
Abstract
Background
The World Health Organization (WHO) defines social determinants of health (SDOH) as “conditions in which people are born, grow, work, live, and age, and the wider set of forces and systems shaping the conditions of daily life.” 1 The American Academy of Pediatrics recognizes that these social and environmental factors play a significant role in the health and well-being of children.2,3 Addressing SDOH is complex, but pediatricians have a unique opportunity to identify and address these issues during a child’s formative years. 4 In March 2016, the American Academy of Pediatrics released a policy statement on Poverty and Child Health, which recommends screening for social determinants during the patient encounter. 4 Several SDOH screening tools have been studied and utilized in children.
The Pasadena-Pediatric and Adolescent Health Center (PA-PAHC) is part of the county health system safety net program and serves as a medical home for underserved, low-income children living in southeast Houston. Sixty-four percent of patients are covered by Medicaid, 4% are covered by CHIP (Children’s Health Insurance Program), 9% private insurance/Affordable Care Act, 9% indigent/charity care, and 5% self-pay. 5 The clinic has faculty physicians employed by a medical school, and the county health system employs registered nurses (RN), medical assistants, 1 social worker, 1 behavioral therapist, and office staff who provide and coordinate care of the patients. This clinic also serves as a learning site for pediatric residents and medical students.
The PA-PAHC clinic systematically screens for food insecurity in its patient population and would like to expand screening to other unmet SDOH. At the time of the survey, the pediatric residents were responsible for verbally screening, documenting, and providing resources on food insecurity. For prioritization of the SDOH screening, the clinic decided to seek opinions of patient caregivers, clinic staff, faculty, and pediatric continuity clinic residents. While previous tools have focused on patient perspectives on screening needs, this approach differs from ones used in the design of previous screening tools as it seeks information about the needs from the patients’ caregivers, faculty, staff, and residents who are all affected by the screening process. This study also aimed to understand if there were differences in the perceived social needs between caregivers, pediatric residents and faculty/staff in order to understand if clinicians had an understanding of the patients’ needs. A secondary aim of this study was also to elicit pediatric resident and faculty/staff perspectives on SDOH screening as they are responsible for the screening of the patients in the clinical site. The clinic staff/faculty consisted of pediatric faculty, nurses, medical assistants, social workers, behavioral therapists, and front office staff.
Methods
A cross-sectional survey was developed to elicit caregiver, pediatric resident, and staff/faculty perceptions on SDOH themes. Several tools have been utilized to screen for the social determinants of health in children. The SEEK (Safe Environment for Every Kid) is one such tool that was created to reduce the burden of child abuse by addressing the social milieu. 6 This tool was validated and studied in the 0- to 5-year age group. 6 Another SDOH screen that has been used in children is the WE CARE (Well-child care, Evaluation, Community Resources, