
Abstract
Keywords
Introduction
Over the next 10 to 15 years, the United States could need an estimated 40 000 to 60 000 more primary care physicians. 1 Primary care physicians serve on the front lines of care, in many instances providing comprehensive care to patients who may have difficulty accessing subspecialty care. Reasons for the primary care physician shortage are multifactorial, from negative perceptions of the field to new placements not exceeding the retirement rate of primary care physicians currently in practice. Common perceptions of primary care are that it is less interesting and not as academic as other specialties, with limited ability to attain professional growth or earn higher salaries. 2 From 1965 to 2010, the number of generalist physicians decreased from 58% to 32% 3 despite an increasing US population. As of 2016, less than 1 in 4 medical students went on to primary care practice, and less than 5% of resident physicians chose to practice in rural communities. 4 It is clear that primary care involves complex problem solving, long-term doctor-patient partnerships, and dealing with a wide array of medical concerns. Primary care physicians care for the whole patient, providing all-inclusive care that can affect not only the health of individual patients but also the health of families and communities. 5
The problem of the physician shortage is more severely felt in rural communities. Even where there are federally qualified community health centers and other rural practices, there is longstanding medical need. 6 When a physician chooses to become part of a rural community—live there, raise a family there, and serve the community as its local physician, a lifelong commitment of service is made. Drivers of the decision to practice in a rural community include education indebtedness, resource availability, and practice sustainability. 7 This brand of physician can be hard to come by and usually has rural-oriented personal characteristics such as being from a rural community or experiencing well-planned and well-executed clerkships with rural communities that influence the decision to return.7,8 Southern states like North Carolina feel the burden of the shortage of primary care physicians. With 70 of the 80 rural counties in North Carolina experiencing a primary care physician shortage, access to quality health care can be difficult. These statistics underscore the concern that the fee for service health care model is unaffordable, 9 but paying for health care under a value-based model and keeping people healthy provides opportunity for improvement.
Of the 29 counties in eastern North Carolina, all but one (Pitt county) are rural, and all but Pitt county, Dare county, and half of Beaufort county suffer most from the lack of primary care. Eastern North Carolina is poorer, more rural, more diverse, and oftentimes sicker than the rest of North Carolina and much of the United States.10-12 In comparison to the rest of the state, people in eastern North Carolina have lower educational attainment, which can translate to lower wages and higher unemployment rates, 11 complicating the health problems of community residents.
There is a medical school in eastern North Carolina that is working to improve the health of the state and region by increasing the number of primary care physicians. The Brody School of Medicine at East Carolina University (ECU) has a mission to increase the supply of primary care physicians serving the state, improve the health status of the citizens of eastern North Carolina, and enhance access of minority and disadvantaged students to a medical education. 12 Brody is a community-based, rural-focused, mission-minded medical school that only accepts applicants from the communities of North Carolina. 12 For this reason, it could be referred to as “the medical school for North Carolina.” Brody has been recognized by the American Academy of Family Physicians (AAFP) for its work in producing family physicians, being named number 1 in North Carolina and number 2 in the nation for the percentage of graduates who choose family medicine as their specialty. 13 Brody also ranks as a top school for retention in primary care five years after graduation, and, of the over 300 family medicine residency program graduates since 1980, over 60% practice in the state.14,15 To characterize the impact of Brody on the primary care physician supply in more detail, the authors sought to determine how Brody compares with other North Carolina medical schools on matching medical students in primary care specialties, including family medicine, internal medicine, medicine-pediatrics, and pediatrics.
Methods
The 4 allopathic medical school members in the state of North Carolina were selected for this study: Brody School of Medicine, University of North Carolina (UNC) Chapel Hill, Duke School of Medicine, and Wake Forest School of Medicine. These medical schools vary in mission, location, enrollment, and number of graduates (Table 1). For each school, residency match results from 2014 to 2018 were queried by consulting school websites, or, in the case of Wake Forest, by requesting the data from the Office of Student Affairs. Primary care specialties were defined as family medicine, internal medicine, pediatrics, and internal medicine/pediatrics. Although obstetrics/gynecology can be considered a primary care specialty in some contexts, it was not defined as such for the purposes of our analysis. Chi-square tests and Fisher’s exact tests were used to compare the proportion of graduates from each school matching to a residency program in each primary care specialty, and to any of the 4 primary care specialties.
