
Abstract
Introduction
Cardiac rehabilitation (CR) following a cardiac event is safe, delivers quality health outcomes and is cost effective.1,2 One of the core components of comprehensive CR is the promotion of lifelong engagement in physical activity (PA) through behavior counseling and exercise training. Despite strong evidence showing a positive correlation between achieving PA recommendations and a lower CVD risk,3-5 referrals to, uptake of, and long-term engagement in cardiac rehabilitation remains low globally.1,6-10
Major health care organizations recommend that CR patients consistently accumulate 30 to 60 minutes of moderate intensity PA per day on more than 5 days of the week and minimize the amount of time that is spent in sedentary behavior (SB). 3 However, even the majority of healthy older adults do not attain these levels of activity. 11 Nevertheless, the health benefits of cardiac rehabilitation appear to exist regardless of the type of cardiovascular disease, whether a patient is prescribed exercise only or comprehensive cardiac rehabilitation, the dose of exercise, when follow-up occurs, whether one exercises at home or at a center or the geographic location the intervention takes place in. 12 This raises a question as to whether or not PA levels change following CR.
There have been 3 systematic reviews investigating the effect of CR on PA and SB.13-15 Dibben et al 13 assessed whether any form of CR changed PA, measured using both subjective and objective methods of assessment. The authors showed with a meta-analysis that CR increased the percentage of participants categorized as physically active in the short and long term. The same was true for SB at a long-term follow-up. 13 Another review and meta-analysis 14 investigated the effect commercial wearable devices with exercise advice had on PA and SB 4 weeks after having taken part in a form of phase II CR, that is, during phase III CR, including exercise and/or counseling and education. These authors found that wearable devices were better for increasing PA in phase III CR compared with wearing no device, but there was no influence on time spent in SB. A third systematic review 15 included studies investigating the impact of center- and home-based, exercise-based, psychosocial and education-based CR on PA measured both objectively and subjectively. They found that home-based CR had better long-term effects compared with center-based CR for improving and maintaining PA levels, and showed that modifying the type of CR had no additional benefit.
The aforementioned reviews all focused on a variety of different components of CR and activity behaviors. Most studies included in the reviews reported activity behaviors using subjective measures, which can introduce bias due to overestimation of patient self-reported activity. 16 Furthermore, although guidelines for the management of SB in people attending CR have not yet been established, there is a body of evidence that suggests sedentary behavior is an independent risk factor for cardiometabolic disease.17-19 Although the interdependence of the relationship between SB and health is not quite clear, 20 time spent in the behavior should be reduced as much as possible. 21 It is not clear whether SB decreases following CR as few studies have measured this behavior objectively. Sedentary behavior level measurement following CR is important as it may be an alternative behavior to incorporate into the behavior counseling in patients during CR.
The current review sought to specifically identify only studies that included objective measures of PA and SB following participation in some form of exercise-based CR in order to synthesize the evidence and evaluate the effectiveness of exercise-based CR on PA and SB in adults with cardiac conditions. This review aimed to include an assessment of PA and SB immediately following phase II CR as well as to assess whether effects were maintained during a long-term follow-up of PA and SB, that is, in phase III CR. Meta-analyses were also performed to quantitatively determine the overall effect size of exercise-based CR on combined habitual activity levels immediately after attendance at CR and, where possible, in the long term.
New Contribution
Patients attending exercise-based CR increase participation in positive activity behaviors in the short and long term compared with receiving standard care without exercise training. Consensus on the optimal type and combination of activity outcomes, and how they are measured, is needed to support the conduct of high-quality trials into the effects of CR on activity behaviors.
Methods
The systematic review identified studies that measured PA and/or SB change using objective methods only in adults before and after exercise-based CR in any country. The review protocol was registered with the International Prospective Register for Systematic Reviews with registration number: PROSPERO 2019 CRD42019124971 (https://www.crd.york.ac.uk/prospero/). The review adhered to the reporting guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Supplementary Table S1).
