
Abstract
Increased migration has given rise to more advocacy efforts against female genital mutilation or cutting (FGM/C), legislation that criminalizes the practice, and guidance to the health sector for managing care of affected groups. More women and girls who have been cut or who are at risk of FGM/C are migrating from regions where it is common to countries where it is not and interacting with health professionals and other community practitioners in these host countries. Despite numerous studies on the negative health impacts of FGM/C, little is known about toolkits on FGM/C that providers can use in their prevention and response efforts. We sought to explore the nature of Internet-based products referenced as toolkits and materials characteristic of toolkits aimed at different service providers who may interact with women and girls affected by FGM/C. Through an online search, we identified 45 toolkits and collected data about each one. We found that the toolkits targeted different audiences and offered a diverse set of information and resources. The majority of toolkits were aimed at health professionals and provided factual and epidemiological-focused content, yet many did not include research evidence, skills development application, or approaches for implementing the toolkit in practice. This review is the first completed in the area of FGM/C to show a rich diversity of online materials. Future toolkits can be improved with the provision of evidence-based information and practical skills development for use by health professionals in implementing best practices in working with women and girls affected by FGM/C.
Background
Over the past two decades, the global community has worked to bring an end to female genital mutilation or cutting (FGM/C). 1 Despite prior programs focused on eradication and accommodating care for affected women and girls 2 and the United Nations’ first resolution in 2012 calling for member states to eliminate FGM/C within their borders, 3 the practice forestalled progress on the 2015 Millennium Development Goals.4,5 The current 2030 Sustainable Development Goals call for specific elimination of FGM/C as part of a larger objective to strengthen gender equality. 6
Over 200 million women worldwide have experienced FGM/C, 7 and over 3.5 million girls are at risk annually. 8 A global health concern, FGM/C also is long-standing human rights issue as girls are cut in childhood or adolescence. 8 The World Health Organization (WHO) categorizes FGM/C into four types. 9 While FGM/C does not confer any health benefit, we acknowledge that it is performed in accord with long-standing, multidimensional cultural values. 10 However, multiple adverse health risks can span the life course, including physical impacts involving difficulty in urinating, difficulty during sexual intercourse, chronic infections, and pregnancy and delivery complications. 11 Psychosocial impacts include anxiety, depression, and posttraumatic stress disorder.12,13
The Impact of Migration and Need for FGM/C Care Services
While geographic prevalence is spread across approximately 30 countries in Africa, the Middle East, and Asia, 14 global migration patterns and immigration rates have given rise to FGM/C in developed countries. 15 In 2016, the United States government estimated that more than 513 000 women and girls had undergone or were at risk of FGM/C “wholly a result of rapid growth in the number of immigrants from FGM/C-practicing countries.” 16 However, the precise prevalence of FGM/C in the United States is unknown, as is the case in other host countries. 17
Increased migration since the late 1980s 18 has prompted passage of national legislation to criminalize FGM/C and mandate reporting of known cases in the Americas, Europe, and the Oceania region.19-21 Furthermore, migration has heightened FGM/C awareness and created a need to inform health care systems on its harmful effects.22,23
While efforts over the past two decades have focused on ending FGM/C through advocacy, education, and awareness building,1,24 attention in recent years has turned to managing care for affected women.25,26 Such management includes educating health care providers on FGM/C cultural factors, using screening guidelines, and encouraging skills to improve communication about this sensitive topic. Recognizing the challenges involved in providing care in this realm, the WHO in 2016 issued its most recent set of FGM/C guidelines for health professionals and policymakers. 27 Furthermore, research recommends a holistic, multidisciplinary approach to care delivery with attention to the social, cultural and psychological contexts of health and the harmful consequences of FGM/C. 28
Use of Toolkits to Improve Public Health and Clinical Care
Information directed to public health and health professionals continues to expand, including in particular toolkits to transfer knowledge to improve practice.29,30 However, the term “toolkit” has not been assigned a consistent format, definition or interpretation. 31 As a result, Barac and her colleagues explain that the term can include any “combination of educational materials including templates, instruction sheets, literature reviews, videos, and posters, presented in a variety of formats (hard copy, web).” 29 Davis et al 31 cite the definition of toolkit given by the US Agency for Healthcare Research and Quality: “[A]n action-oriented compilation of related information, resources, or tools that together can guide users to develop a plan or organize efforts to conform to evidence-based recommendations or meet evidence-based specific practice standards.”