Characteristics of Allopathic Medical Schools in North Carolina. a
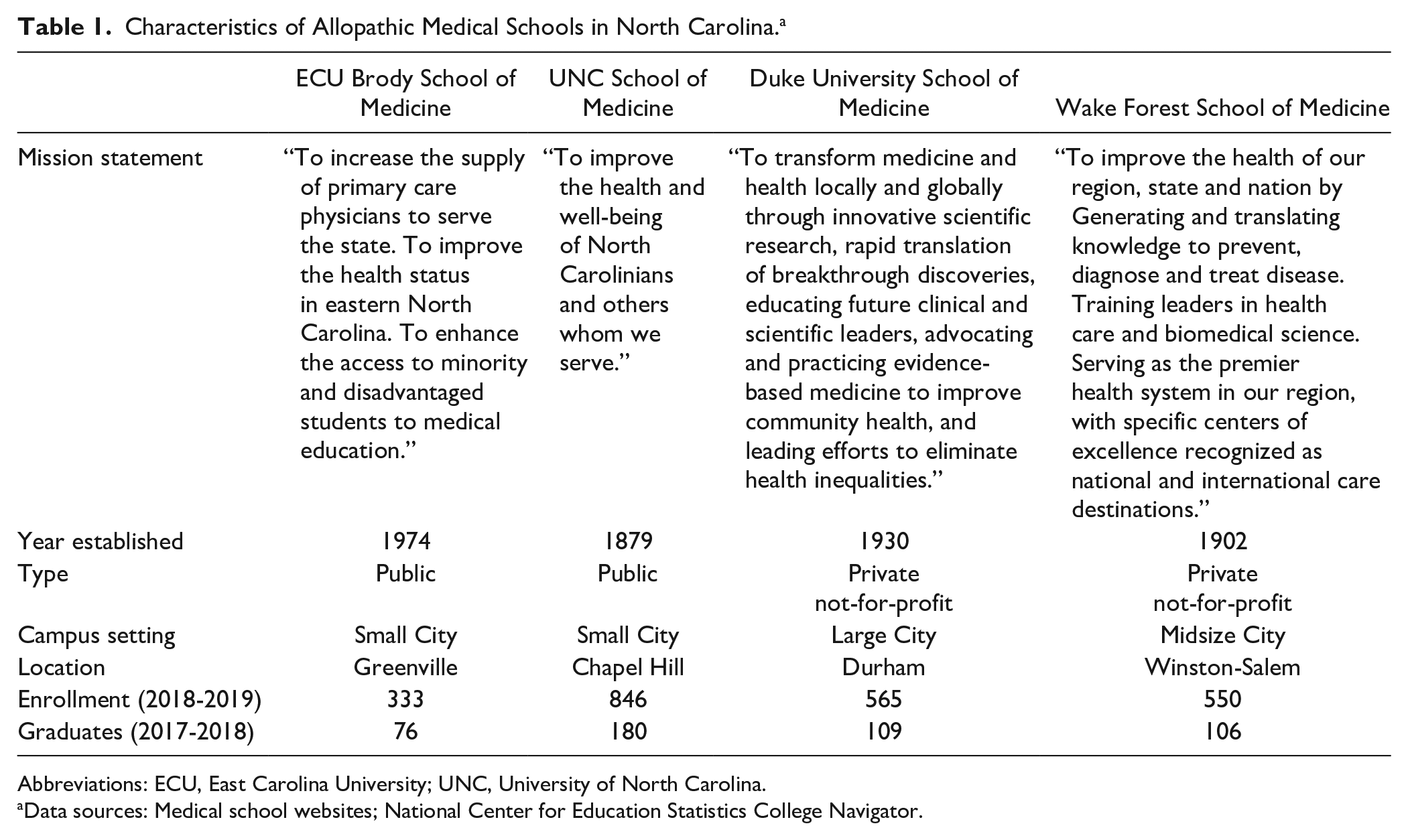
Abbreviations: ECU, East Carolina University; UNC, University of North Carolina.
Data sources: Medical school websites; National Center for Education Statistics College Navigator.