Databases and Search Strategy
A comprehensive systematic search of the literature was performed by 2 reviewers (RMM and KT) in March 2019. Five databases were searched: PubMed (using best match instead of most recent), Medical Literature Analysis and Retrieval System Online (MEDLINE) (Ovid), Scopus, SPORTDiscus, and Cumulative Index to Nursing and Allied Health Literature (CINAHL) under the referencing system EBSCOHost. The literature search was conducted with medical subject headings (MeSH) and keywords in the title, abstract, and text for the population, intervention, comparator, and outcomes (PICO). The MeSH and keywords utilized in the searches were assembled into 15 sets of 3 MeSH and keyword combinations that all consisted of “Cardiac Rehab*” with the following keywords “Physical Activity,” “Accelerometer,” “Exercis*,” “Sedentary Behavio*,” “Pedometer,” “Objectively Measured.” This systematic review was conducted on published studies in the English language from inception to 2019. A final search was conducted from references found in literature reviews that related to topic of interest. Last, the reference list of systematic reviews found during title screening were examined for additional studies to be included in this systematic review. Duplicates of articles retrieved in the search were removed.
Study Eligibility Criteria
Longitudinal, pre-post, experimental studies (with or without control groups) that measured PA and/or SB using objective methods only, in adults before and any time after exercise-based CR were included in the review. Objective measures of PA and SB included accelerometers or pedometers. Studies were included if PA and/or SB was objectively measured prior to the onset of CR, after completion of CR and/or if they included a follow-up after cessation of the CR program. Studies were included if exercise training was conducted in a hospital-based (supervised) and/or free-living or community-based setting (unsupervised). Studies were excluded if they measured PA and/or SB subjectively using self-report and/or questionnaires or if they did not use a structured exercise program as the primary intervention, that is, studies using tele-rehabilitation or behavior change interventions only. Studies that did not explicitly state that they measured PA and/or SB before the onset and after the cessation of a CR program, that is, studies that only measured PA during the CR program were also excluded.
Study Selection
Two reviewers (KT and RMM) independently selected articles based on title, abstract, and full text articles. Disagreements of article selection based on title were resolved by discussion. Article selections were based on abstract and a third reviewer (LB) adjudicated full texts at each stage to resolve the disparity in article selection between the 2 primary reviewers.
Data Extraction
Two authors (RMM and KT) agreed a priori on which data to extract from the included articles. Data extraction from the included articles was performed using a predetermined data extraction sheet by one author (KT) and cross-checked for accuracy, detail, and consensus by the remaining authors (RMM and LB). For each included article, the following data were extracted, summarized, and presented in tables: study design, sample size, demographics, and pathology of included study participants; characteristics of the CR program with assessment time-points, type of accelerometer, the placement of the device, and the protocol used; outcome measures of objectively assessed PA and SB; and study findings. Data on compliance to the intervention and whether additional educational sessions or behavior counseling were included as part of the CR program were also extracted.
Critical Appraisal of Methodological Quality
The methodological quality of included studies was assessed using the Scottish Intercollegiate Guidelines Network (SIGN) checklist 2 for controlled trials or checklist 3 for cohort studies. Two authors (KT and RMM) assessed the risk of bias of the included studies. Agreement on the final ratings was reached by discussion between these 2 authors and adjudicated by the third author (LB).
