
Abstract
Background
Obesity and chronic disease risk are significantly related to healthy lifestyle behavior, including dietary intakes. Further, the interrelated etiology of many chronic conditions supports the comorbidity in US adults to manage multiple diagnoses. The purpose of this study was to assess diet quality across varying numbers of existing conditions, including obesity, hypercholesterolemia, hyperglycemia, and hypertension.
Methods
Cross-sectional analysis of data from 17 356 adults aged 45 years and older from the 2005-2016 National Health and Nutrition Examination Survey were assessed for the presence of overweight or obesity (body mass index >25 kg/m2), hyperglycemia (glycated hemoglobin >5.7%), hypercholesterolemia (>200 mg/dL), and high blood pressure (>120/80 mm Hg). Overall diet quality was assessed using Healthy Eating Index 2015 scores computed from the intakes reported during the 24-hour dietary recall collected in the mobile examination center. The total score (range 0-100) is based on the sum of 13 subscales that represent concordance with the Dietary Guidelines for Americans.
Results
Few adults presented with no markers of chronic disease (n = 407), with other presenting 1 indicator (n = 1978), 2 indicators (n = 4614), 3 indicators (n = 6319), and all 4 indicators (4038). While there was no significant difference in mean energy intakes on the day of intake, those with all 4 markers of chronic disease had a significantly poorer diet quality (P < .001) and consumed significantly more saturated fat (P = .026), but significantly less total carbohydrates, dietary fiber, and added sugars (P < .005). While mean consumption of protein was lowest in those with more chronic conditions, the differences were not significant.
Conclusion
Overall dietary intakes from the day of intake indicated that those with a greater number of chronic conditions presented with poorer overall dietary intakes. The foundational intervention strategy across all evidence-based treatment strategies is the promotion of healthy lifestyle behaviors.
Introduction
The prevention and treatment of chronic disease is what defines modern health care and is the subject of several World Health Organization reports.1-3 The US National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP) estimates that 60% of US adults have 1 chronic disease (including heart disease, cancer, and diabetes), while 40% have 2 or more. 4 Furthermore, chronic diseases significantly contribute to the $3.3 trillion in annual government-run health care costs, and are the leading causes of death and disability in the United States. The Global Burden of Diseases Study of 2010 5 further confirmed the role of poor diet as a risk for lost disability-adjusted life-years, and that high blood pressure, body mass index (BMI), fasting plasma glucose, and total cholesterol are all strongly related to diet. Weight gain over 4 years was associated with a lower diet quality score in the Nurses’ Health Study and the Health Professionals Follow-Up Study. 6 However, Wang et al 7 evolved this finding by associating a healthy dietary pattern to lower weight gain in those predisposed to obesity, suggesting some underlying biochemical advantages of good quality diets. Attaining a good diet quality (adequate intake of fruits, vegetables, whole grains, lean proteins, and unsaturated fats while low in sodium, saturated fat, and added sugars) has been termed primordial prevention of chronic disease, and is part of the American Heart Association’s (AHA) Life’s Simple 7. 8
A lower quality diet is one of the leading preventable causes of death and disability in the United States and globally. 9 Older adults tend to report inadequate intakes of fruit, vegetables, legumes, whole grains, nuts or seeds, fish, lean meat, poultry, and low-fat fluid dairy products, but excess intakes of refined grains, processed and fatty meats, fried foods, solid fats, and added sugars. 10 The diet quality of middle-aged adults seems to be of poorer quality than older adults, possibly setting a foundation for worse aging outcomes. 11 Using the Multiethnic Cohort, 12 diet quality was positively associated with dietary carotenoids and high-density lipoprotein (HDL) cholesterol, and negatively associated with C-reactive protein (CRP), total cholesterol, triglycerides, glucose, and insulin, suggesting some underlying biochemical changes related to diet quality. Similarly, Jacobs et al 13 found that higher diet quality resulted in up to a 20% reduction in risk for type 2 diabetes due to lower homeostatic model assessment of insulin resistance (HOMA-IR), triglycerides, and inflammation (CRP), strengthening the link between diet and diabetes risk. Liese et al 14 observed that high diet quality was associated with significantly lower risk of all-cause mortality, as well as cardiovascular disease and cancer mortality among both men and women. This suggests that diet quality is critically important to the outcomes from many types of chronic diseases, evidenced by reductions in hyperglycemia and hypercholesterolemia.