Web-based resources expressly labeled as toolkits or having the characteristics of toolkits have grown to promote health on diverse issues such as miscarriage, nutrition, tobacco cessation, and disease prevention.32-35 Toolkits also exist to help meet the needs of different groups, such as autistic adults, 36 address obesity prevention, 37 and help physicians improve practice and accountability.38,39
Barac et al 29 found that while toolkits are perceived as practical and useful, “they lack scientific rigor with respect to the evidence underlying their content, and evaluation of their overall effectiveness.” Other research suggests that despite little information available on the implementation or impact of toolkits, the health sector continues to procure them because they seemingly provide an efficient means of instituting enhanced practices. 30 Despite limited research on toolkit uptake and effectiveness, 40 studies also indicate that practical use of toolkits suffers from context-specific challenges and limited resources.30,31
Toolkits to Assist Practitioners and Support Women and Girls Affected by FGM/C
Despite the established negative health risks associated with FGM/C, there is limited understanding of the needs of affected women and girls,41,42 as well as a paucity of research on providers’ knowledge and attitudes toward FGM/C. 43 Many health care providers in the United States, for example, have limited knowledge about FGM/C and capacity for managing medical complications. 26 Research suggests this is also the case for practitioners globally.23,43,44
Few evidence-based resources and interventions exist to educate and improve providers’ skills to deliver optimal care in cases of FGM/C.24,27,45,46 For instance, the American College of Obstetricians and Gynecologists does not list a practice advisory on FGM/C on its website, 47 and while it offers e-module tools for practitioners on issues such as breastfeeding 48 and obesity, 49 one on FGM/C is lacking. However, to inform professionals and to protect children, the health, social services, law enforcement, child protection, and education sectors have developed guidance on FGM/C. Examples of such material include summaries of U.S. state laws on FGM/C,26,50 brochures and factsheets,11,51,52 and tables and illustrations detailing the types of FGM/C and related chronic and acute consequences. 53
There also are an insufficient number of support and educational resources for women with FGM/C, and limited inquiry on psychological effects of the practice.24,54 Researchers recommend shared decision making and an integrated approach to providing optimal care,23,55 including the provision of high-quality and connected care in areas of mental and sexual health.26,56,57
Statutory measures to combat FGM/C, increased media and political attention, expanded use of the Internet for health information, and advocacy for digital innovations in care delivery 58 make FGM/C an area in which online knowledge sharing has emerged, including in particular toolkits that offer, for example, screening assessment tools, educational materials, and trainings. The capacity of health systems to adequately manage FGM/C sequelae is challenging in both countries where the practice is customary and in host countries,55,59 and toolkits can impart important information to help improve patient care.
To the best of our knowledge, there are no studies that have reviewed web-based toolkits as knowledge sharing resources on FGM/C. Given the global attention to FGM/C and use of the Internet to mediate medical practice and education,60,61 this review is important to understanding the scope of resources available to a diverse set of stakeholders, and to inform areas for future research and intervention development.
Purpose
To address this need, we sought to identify and review existing internet-accessible toolkits aimed at presenting information about FGM/C to educate and improve FGM/C-related health services, including mental health care, and provide resources directly to affected women. This review was a key component of our project to construct a toolkit for women in the United States who have experienced FGM/C and their health care providers. In addition to facilitating project objectives, it was our belief that the review would illuminate the availability of online information and identify strengths and gaps in identified toolkits.
Methods
To capture a broad set of websites that present information on FGM/C and locate toolkits that were published in previous years as well as more recent ones, we conducted a Google search with no limit on date published. We used Google as the sole search engine because it is optimized to locate websites with the use of search terms. 62 Existing literature suggests that Google is the most popular search engine globally, dominating the market in electronic discovery of information through organic, keyword searching. 63 Google was also chosen because the objective was to locate websites containing information on FGM/C. Use of an academic search engine, such as Google Scholar, would have produced results of scholarly information but would not necessarily have produced a variety of FGM/C-related websites.
The search was limited to resources and toolkits delivered or available in English. A combination of the following search terms and phrases was inputted into Google: “toolkit,” “FGM,” “FGC,” “FGM/C,” “female genital mutilation,” “female genital cutting,” “online resources,” “toolkits FGM survivors,” and “health care professionals.”