Data Synthesis and Analysis
A descriptive synthesis of the evidence was undertaken by tabulating the main findings of each study; means, standard deviations, medians, interquartile ranges, confidence intervals, and P values were extracted. Meta-analysis (Comprehensive Meta-Analysis Version 3, Biostat) was conducted separately for pre- to immediate post CR follow-up points, pre- to immediate post CR in studies comparing with a control group, and pre- to long-term follow-up points where these data were collected. A random-effects model was used to account for external influences on the intervention outcomes between studies. 22 Individual study results were combined where more than one PA/SB outcome measure was used, and reported as standardized mean differences (SMDs) with 95% confidence intervals (CIs). Using SMDs allowed the studies to be combined on a uniform scale to account for variability observed in each study (ie, difference in mean outcome/standard deviation of the outcome). Within studies that had more than one intervention,26,36 or follow-up period,25,26,30,36 each intervention was entered into the meta-analysis separately. Effect sizes associated with these SMDs were allocated as follows: >0.8 large, 0.5 to 0.79 moderate, and 0.2 to 0.49 a weak effect. 23 Heterogeneity between studies was assessed using the I2 statistic, where <25% indicates low risk, 25% to 75% indicates moderate risk, and >75% indicates high risk of heterogeneity. 24 Data are presented using Forest plots. In the plots, the squares represent point estimates of treatment effect (larger squares indicate larger samples), the horizontal lines (whiskers) are 95% CIs and the diamond represents the pooled treatment (summary) effect, while the vertical lines represents the size of the SMD and 95% CIs.
Results
Study Selection
A total of 876 articles were obtained from the initial electronic databases search excluding duplicates. An additional 17 were included through reference list searches. Titles of these 893 articles were screened and after adjudication, 146 articles were selected for further abstract screening. Abstract screening (RMM and KT) resulted in 26 articles selected for full text assessment. Full text screening resulted in 15 eligible studies for the final data analysis (Figure 1). Titles of the excluded full text screened studies with reasons are presented (Supplementary Table S2).

Flowchart showing the method of selection of studies included in the final analysis.
Methodological Quality Assessment
Of the 4 cohort studies, 3 were of acceptable quality while 1 was deemed low quality. Most randomized controlled trials were of acceptable quality. The most common risks of bias were inadequate concealment methods or concealment methods not mentioned, and participants and investigators not blinded to treatment allocation. Additionally, another common weakness was that intervention and control groups were not similar at baseline (6/11 = 55%). The results of the SIGN assessment appear in Supplementary Tables S3 and S4.
Characteristics of Included Studies
A total sample size of 1434 participants were recruited into the 15 studies and entered into an exercise or control group. Approximately 80% of participants were male (1150) and 20% were female (294). The mean ages of the participants ranged between 54.8 and 79.5 years.
A detailed description of the design and participant characteristics in each study appears in Table 1. Of the included studies, 4 were prospective cohort studies25-28 and 11 were randomized controlled trials29-39 published between 2004 and 2019. The study by Ribeiro et al 35 was a subanalysis of 2 randomized controlled trials.
Study Characteristics.

Abbreviations: CR, cardiac rehabilitation; RCT, randomized controlled trial; IG, intervention group; CG, control group; NYHA, New York Heart Association; NR, not reported.
Age reported as mean (SD) or mean [range].
Standard deviation not reported.
Not reported if % is for baseline number of participants or those who completed the intervention.
Data for patients only and not spouses.
Three studies were conducted in the Netherlands,28,36,37 2 in Portugal,33,35 2 in Belgium,31,32 2 in the United States,27,39 2 in Canada,26,34 1 in Australia, 25 2 in the United Kingdom,30,38 and 1 in Sweden. 29 The patient profile within the studies included patients with heart failure (mostly systolic dysfunction, NYHA [New York Heart Association] class II and III) with reduced or preserved ejection fraction,29,30,37,38 those who had been diagnosed with coronary artery disease, ischemic heart disease, and/or acute coronary syndrome and who were treated for such including via coronary artery bypass grafting or revascularization surgery.25-28,31-36,39
Characteristics of the Exercise-Based Cardiac Rehabilitation Programs
The descriptions of the CR programs, compliance to the intervention, and whether additional educational sessions or behavior counseling was included as part of the CR program are presented in Supplementary Table S5. The duration of CR exercise programs ranged from 4 to 8 weeks with a frequency of visits between 2 and 3 times per week. Nine out of the 15 studies included a follow-up after the intervention,25,28,30-32,36,38,39 which ranged between 18 weeks and 18 months. Exercise sessions lasted between 15 and 60 minutes. All studies involved aerobic exercises with 6 including balance and/or resistance training.28,29,34,36,38,39 Five studies did not specify either the mode of exercise or the intensity of training.25,27,28,31,34 Ten studies incorporated education and counseling sessions on improving lifestyles, PA and its consequences, strategies on improving PA and improving lifestyle and diet (Figure 2).25,26,28,30-32,34-36,38,39 All but 2 studies29,36 reported intervention compliance results.