The link between high dietary sodium and hypertension is well known, as is the Dietary Approaches to Stop Hypertension (DASH) eating plan. 15 While the sodium restriction does improve blood pressure outcomes, the DASH eating plan does not solely focus on dietary intakes of sodium 16 ; instead it focuses on improving overall diet quality, including increasing fruits, vegetables, whole grains, and low-fat dairy while limiting saturated fat and added sugars.
Because the presence of one or more chronic diseases is prevalent among US adults, and poor quality diet is a chronic disease risk factor, 17 it supports the notion that diet quality may be different between those with one and more than one clinical chronic disease risk factor (overweight/obesity, hypercholesterolemia, elevated blood pressure, and poor glycemic control). While broader assessments of diet quality have been linked to chronic disease risk, limited work has explored the differences in diet quality between those with the presence or absence of disease to develop targeted lifestyle interventions. Therefore, the purpose of this study was to assess differences in diet quality and nutrient intakes in adults aged 45 years and older by the number of clinical chronic disease risk factors.
Materials and Methods
Data for 17 356 adults, 45 years and older, from the 2005-2016 National Health and Nutrition Examination Survey (NHANES) with complete dietary intake data were analyzed to assess differences in dietary intakes by the prevalence of clinical chronic disease risk factors across age groups. NHANES is a cross-sectional national surveillance system that monitors the health and nutritional status of the noninstitutionalized US population. Cluster-randomized samples, with purposive oversampling of hard-to-reach populations, was employed for older adults, low-income individuals, and racial/ethnic minorities. Identified potential participants were screened and consented during an in-home interview before scheduling a mobile examination center (MEC) visit to complete dietary, biochemical, and physical assessments. All protocols were approved by the CDC National Center for Health Statistics (NCHS) Research Ethics Review Board.
Presence of Clinical Chronic Disease Risk Factors
The number of clinical risk factors were assessed through the presence of elevated BMI, cholesterol, blood pressure, and glycated hemoglobin across the sample from physical and biochemical measurements from the mobile examination center visit. Presence of overweight or obesity (BMI >25 kg/m2), hypercholesterolemia (>200 mg/dL), high blood pressure (>120/80 mm Hg), and poor glycemic control (HbA1c >5.7%) were determined across each individual participant. The number of chronic disease risk factors exhibited were categorized as none or 1, 2, 3, or 4 (maximum). As few participants had no relevant risk factors, they were combined with those with only 1 risk factor for analytical stability in weighted population analyses.
Assessment of Dietary Intakes and Diet Quality
Dietary intake data from one 24-hour recall per participant were collected in the MEC visit utilizing the validated Automated Multiple Pass Method, which seeks to collect information from foods and beverages reported as consumed from the previous day, from midnight to midnight, by a trained interviewer. 18 Nutrient and MyPlate equivalents were computed from the Food and Nutrient Database for Dietary Studies 19 and the Food Patterns Equivalents Database, 20 respectively.
Overall diet quality was assessed using mean scores for the Healthy Eating Index-2015 (HEI-2015) 21 computed from the intakes reported during the 24-hour dietary recall collected in the MEC. The HEI-2015 is a density-based scale that aligns with the 2015-2020 Dietary Guidelines for Americans (DGA). 22 The scale is composed of 13 subscales that represent food and nutrient intakes for the following intakes: total fruits; whole fruits; total vegetables; greens and beans; whole grains; dairy; total protein foods; seafood and plant proteins; fatty acids; refined grains; sodium; added sugars; and saturated fats. The maximum total HEI-2015 score of 100 represents ideal concordance with the DGA. 23 Intakes of moderation are reversed scored; therefore, a higher score on all subscales as well as the overall index are indicative of better diet quality.