Considering the lack of a uniform definition of toolkit and that toolkits can be varied materials as well as structured sets of information and resources, our search included products expressly labeled as toolkits, as well as sites that provided content similar to that in labeled toolkits, such as an orientation on FGM/C, available protections, clinical care management and other practice-focused material, and third-party resources for information.
Our online search generated a total of 45 toolkits. We reviewed our sample by drawing on existing research on health-related toolkits from which we learned that to promote practice change, toolkits should be backed by demonstrated effectiveness and the content should include evidence.29,30 We also drew on our objective to develop and evaluate an educational toolkit for health professionals and women affected by FGM/C. We structured our review to locate information in the following six domains: country of origin, date of issuance, derivation of publisher, format, target audience(s), and focus and content description, including research evidence underlying the content. If available, we considered clear statements as to the toolkit’s country of origin, date of origin, and derivation of publisher as demonstrative evidence of such information. We determined the format based on the uniform resource locator (URL) that represented a website (eg, ending in .com) or file (eg, PDF or HTML).
We determined the target audience(s) based on direct statements regarding the publisher’s intended or potential users. We interpreted each toolkit’s primary focus based on direct statements expressing the principal purpose or aim. Similarly, we determined the content, including dominant themes, based on provision of textual and multimedia materials, such as images and audiovisual files, that conveyed the key topics and elements. Where possible, we identified and described evidence provided by the publisher on sources of information for the presented content.
Results
This section summarizes key findings pertaining to our review of the identified web-based toolkits on FGM/C. Table 1 presents the results of our review, with applicable hyperlinks, issuer information, date of publication if ascertainable, and dates that the websites were accessed.
Online Toolkit Sources. a

The URLs listed in the table were operable at the time of research and data collection. All may not be currently accessible.
In our sample of 45 toolkits, we found 31 geared toward health professionals, with some overlapping with other stakeholders working in social services, law, law enforcement, child protection, education, and national level policymaking.
Format of Toolkits
The identified toolkits (N = 45) were of varying format, including websites with different design layouts, online PDF or HTML publications (eg, reports and brochures), information about e-learning modules, reference to DVDs or CD-ROMs for the toolkit content, and journal articles (see Table 2). The near majority (n = 22, 49%) were digital publications of PDF or HTML files. Twelve were presented as websites with varying layouts, featuring horizontal navigation menus or vertical scrolling designs. Three toolkits were in the format of self-paced e-learning (internet-based) modules, and one was in the format of CD-ROMs for purchase.