Heat map of changes in physical activity (PA) and sedentary behavior (SB) immediately after and at the long-term follow-up after cardiac rehabilitation by type of study. Whether each study included a behavior intervention or counseling in addition to exercise as part of their cardiac rehabilitation is also included. Red, no; Green, yes; no color, not applicable/not reported.
Summary of Physical Activity and Sedentary Behavior Outcomes and Changes
A range of accelerometer devices were used to measure PA and/or SB, the most common being the ActiGraph accelerometer. The accelerometers were worn for periods ranging from 2 to 7 days prior to the start of, and after CR, to a full 12 weeks of continuous consecutive wear during the study. 32 Five out of the 15 studies included some measure of SB as an outcome. A description of the accelerometer protocol for each study, the data reduction methods applied, and the main activity outcomes findings is presented in Table 2.
Study Accelerometer Protocols and Main Activity Outcome Findings.
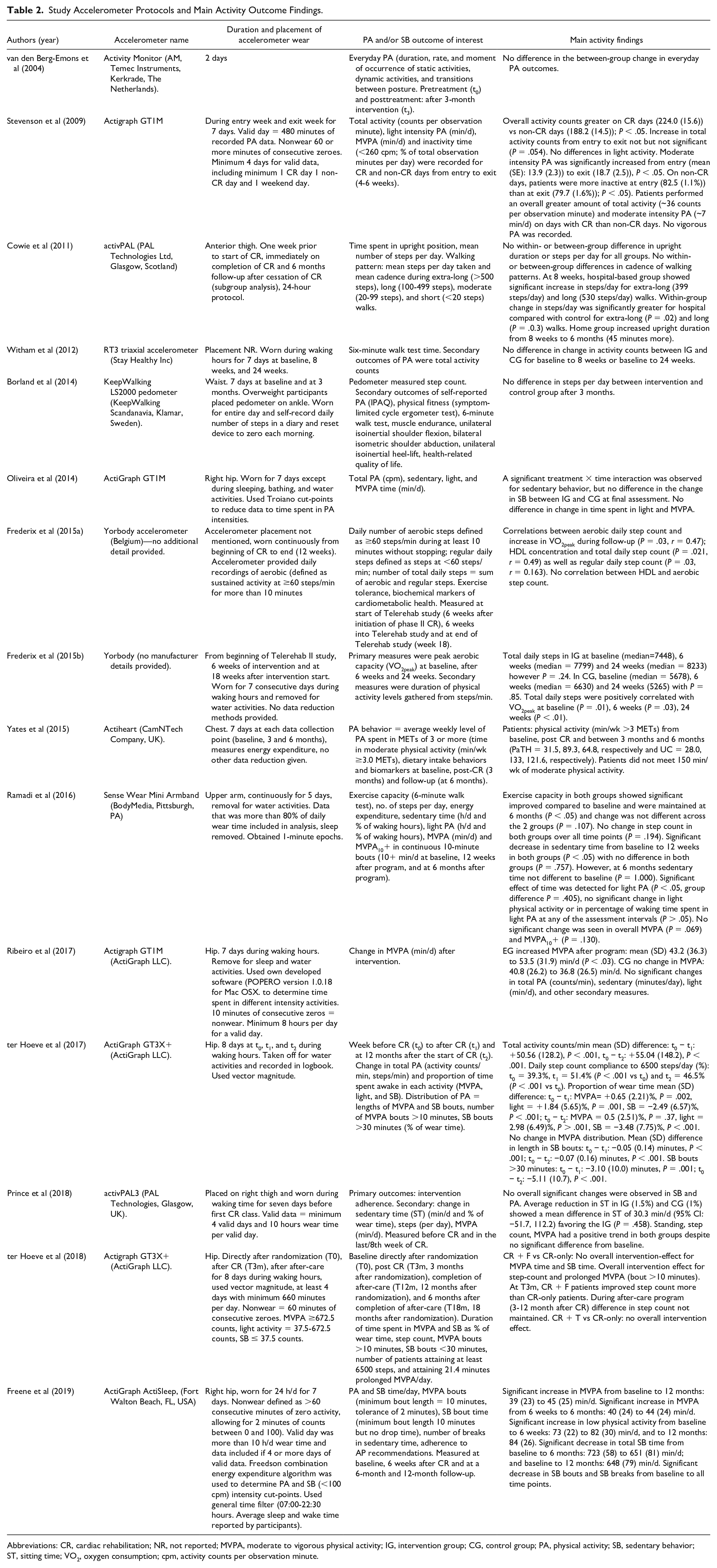
Abbreviations: CR, cardiac rehabilitation; NR, not reported; MVPA, moderate to vigorous physical activity; IG, intervention group; CG, control group; PA, physical activity; SB, sedentary behavior; ST, sitting time; VO2, oxygen consumption; cpm, activity counts per observation minute.
Eight out of the 15 included studies showed a significant improvement in PA outcomes while 7 studies reported that objectively measured PA did not change immediately following the intervention compared with preintervention levels and/or compared with the control group (if relevant) (Figure 2). One study did not report on whether the actual change in PA was significant following the intervention, rather they showed that there was a correlation between aerobic daily step count and VO2peak which increased significantly in the intervention group. 