Statistical Analysis
Public use data files were downloaded for data preparation and analysis. Statistical Package for the Social Sciences (SPSS) Complex Samples (version 25.0, IBM SPSS) was used to conduct an analysis by the number of clinical chronic disease risk factors. The data were weighted with SPSS Complex Samples to produce nationally representative estimates of dietary intakes and conduct statistical testing with appropriate standard errors to control type 1 error. Descriptive statistics were utilized to assess personal and demographic characteristics as well as dietary intakes compared to recommended levels. Analysis of covariance was used to compare means of nutrient intakes, MyPlate equivalents, and HEI-2015 scores, adjusting for race, ethnicity, gender, marital status, and percent of the federal poverty rate. Statistical significance was established a priori at .05.
Results
Demographics
Of the 17 356 adults, few presented with no clinical risk factors of chronic disease (n = 407; 3.0%), whereas other participants presented with 1 factor (n = 1978; 13.0%), 2 factors (n = 4614; 28.1%), 3 factors (n = 6319; 36.3%), and all 4 risk factors (n = 4038; 19.6%) of chronic disease. For the remaining analyses, those with none or 1 clinical factor were combined. Demographics and personal characteristics by number of clinical chronic disease risk factors are presented in Table 1. The prevalence rates of number of clinical chronic disease risk factors were similar by sex and marital status. Non-Hispanic Whites (17.7%) and those with at least a college degree (14.4%) had the lowest proportion presenting with all 4 risk factors of chronic disease, with the highest rates found in African American (28.3%) and those with less than a ninth-grade education (27.2%).
Demographics by Number of Clinical Chronic Disease Risk Factors. a

Abbreviations: HS, high school; GED, General Education Diploma; AA, Associate’s degree.
Data presented as unweighted count (weighted %).
Prevalence of Clinical Chronic Disease Risk Factors: Comorbid Diseases
Table 2 presents the proportional distribution of comorbid diseases by the presence of each clinical risk factor of chronic disease. Less than 10% of adults presenting with a chronic disease risk factor possessed only that condition, with the majority presenting with multiple diseases. Between 23% and 33% of adults with each of the investigated factors had one additional clinical risk factor of chronic disease. Nearly three-quarters of adults presenting with an elevated glycated hemoglobin presented with the other 3 clinical factors of chronic disease.
Prevalence of Clinical Chronic Disease Risk Factors Across Adults. a

Abbreviations: Dx, diagnosis; BMI, body mass index.
Data presented as unweighted count (weighted population %).
Food Group and Nutrient Intakes
Nutrient intakes differed across adults with varying number of clinical chronic disease risk factors (Table 3). Participants with three or all four risk factors consumed significantly higher proportions of their total calories from fat, and specifically from saturated fat, than those with fewer risk factors. Total energy intakes were not significantly different across groups. Adults with all 4 chronic disease factors consumed significantly less carbohydrates and fiber, and significantly more total fat and saturated fat than those with fewer chronic disease factors. Adults with more clinical risk factors consumed significantly more sodium and less potassium than adults with fewer clinical factors.
Differences in Nutrient Intakes Across Adults With Varying Number of Clinical Chronic Disease Risk Factors.*

Mean (SE) intakes from analysis of covariance, adjusted for age, race, ethnicity, gender, marital status, and percent of federal poverty rate.
Values with different superscripts are significantly different.
Table 4 shows the differences in food group consumption from the day of intake across adults with varying number of clinical chronic disease risk factors. Adults with all 4 factors consumed significantly more total and refined grains than all others with fewer chronic diseases (P = .026), while those with none or 1 clinical risk factor for chronic disease consumed significantly more whole grains (P = .002). Intakes of total fruit differed significantly across all groups, with those with fewer risk factors having higher intakes of fruit (P < .001). Adults with 3 and 4 chronic disease risk factors consumed significantly more total meat and processed meats than all other adults, but intakes were not different from each other (P < .001, respectively).