Results
Over the study period, 961 medical school graduates in North Carolina matched to a residency in a primary care specialty (Table 2). The UNC School of Medicine and Brody School of Medicine accounted for 40% and 22% of graduates entering a primary care specialty, respectively, although UNC’s enrollment was much larger during this time. Of the 961 graduates entering a primary care field, 44% matched to a residency in internal medicine, 25% matched to a residency in family medicine, 23% matched to a residency in pediatrics, and 8% matched to a combined internal medicine/pediatrics residency.
Graduates From North Carolina Medical Schools Matching to a Residency in a Primary Care Specialty, by School and Year.
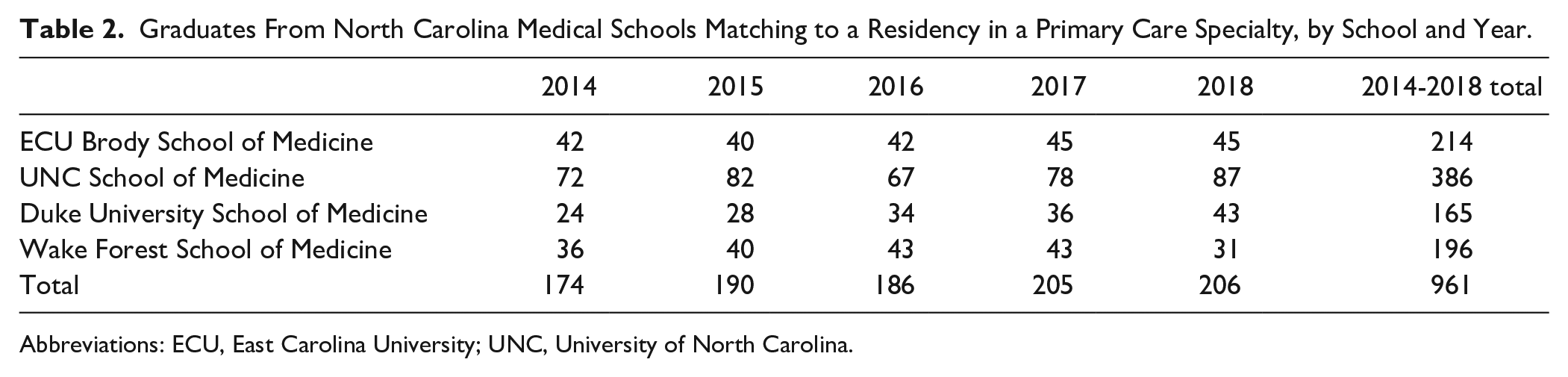
Abbreviations: ECU, East Carolina University; UNC, University of North Carolina.
Table 3 summarizes the comparison across schools in the proportions matching to any residency in a primary care specialty, as well as proportions matching in each specific field. Among the 4 schools, Brody was distinguished by producing the highest proportion of graduates entering any primary care specialty (53%), as well as the highest proportion of graduates matching to a residency in family medicine (16%), pediatrics (6%), and internal medicine/pediatrics (6%). By contrast, Duke had the highest proportion of graduating students matching to an internal medicine residency among the 4 schools (22%).
Residency Matches to a Primary Care Specialty Among North Carolina Allopathic Medical School Graduates in 2014-2018, by School. a

Abbreviations: ECU, East Carolina University; UNC, University of North Carolina.
Values are presented as number (percentage).
While match rates to each specialty varied significantly across all 4 schools, we also specifically compared Brody with UNC, the medical school with the next-highest proportion of graduates entering a primary care field (45%, vs 53% at Brody; P = .007). Brody had a higher proportion of graduates matching to a residency in family medicine (18% vs 13%, P = .015) or pediatrics (16% vs 9%, P < .001). However, UNC had a higher proportion of graduates matching to a residency in internal medicine (19% vs 14%, P = .025). The 2 schools did not significantly differ in the proportion of graduates matching to a combined internal medicine/pediatrics residency (6% at Brody vs 4% at UNC, P = .326).