Female Genital Mutilation/Cutting (FGM/C)–Related Toolkit Format and Target Audience.
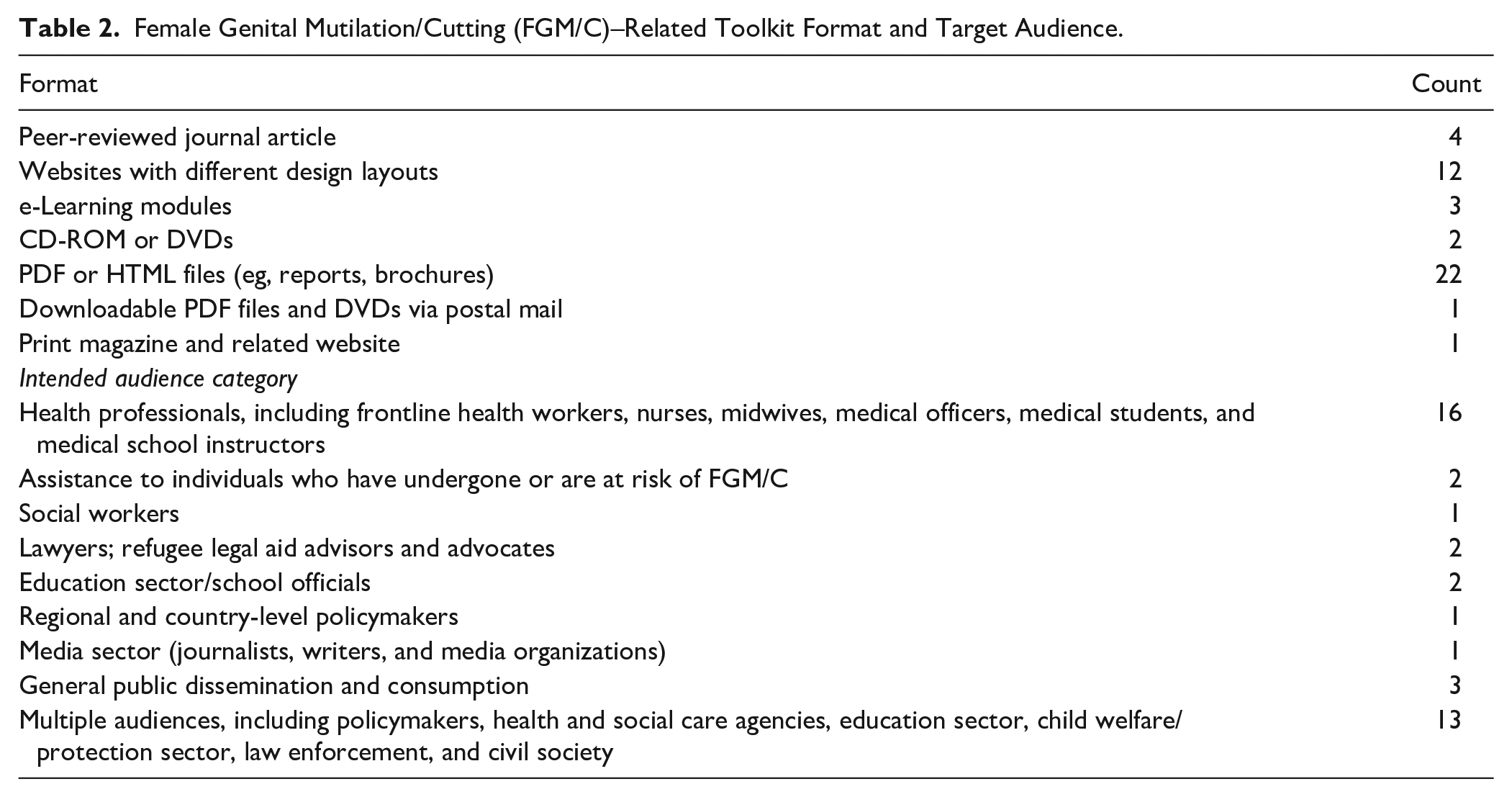
In addition, one website toolkit offered two versions of a resource DVD free of charge, one for health professionals and one for nonhealth professionals. Directed mainly to health and child protection sectors, another toolkit offered guidance free of charge as downloadable PDF files or as DVDs via postal mail. Four toolkits were in the format of articles published in peer-reviewed journals based in the United States and Canada. One resource was an article published online in association with a print magazine.
Target Audiences
Audiences varied from health care staff and social workers to law enforcement, lawyers, teachers, child protection services, policymakers, the general public, and civil society. Some toolkits aimed to serve multiple audiences (see Table 2). For over a third of the toolkits (16, 36%), the target audience was exclusively health professionals, such as general practitioners, clinical specialists, nurses, midwives, medical students, instructors, and health staff working in international development field missions around the world. Of these, two immigrant health toolkits issued in the United States and Canada, respectively, aimed to provide information about FGM/C specifically to pediatricians. Three toolkits in the form of journal articles were directed to primary care doctors, family physicians, or obstetrical-gynecological specialists.
Thirteen of the toolkits aimed to inform a diverse set of stakeholders involved in medical care delivery and safeguarding children at risk of FGM/C, such as policymakers, health and social services, education, child welfare/protection, law enforcement, and civil society. Two toolkits in our sample were aimed specifically at teachers and school officials, and another two were intended exclusively for lawyers and legal aid advisors/advocates who assist immigrant populations. None of the toolkits exclusively targeted professionals working in child protection and welfare; this group was included with broad audiences that included health, law, social care, and education sectors.
One toolkit was exclusively designed to support social workers, along with a single toolkit intended for media professionals. In addition, one toolkit was specifically aimed at informing and supporting policymakers in member states of the European Union. In our sample, only two resources issued by nonprofit organizations specifically offered aid to women who have undergone FGM/C, one specializing in legal and social services for immigrant women and girls in danger of violence, and another offering medical, psychological, and legal assistance to support affected women and girls.