Differences in Mean MyPlate Equivalents Intakes by Number of Clinical Chronic Disease Risk Factors.*
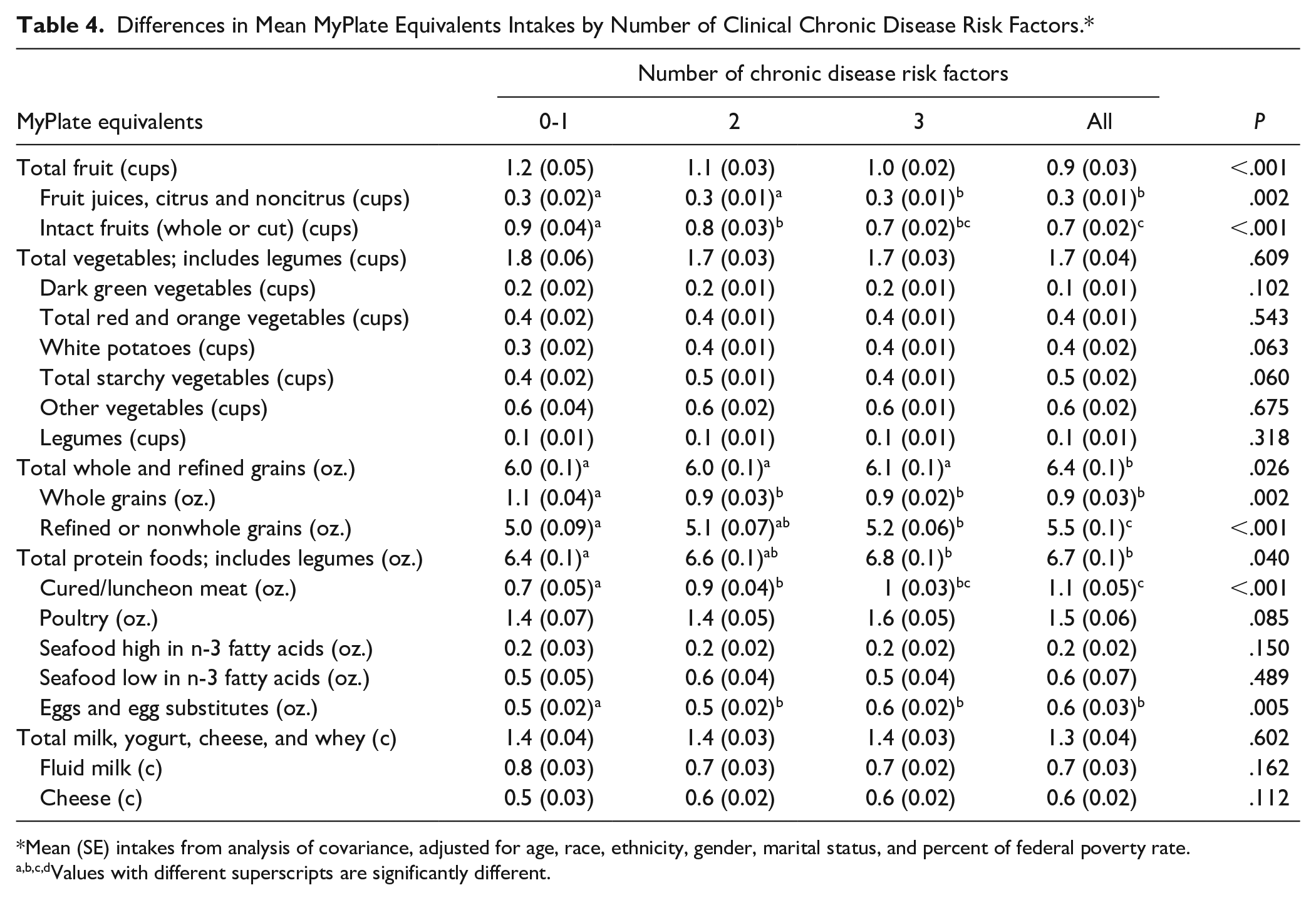
Mean (SE) intakes from analysis of covariance, adjusted for age, race, ethnicity, gender, marital status, and percent of federal poverty rate.