31 Of the 7 studies that reported changes in SB, 4 observed a significant change immediately following CR25,26,28,33 while 3 did not34-36 (Figure 2). Of the 4 studies that observed a significant reduction in SB immediately after CR, three studies assessed SB outcomes at a long-term follow up.25,26,28 All 3 studies were prospective follow-up studies with no control group. One study found that the SB decrease was maintained at a 1-year follow-up, 28 while the other found that the six month SB level was comparable to baseline. 26 The third RCT followed up their patients 6 and 12 months after CR and found that at both time points patterns of SB were significantly decreased compared to baseline levels. 25
Meta-analysis
Of the total number of studies meeting inclusion criteria, there were 11 that provided data for meta-analysis. The pooled data from nine studies reporting a pre- to postchange in PA and SB indicated that cardiac rehabilitation produced a moderate effect on activity behavior (SMD 0.50, 95% CI 0.25-0.55, P < .0001). Heterogeneity was high (I2 = 78.4%, P = .001). The forest plot is shown in Figure 3.

Forest plot of effect sizes for studies of pre-post exercise-based cardiac rehabilitation. The overall point estimate revealed a small effect favoring greater objective physical activity (PA) and sedentary behavior (SB) immediately following exercise-based cardiac rehabilitation. Arrow denotes the effect was greater than 1.
The pooled data from 5 studies comparing an intervention and control group indicated with a weak effect that cardiac rehabilitation resulted in a greater improvement in activity behaviors in the intervention compared with the control group (SMD 0.25, 95% CI 0.02-0.49, P = .04). Heterogeneity was low (I2 = 0%, P = .95). The forest plot is shown in Figure 4.