Issuing Entities and Countries
The majority of the toolkits were produced in the United States (see Table 3). In addition, 14 toolkits originated in the United Kingdom. The European Union also was in our sample. The other issuing countries were all Western countries, specifically, Australia, Belgium, Canada, New Zealand, and the Netherlands, with the exception of Kenya.
Originating Countries and Types of Issuing Entities.
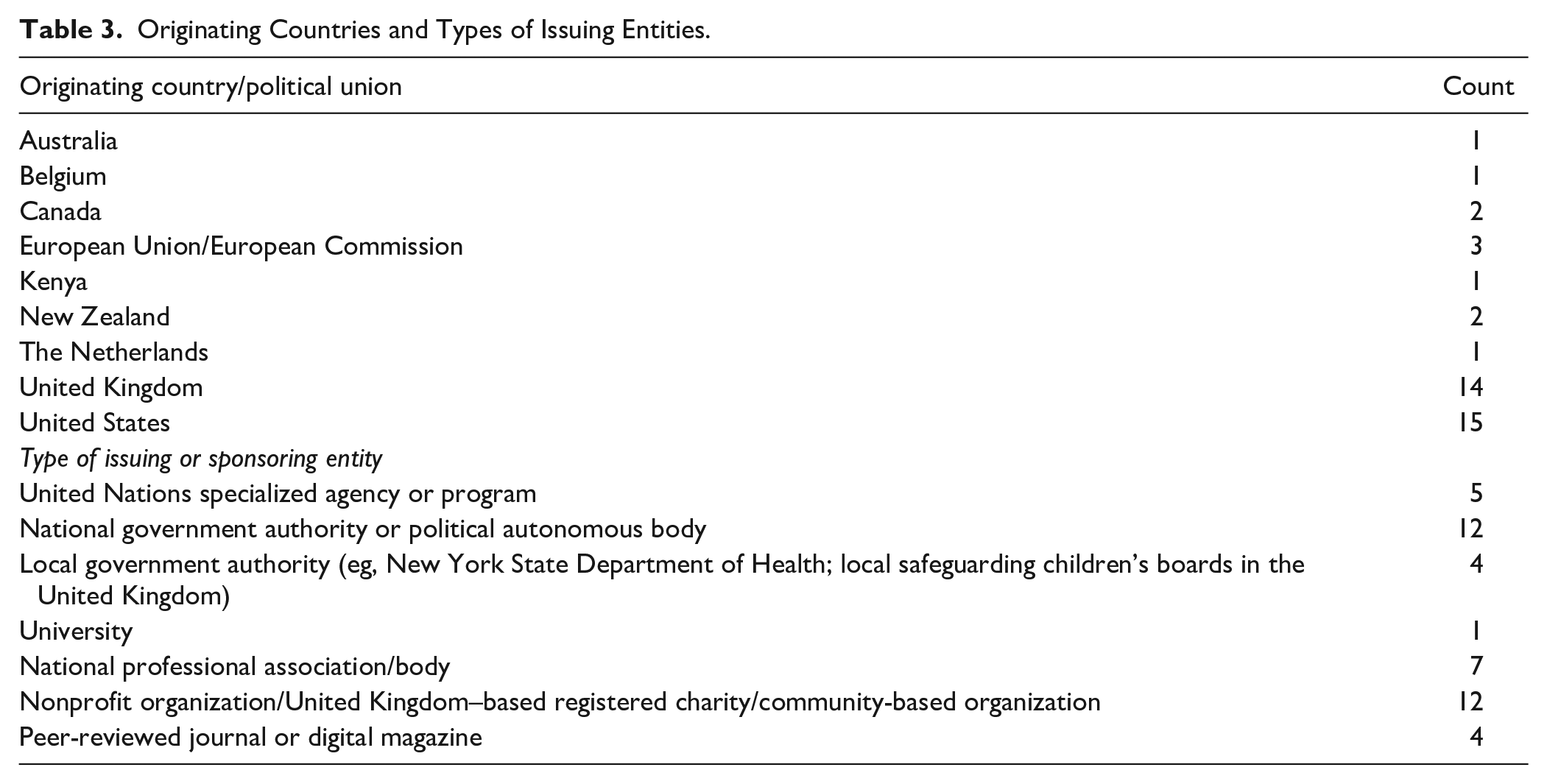
The toolkits were published by a variety of entities, including United Nations organizations, national government institutions, local government authorities, professional associations, nonprofit organizations, including United Kingdom–based registered charities, community-based organizations, and academic publications.