Values with different superscripts are significantly different.
Diet Quality
Overall diet quality was progressively lower across groups. Adults with none or 1 clinical risk factor of chronic disease had significantly better total diet quality compared to adults in all other groups (Table 5; P < .001). Their diet quality was also significantly better for total fruit, whole fruit, greens and beans, whole grains, seafood and plant and plants proteins, and saturated fat compared to all adults with more than 1 clinical risk factor (P ≤ .002). Adults with all 4 chronic disease risk factors had the lowest diet quality across all groups, with total fruit, refined grains, and sodium significantly lower than all other groups (P < .001).
Differences in Mean Healthy Eating Index-2015 (HEI-2015) Scores by Number of Clinical Chronic Disease Risk Factors.*

Mean (SE) intakes from analysis of covariance, adjusted for age, race, ethnicity, gender, marital status, and percent of federal poverty rate.
Higher scores for scales related to moderation represent lower intakes.
Values with different superscripts are significantly different.
Discussion
Improving health, functionality, and quality of life of older adults is a goal of Healthy People 2020. 24 Sixty percent of older adults manage 2 or more chronic diseases and there are marked disparities in their dietary intakes. Diet quality of US adults is generally improving over time, but not fast enough to meet the Healthy People 2020 objectives. 25 Diet quality has been linked to morbidity and mortality from chronic disease. 26 Poor diet over many years has been shown to contribute to the development of chronic diseases, such as overweight or obesity, hyperglycemia, hypercholesterolemia, and hypertension. As lifestyle behavior interventions are the primary treatment approach from evidence-based practice guidelines, diet quality is an important consideration for chronic disease management, especially in those with multiple comorbidities. The present study indicated that US adults have poor diet quality, especially among those with a higher number of clinical risk factors, which may be used for targeted care for the lifestyle management of chronic conditions.
Although individual health status has multiple contributing factors, diet and nutrient intakes are major determinants of healthy aging and quality of life. While dietary recommendations differ slightly across disease states, they carry many of the same tenets linked to overall diet quality. Reedy et al 26 observed that higher diet quality indices were associated with 12% to 28% decreased risk of all-cause, cardiovascular disease (CVD), and cancer mortality during 15-year follow-up in the NIH-AARP Diet and Health Study. Higher intakes of whole grains, vegetables, fruit, and plant-based protein were key elements associated with higher diet quality. Poor dietary patterns and intakes among adults with chronic disease were related to poorer disease and health outcomes. Similarly, the Health ABC study found that in older adults (70-79 years), a diet consistent with current guidelines, including relatively higher amounts of vegetables, fruits, whole grains, poultry, fish, and low-fat dairy products, may be associated with superior nutritional status, quality of life, and survival. 27 In the present study, adults with higher number of clinical chronic disease risk factors had poor intakes of fruits and whole grains, while consuming more refined grains, starchy vegetables, meats, and eggs, which was related to a greater number of chronic conditions.
Micha et al 9 identified 10 foods and 7 nutrients with evidence for causal cardiometabolic effects, including protective effects of fruits, vegetables, beans/legumes, nuts/seeds, whole grains, fish, yogurt, fiber, seafood with omega-3 fatty acids, polyunsaturated fats, and potassium; and harmful effects of unprocessed red meats, processed meats, sugar-sweetened beverages, high glycemic load, trans-fats, and sodium. Likewise, in the present study of US middle-aged and older adults, those with fewer chronic conditions reported higher intakes of whole grains and fruits, and lower intakes of refined grains, total meat, and processed meat, demonstrating a level of congruency between broader associations in individual behaviors. One noteworthy finding was the better added sugars score among those with a great number of chronic conditions, despite poorer intakes on many other scales. With such a greater emphasis on added sugar intakes, especially in the management of diabetes, 28 these data could offer positive outcomes of the system’s focus on this single element in changing patient behavior. However, it also uncovers the other areas for improvement.