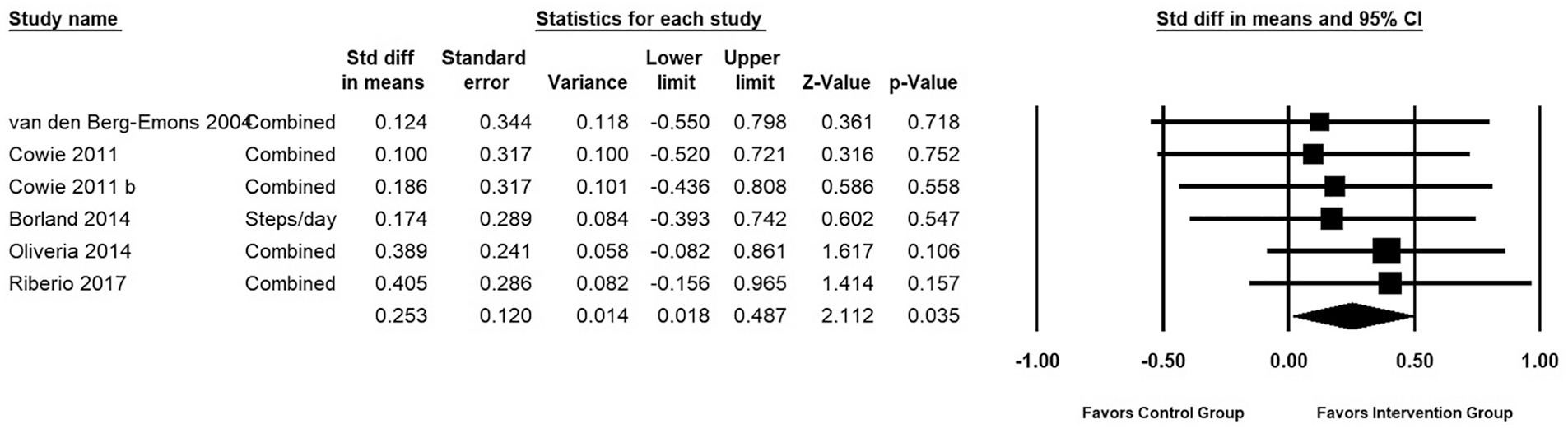
Forest plot of intervention versus control group for the change in activity behaviors following cardiac rehabilitation. The overall point estimate revealed a small effect favoring structured exercise-based cardiac rehabilitation versus nonexercise or alternative control interventions on objective physical activity (PA) and sedentary behavior (SB).
The pooled data from 5 studies that included a longer term follow-up indicated improved activity behaviors were maintained but this was associated with a weak effect (SMD 0.32, 95% CI 0.22-0.41, P < .0001). Heterogeneity was moderate (I2 = 70.3%, P < .0001). The forest plot is shown in Figure 5.

Forest plot of studies that included a long-term follow-up of activity outcomes versus baseline. The overall point estimate revealed a small effect favoring greater objective physical activity (PA) and sedentary behavior (SB) at longer term follow-up after completion of exercise-based rehabilitation.
Discussion
PA and SB have well-documented associations with cardiovascular health outcomes,17,18 and as technology to measure these behaviors improves, research has emerged into whether cardiac rehabilitation modifies PA and SB. This current systematic review included 15 studies that investigated whether taking part in an exercise program as part of CR improved objectively measured PA and SB in patients diagnosed with and/or recovering from cardiovascular disease. Overall, it appears that taking part in exercise-based CR favors improvements in objectively measured PA and/or SB immediately following rehabilitation and when compared with a control group. Half of the studies that assessed changes in SB, showed an improvement in SB while the other half showed no change. An additional aim of this systematic review was to determine long-term changes in PA and/or SB following participation in exercise-based CR. Overall in the long term, participants who attended exercise-based CR appeared to sustain their increased engagement in positive activity behaviors, as shown by the meta-analysis. Two studies measuring long-term improvements in SB after CR showed reductions in SB were maintained for at least a year.