Toolkit Focus and Content
We found that the focus of the toolkits varied, ranging from advocacy/policy efforts for FGM/C prevention and elimination, child protection, and education in school settings, to law enforcement, immigration/asylum assistance, clinical practice, and reporting in accord with applicable law (see Table 4).
Toolkit Focus and Content Overview.

Overall, we found the toolkits to be variable in quality of content and timeliness of information presented. They communicated epidemiological and legal information, but lacked the provision of skills development or a presentation of evidence-based practices in working with women who have experienced FGM/C or girls at risk of FGM/C. None of the toolkits included results of an evaluation of their effectiveness as a strategy, in connection with implementation or clinical outcomes, or recommended that users test the toolkit in a work setting. However, a few included literature reviews, an evidence-based approach to discussing FGM/C in clinical settings, and recommendations and best practice statements.
Among the 31 toolkits directed at health professionals, the content for 15 included some combination of tables, illustrations, factsheets, checklists, lists of frequently asked questions, leaflets for patients, and hyperlinks to information and resources germane to FGM/C, as part of the presentation of materials. Dominant themes in these toolkits included information on the origins of FGM/C, prevalence data, types of FGM/C, relevant laws, medical treatment recommendations, and in some cases, communication guidelines based on the authors’ personal clinical experiences to help providers discuss FGM/C with their patients (see Table 4). In seven of the 31 toolkits, we found some mention of the need for cultural awareness on the part of the practitioner, in interacting with and providing care to women and youth with FGM/C. Some of toolkits also presented language to use when discussing FGM/C with patients, screening questions, and associated acute and chronic health consequences. Eleven of the 31 toolkits included references to existing literature.
In five toolkits on clinical management of FGM/C, it was unclear from the website if the information provided was based on research evidence, because citation references were missing, or because we were unable to ascertain if evidence was included because the site required a login to gain access to the materials themselves. Of the 45 toolkits, one offered self-assessment quizzes and electronic certificates for completion of e-learning courses on FGM/C.
Five of the six toolkits issued by global organizations, including the WHO, United States Agency for International Development, United Nations Population Fund, and United Nations Development Programme, were designed to inform medical instructors, medical students, midwives, mission-based staff, and individuals who direct the work of medical staff in global settings. These five toolkits aimed to impart knowledge about the different types of FGM/C, affected populations, global prevalence of the practice, and its immediate and long-term health consequences. The sixth toolkit aimed to educate the general public and build awareness, and highlighted incremental change occurring in Egypt in part because of the organization’s efforts to combat FGM/C there.
Two of the three toolkits issued by the WHO were issued in 2001 and one in 2016. The 2001 publications focused on management of medical complications from FGM/C, one of which provided a set of training manuals for medical teachers and students on strategies to prevent FGM/C and manage health impacts. The 2016 WHO guidelines also focused on FGM/C complications and cited “evidence-informed” best practices and recommendations with inclusion of a reference list and a description of the process for developing the document.
Eight of the toolkits focused on disseminating information in connection with advocacy efforts to eliminate FGM/C, and in two cases, highlighted firsthand accounts from women of the impacts. With prevention and abandonment of FGM/C as the focus, the content of these toolkits discussed available protections for women and girls, strategies for engaging schools and communities, and leveraging law and policy to facilitate change. One U.S.-based nonprofit organization published videos of refugee women who had undergone FGM/C and their experiences of asylum and integration in foreign countries. However, only one toolkit specifically aimed to provide individual support to affected women, including psychosocial support, in addition to offering community-based workshops and training to professionals working in education, health care, law, and social care.
The majority of toolkits originating from the United Kingdom addressed health and nonhealth professionals involved in child welfare and safety, because of the 2015 UK law mandating reporting of cases of FGM/C in girls under age 18. 64 Government authorities issued a collection of online information products covering mandatory reporting in health, social care and education realms, services and resources for affected women and girls, and video and e-learning resources for health professionals. In addition, multiagency local safeguarding children’s boards, responsible for coordinating child protection and welfare work at the community level, and registered charities in the United Kingdom issued toolkits on protecting children and web-accessible learning modules on FGM/C.