Analyses by Micha et al 9 and Reedy et al 26 also support an approach with an emphasis on foods rather than nutrient-based metrics for determining risk of chronic disease. The data from the present study are aligned with such efforts as key priorities for reducing burdens of cardiometabolic diseases; however, it also illuminates areas where improvements in diet quality can be made. Establishing foci for medical nutrition therapy is an important step to shape patient-focused, evidence-based care. In the Health Professionals Follow-up Study and Nurses’ Health Study, compared with individuals whose diet quality remained relatively stable in each 4-year period, those with the greatest improvement in diet quality scores had a 7% to 8% lower CVD risk in the subsequent 4-year period. 29 Additionally, increasing diet scores were associated with lower CVD risk during the next 20 years, while a decrease in diet quality scores was associated with significantly elevated risk of CVD.
It is known that diet and lifestyle changes can positively affect overweight or obesity, hypercholesterolemia, high blood pressure, and poor glycemic control. 30 Wilson et al 25 reported that the mean HEI-2010 total score for the US population had increased from 49 in 1999-2000 to 59 in 2011-2012, and projected that if it stays on this trajectory it could reach a score of 65 by 2019-2020. However, the current study shows that HEI scores of US adults are not advancing as anticipated, further highlighting the need for more targeted nutrition education programs and campaigns. A diet that would meet the Healthy People 2020 objectives would need to receive a score of 74, which might not be achievable given the findings of the present study and will require dramatic shifts from current trends.
Results of the current study and previous studies demonstrate the need for substantial changes in individual dietary intake behaviors to change the American diet quality and chronic disease risk trajectory, especially among adults with a greater number of chronic conditions. Further, aging adults often have multiple medical conditions affecting their dietary intakes and may be using numerous prescription and over-the-counter medications that can impair food intake or alter digestion, absorption, metabolism, and excretion of nutrients. It is essential to remove the barriers to healthy eating to help lower the risk of chronic diseases. 31 The present study further demonstrates that identifying targeted ways to improve diet quality and nutrient intake of adults is key to lowering risk of chronic disease and to improving health among US adults.
The present study has several strengths and limitations that need to be considered. This study utilizes cross-sectional data from a large national nutrition monitoring surveillance program, producing a nationally representative estimate of US adults’ dietary intakes. Differences in nutrient intakes and diet quality by clinical chronic disease risk factors were assessed, which identifies opportunities for nutrition intervention targets. While national surveillance data are useful to assess broader dietary patterns, study limitations also need to be acknowledged. This cross-sectional population analysis is based on a single 24-hour dietary recall per participant; although the Automated Multiple Pass Method helps maximize recall and accuracy of the data collected, it is still reliant on self-reported dietary intake. The reported nutrient intakes are associated with the known limitations of dietary recalls, including underreporting across different demographic characteristics and food groups. Further, these data cannot be assumed to represent usual intakes. As a cross-sectional study, a causal inference cannot be made for the dietary intakes and presence or absence of chronic disease, but to identify overall patterns on the day of intakes reported. As well, this analysis was limited to dietary intakes and did not account for other lifestyle behaviors. Future studies should examine the longitudinal changes in nutrient intakes, diet quality, and relationships to clinical chronic disease risk factors and health outcomes.
Conclusion
Overall diet quality in this study was lacking in middle-aged and older adults in the United States. While poor diet quality itself could be a risk factor for chronic disease, the diet quality of US adults with more clinical chronic disease risk factors is worse than those with less risk factors. This provides formative data to support targeted lifestyle management of chronic conditions, especially among those with multiple comorbidities. Helping individuals make the right food choices will help improve nutrient intakes and diet quality while lowering their risk and required management of chronic diseases, ultimately supporting healthy aging. Early intervention for promoting healthy lifestyle behaviors, such as improving diet quality, especially in middle-aged adults, could improve health outcomes later in life by managing the clinical risk factors for chronic disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Satya S. Jonnalagadda and Owen J. Kelly are employees of Abbott Nutrition.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by a grant from Abbott Nutrition.