Our results are slightly different to those of a previous systematic review 13 that analyzed PA outcomes from studies using both objective and subjective measurements. Although the outcome variables used in this current meta-analysis were pooled, as there were too few studies measuring the same construct in the same way to allow individual analysis, the previous systematic review stratified their results by type of activity outcome measure. 13 While we found that overall there is a moderate but significant increase in PA in general, Dibben et al 13 found no effect of CR on the time spent sedentary, in light, moderate or vigorous activity. However, the authors of the latter study reported that CR participation was associated with an increase in objectively measured daily step count. The most obvious explanation for the difference in findings is the fact that we excluded self-reported measures of PA because of the known bias in self-reporting PA levels, 16 a limitation that was confirmed by the authors of the previous review. Nevertheless, when considered together the results of both reviews are promising especially for long-term changes in PA behaviors following CR.
The moderate to high heterogeneity observed in the meta-analysis for the pre-post studies and those that included a long-term follow-up, may result from the large number of different activity outcomes measured in the studies, the differences in the exercise-based program protocols as well as the number of participants at each time point within and between each study. Although combining PA and SB outcome measures may also have contributed to the heterogeneity in the meta-analysis due to them being slightly different constructs, considering that the 2 behaviors are naturally correlated it made the most sense to combine them as an outcome of total activity behavior change in the positive or negative direction. Treating them as independent variables when they are related constructs would affect the size of the point estimate and significance. In the pre-post analysis, the high heterogeneity across studies is most likely due to variation in exercise-based CR protocols that were delivered (eg, frequency, duration, and intensity of exercise, home vs clinic-based, aerobic plus strength vs aerobic only), even though there was a moderate effect size for the intervention. In the meta-analysis for the intervention versus control, there was low heterogeneity across studies, likely because both groups were exposed to similar environments within each individual study and the same outcomes were measured for both groups. Thus, the magnitude of changes between control and intervention groups was consistent between studies. However, there was only a weak effect on overall change in activity outcomes between groups. For the meta-analysis of studies that included a long-term follow-up, we also found moderate variability in sample estimates between studies, again possibly due to the different types of exercise-based CR intervention protocols and outcome measures utilized. While statistically significant, the pre-post difference for long-term follow-up were accompanied by a small effect size. The heterogeneity observed when combining studies investigating CR intervention studies emphasizes the vast differences in exercise-based CR approaches, making it difficult to determine whether one approach is better than another, and the overall impact of CR on objectively measured PA and SB.
The short- and long-term health benefits of CR seem to exist regardless of the type of cardiovascular disease, whether a patient is prescribed exercise only or comprehensive CR, the dose of exercise, length of follow-up, whether one exercises at home or at a center, or the geographic location of the intervention.
40
Given this, adherence to exercise prescription in the long term is difficult for some patients and uptake of phase III CR is often poor.7,41,42 Frequency, duration, and intensity of exercise additionally differed between studies in this review, and whether these variables play a significant role in determining individual engagement in long-term positive activity behaviors for health remains to be elucidated. A study by Ayabe et al
43
objectively measured patient activity level during exercise-based CR and found that patients achieved their PA targets during the time (7
Seven studies assessed SB as an outcome measure following participation in exercise-based CR. It is important to note that there were many different definitions and measures of SB outcomes and/or data reduction techniques across these studies. In both studies led by ter Hoeve,28,36 an Actigraph GT3X was used, which does not distinguish between active standing and being sedentary. Stevenson et al 27 classified inactivity as being <260 cpm (activity counts per observation minute) measured with an ActiGraph GT1M, which may have included the <100 cpm, which typically defines time spent being sedentary when measured with the GT1M. Given that the definitions as well as the physiology between inactivity and sedentary behavior appear to be different,18,45 these misclassifications may have ramifications for studies using different definitions of activity and their conclusions on health outcomes. Only 1 study 34 used the activPAL in the assessment of SB, which is currently the most accurate monitor to do so. 46 Data from the intervention group was excluded from this meta-analysis because the intervention group had their SB constantly interrupted with another device that gave alerts to participants when they were sedentary for too long. However, it is interesting to note that the alerting device had no additional effect on reducing SB compared with the control group who only participated in exercise-based CR for the duration of the 8-week intervention. This finding appears to indicate that SB may not be modified following CR. However, there are not enough studies on the effect of exercise-based CR on SB to provide a definitive answer at this time and more studies using the activPAL to quantify SB are needed.