Discussion
Generally, reviewing web-based tools can be challenging because of the variety of information presented and issues beyond quality of content, such as design and perceived user-friendly characteristics of a website. In the domain of health specifically, a definitive tool for assessing the quality of web-based information does not exist. 65 Our review brings forward the perceived role of online toolkits in educating and informing practitioners in different health-related settings who work with ethnically diverse groups affected by FGM/C. Despite the variety of materials that our review reveals, our findings suggest that toolkits can be improved in three domains set out below. However, it is also important to consider that the toolkits were developed by a variety of entities to address different needs of women and girls at different times, so our inferences and findings are presented with caution.
More Inclusion of Research Evidence and Skills Development
While some of the toolkits addressed FGM/C prevention efforts, the majority (n = 31) aimed to inform health care practice for affected women and girls. Ten of these, however, did not cite sources as evidence for the presentation of content, or it was not clear if the information was based on existing research. In cases where evidence was given in connection with, for example, suggested guidelines and screening questions, and descriptions of risk factors associated with FGM/C, the form of evidence was reference lists of literature. Ultimately, the primary purpose of most of the toolkits was to impart information and potentially guide interventions to protect young girls and improve health outcomes for women with FGM/C. Virtual toolkits supported by evidence can help issuing entities better serve providers in implementing best practices in this important area of women’s physical and mental health.
None of the toolkits in our sample included a clear statement regarding envisioned goals of providing the information as a strategy to improve health services for women with FGM/C. Only one, aimed at European Union policymakers, referenced the use of behavioral change theory and community-based participatory action to end FGM/C, and described an intervention delivery and evaluation strategy for stakeholders to assess whether the approach results in change in the community over a period of time. 66 Along with specifying a target audience, which research suggests can help to make toolkits more effective, 31 inclusion of evidence in an FGM/C toolkit to substantiate conceptual components can positively affect perceived reliability. Such inclusion also may facilitate provider buy-in and engagement and assist in the development of a validated FGM/C screening tool, which currently does not exist. 26
Overall, the toolkits offered information on the epidemiology of FGM/C. This is similar to existing research on training and research reference materials on FGM/C management that “showed major strength in epidemiology, but scored marginally on physical, gynecological, and obstetric complications.” 67 While the resources we identified generally aimed to fill knowledge gaps about FGM/C, our findings suggest a need for more materials backed by evidence that can be implemented as interventions oriented toward improved health services.
Additionally, there is a need for skills development and easily accessible tools that can be used by providers, including psychologists, to ensure optimal professional practices are implemented when working with populations affected by FGM/C. One area of skills development, for example, should be the provision of culturally sensitive care that all toolkits in on FGM/C should reference as critically important. Effective communication is fundamental to implementing a holistic, multidisciplinary approach for treating and supporting this population. Helping providers understand the cultural circumstances surrounding FGM/C and providing them with actionable steps for improving cultural competence, including communicating with empathy, has the potential to reduce disparities that exist in dimensions of race, ethnicity, and gender.
Evaluating/Monitoring Toolkits to Improve Quality and Utility
Existing research suggests that health professionals prefer toolkits that have been tested and demonstrated as effective. 31 None of the 31 toolkits directed to the health sector, in conjunction with other audiences in some cases, included information about the toolkit’s effectiveness, or a strategy to evaluate if the toolkit as an intervention resulted in improved care delivery or health outcomes. Developing and employing a toolkit evaluation plan can help determine ways to improve service capacity for affected populations. Furthermore, use of data to monitor implementation progress can help build the case for practice improvements that are evidence-based.
Similar to recent research,24,55 our findings show a need for more digital tools that can help health care providers in the United States readily access reliable information about FGM/C and accurately document cases. However, a practical question exists as to whether and to what degree information made available through toolkits would be used by providers. In this regard, we recommend practitioners evaluate toolkit use, as doing so is the only way to learn contextual factors, including policies, resources, and access to care, that may affect implementation and health outcomes in affected groups. This is an area of limited research that also calls for exploring ways collaboration among providers can aid in integrating an FGM/C toolkit at the system level.23,31 As existing toolkit research suggests, data are vital for identifying gaps, updating prevalence and incidence statistics, and facilitating or systematizing care delivery.24,29,30,55 We recommend that toolkits be subject to evaluation and monitoring to improve their quality and utility.
