters. This highlights the need to include more studies from different areas to better assess the vulnerability of the situation and provide guidance for future protective measures.
Conclusion
The present study reveals low prevalence of conventional cardiac risk factors and marginally higher tendency of modifiable risk factors such as smoking and obesity among low risk cardiac physicians. The prevalence of CVD risk factors amongst physicians has alarming implications and a large proportion of physicians have not yet assessed their prevalent risk factors of CVD. If proper health awareness and promotion programs are not held, such ignorance can constitute a major threat to this population. Although health policies are present, thorough awareness for CVD risk factors must be consistently reinforced. Guidelines for CVD detection and prevention need to be developed, disseminated, and enforced.
Footnotes
Authors’ Contributions
SF and KAK conceived the idea, SF and MK designed the study, SF and DK collected data, SF, MK, SA, DK, MTH, MAU, TJS contributed in manuscript writing, MK and KAK reviewed the manuscript, and SF and KAK supervised the entire project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.