Discussion
Despite recent expansion of medical schools in the United States, the supply of primary care physicians remains short of current and projected needs.3,16 In North Carolina, the US Department of Health and Human Services (Health Resources and Services Administration) has projected a demand of 8640 primary care physicians and a shortage of 11.6% in North Carolina for year 2025. 17 This study demonstrates the impact of the Brody School of Medicine on producing graduates in primary care, with a significantly higher proportion of its graduating students matching to residency in a primary care field, as compared with the other allopathic medical schools in the state. Particularly, the Brody School of Medicine led all other schools in the state in the proportion of graduating students who matched to a residency in family medicine or pediatrics, 2 of the specialties that have the greatest impact on the primary care physician workforce.
Both individual and institutional factors influence medical students’ match into a residency in a primary care specialty. Among individual factors, interest in primary care, experience during clerkship, and participation in primary care–related interest group or a rural medical education track have all been identified as predictors of matching in a primary care field and eventually entering primary care practice.18,19 While primary care is traditionally considered a less academic area of practice, one study found that participation in a dual MD/MPH program increased the likelihood of primary care practice among graduates of a single institution. 19 In a survey of graduating medical students, Kost and colleagues also found that positive perception of family medicine and favorable expectations for the future of this specialty were associated with increased likelihood of choosing a family medicine residency. 20 These data suggest that providing high-quality clinical and educational opportunities related to primary care may help medical schools maintain a culture of high student interest in primary care, and potentially increase the proportion of students matching to these specialties.
Considering specific institutional factors influencing graduates’ specialty choice, Phillips and colleagues have reported that among allopathic schools, the presence of a family medicine department increases the likelihood of students choosing to pursue residency in family medicine. 16 Among schools with family medicine departments, Wimsatt and colleagues have further reported that public schools, schools with longer clerkships, and schools with at least 1 family medicine physician in a senior leadership role had higher proportions of students matching in family medicine. 21 While these findings point to incremental changes that institutions can make to facilitate training more primary care physicians, the experience of the Brody School of Medicine suggests that a more comprehensive focus on serving the needs of a region or state can produce significantly higher proportion of graduates entering primary care specialties, as compared with other allopathic medical schools in North Carolina.
Among Brody graduates, a high proportion of students entering primary care is matched by high rates of students continuing to practice in rural areas and in North Carolina as compared to other states. Among graduating classes between 1990 and 2015, 48% of Brody graduates were active physicians in 2016 in North Carolina, 22 the highest percentage among other medical schools in the state. Between 4% and 13% of Brody graduates also go on to practice in rural counties 5 years after graduating. 22 This illustrates the success of Brody in producing graduates who enter practice in the areas and locations where the physician shortage is arguably most acute. Some of the distinguishing features of Brody include its community-minded mission, its policy of admitting only North Carolina residents, and the location of its campus in a medically underserved and rural region, a deliberate choice made at the time of the school’s founding. While these characteristics may be too radical or infeasible to implement as changes to other existing institutions, the success of Brody at training primary care physicians offers a template for new institutions to follow as the number of medical schools in the United States continues to expand.
Limitations to this study include the use of publicly available, aggregated data. While similar data have been used to chart the trend of students entering primary care specialties nationwide, 16 in-depth survey or interview data may have provided additional information on students’ motivation to enter a primary care specialty, and how this was fostered or reinforced by their experiences during medical school. A further limitation is that given the recent years of the study, the ultimate practice type and location of many graduates in our study is not yet known. Although the majority of family medicine residents enter primary care practice, this is less often the case for internal medicine or pediatrics residents. 3 Similarly, we could not fully analyze whether graduates in these cohorts entered practice in rural areas or working with underserved populations. Longitudinal and mixed-methods studies may help distinguish specific ways in which Brody helps its graduates launch and sustain primary care careers in rural and medically underserved areas. Last, we analyzed the graduation outcomes of allopathic medical schools in North Carolina, whereas Campbell University, the osteopathic medical school in the state, was excluded due to it not being an AAMC (Association of American Medical Colleges) allopathic medical school and due to it being relatively new and having a limited amount of primary care match data.
Conclusion
The Brody School of Medicine in eastern North Carolina is meeting its mission of service to the state. Not only is Brody the only medical school in the state with medical school classes made exclusively from the communities of North Carolina, Brody is the medical school for the state of North Carolina, with evidence of successes in supplying physicians for the state. Medical schools like Brody should receive increased attention and resources to support their community driven missions and outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.