Web-Accessible Support for Affected Women and Girls
Women who undergo FGM/C can experience significant negative psychosocial and physical health consequences that need informed, specialized care. Toolkits can be instrumental interventions for sharing health information, supporting clinical practice, and improving providers’ communication and attitudes toward FGM/C that factor into women’s reluctance or willingness to seek medical care or psychotherapy.23,26,54,68 If directed to women who have experienced FGM/C, in addition to health care providers, toolkits can be supportive and accessible to this population, and aid immigrant and refugee communities through the provision of resources and information.
In our sample of 45 toolkits, we found only one that offered mental health services directly to individual women with FGM/C and girls at risk of FGM/C. This is in line with prior findings,54,55 and one review in particular that found health-related training and research “reference materials scored poorly on the sexual and psycho-social impacts of FGM/C.” 67 We recommend the provision of online information for health professionals working with groups affected by FGM/C be expanded to provide direct support and psychological services to individual women and girls, as the paucity of such support has been documented.69,70 Women living with FGM/C and their families could benefit from online support programs for mental health and sexual counseling, and awareness of community resources.
Limitations and Strengths
We located and accessed toolkits in the time period of January to March 2018. It is likely that more FGM/C-related materials, both labeled and not labeled as toolkits, have been published online since then. Additionally, we limited our search to toolkits available in English. Doing so likely curtailed the number of toolkits in our sample, compared to if we had included non-English sources. We also did not compare our sample using Google against other search engines, to assess the validity of our results.
We note that this study also has distinct strengths. First, our search was purposively broad to capture toolkits on FGM/C that have been issued in realms apart from health care, but that critically intersect with health, such as government, law, community, and education, and must work with the health sector to improve outcomes. Second, it provides a first-ever profile of existing web-delivered toolkits that aim to offer information and resources in connection with preventing, managing, and responding to cases of FGM/C. No studies to date have researched FGM/C guidance for this purpose. In this sense, our study forms the basis for future research on ways to improve the quality and use of web-based resources on FGM/C, and to monitor and evaluate their application in practice.
Implications for Practice and Policy
This review can benefit many health professionals, including medical students, physicians, nurses, midwives, social workers, psychiatrists, women’s health specialists, and pediatricians. Health care administrators and policy advisors also can benefit from understanding the diversity of toolkit-oriented information available online, in consideration of strategies to improve health practice and prevent unhealthy outcomes for affected women and girls. Furthermore, this review is relevant for community practitioners working to design and implement health promotion programs and tools related to care management of FGM/C.
In the domain of health, our review of web-based resources suggests a need for skills development, guidance, and tools that providers can use to provide optimal care for women and girls with FGM/C. From our review, the expanse of web-based materials on FGM/C provides an opportunity to find ways to improve future toolkits to support practice with, for example, the inclusion of research-backed information, online resources for affected groups and practitioners who provide counselling and psychological services to women and girls, and monitoring the implementation of FGM/C toolkits as interventions. Health care providers are essential in the care and management of sexual, reproductive, and psychosocial sequelae of FGM/C. More availability of reliable, easy-to-access toolkits can help providers improve quality of service and meet challenges in providing care to culturally diverse groups of women and girls. In this regard, future research should explore the implementation of FGM/C toolkits as potential quality improvement measures aimed at enhancing patients’ health experiences and outcomes.
Additionally, future research should examine the availability of FGM/C toolkits in Asian and African countries, given increased efforts in these regions to ban the practice and use of community-level programming and delivery of primary care, particularly for women and children. Further, our study highlights the development of FGM/C toolkits mostly in high-income countries. A comparison of similar toolkits in low-resource contexts would be useful, and could serve as a basis for promoting the use of toolkits to address sectoral training and capacity gaps and to provide accessible clinical guidance for managing FGM/C-related care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported under Grant 1 ASTWH160035-01-00, titled “Development and Testing of a Community Centered FGC Prevention Project,” awarded by the Office on Women’s Health within the US Department of Health and Human Services. The funders were not involved in the collection, analysis, or interpretation of data. The findings and conclusions in this study are those of the authors and do not represent the position of the funders.