Activity behaviors occur as a continuum throughout the day and previous research has analyzed compositions of activities in a day (ie, proportions of SB, light, and moderate to vigorous physical activity [MVPA]) and found associations between certain compositions and better health outcomes in adults. 47 There is currently a lack of research on the effect that holistically modifiable behaviors (ie, enhanced light and/or MVPA in combination with reduced SB) have on the health of patients with cardiac disease. It is therefore interesting to note that in the study by Ribeiro et al, 35 the exercise group significantly increased their participation in MVPA following CR. Although not statistically significant, the control group (who received usual care and education) reduced the amount of time spent in SB by almost 19 minutes per day (95% CI −43.0 to 5.7) and increased their time spent in light activity by an additional 28 minutes per day (95% CI −0.4 to 57.2). These findings indicate future research may wish to consider the effect of exercise-based CR on combinations of behaviors and their impact on health outcomes.47,48 Overall, our findings justify the need for more consensus on what the most relevant and modifiable activity behavior combinations may be following exercise-based CR, the most optimum way to measure them, and to elucidate the effect of those combinations on health outcomes in this patient population. The most relevant and modifiable activity behavior combination, is currently a potential avenue of research for trials on exercise-based CR.
Clinically, this would mean advising individuals on multiple activity behavior changes rather than individual activity intensities, that is, increasing MVPA. A more pragmatic and holistic approach for individuals may increase the uptake and compliance to engagement in physical activity for health in those with cardiac conditions.
Strengths and Limitations
The main strength of this systematic review is that we excluded studies that did not explicitly state that activity behaviors were measured before the onset of and after the cessation of the CR program. Furthermore, we only included studies that reported objective measures of PA and SB, providing outcomes that are not biased by subjective recall. One limitation of this systematic review stems from the heterogeneity of included studies. 49 For example, different interventions were used and compared with “a traditional CR program” which itself varied by frequency, mode, and intensity of the CR exercises, education and counseling, follow-up sessions, model of accelerometer, and when the outcome measures were obtained. Another limitation is that only a few studies measured SB, and so PA and SB outcome measures were combined, which did not allow separate conclusions to be drawn between an increase in PA and a reduction in SB.
Furthermore, conclusions of a systematic review depend on the quality of the included studies. Limitations to the internal validity of the studies included in this review were that many studies could not blind those who were administering the intervention; however, most studies at least included a blinded outcome assessor. Furthermore, some studies did not exclude participants who had already attended another cardiac rehabilitation program prior to starting the intervention. Activity levels may have been different between participants at baseline across within studies, and this may have influenced the magnitude of change in PA and/or SB due to the CR program.
More trials monitoring home-based CR and activity are needed to delineate whether it is the intervention or the constant attention of having an intervention delivered in a laboratory setting that drives the improvement in PA engagement post CR program. Comparisons in activity behaviors between home- and center-based CR programs should be undertaken, particularly with multiple follow-ups as there little long-term data for how CR delivery mode influences habitual activity.
Supplemental Material
Supplementary_File – Supplemental material for The Effect of Exercise-Based Cardiac Rehabilitation on Objectively Measured Physical Activity and Sedentary Behavior: A Systematic Review and Meta-analysis
Supplemental material, Supplementary_File for The Effect of Exercise-Based Cardiac Rehabilitation on Objectively Measured Physical Activity and Sedentary Behavior: A Systematic Review and Meta-analysis by Rebecca Mary Meiring, Kento Tanimukai and Lynley Bradnam in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.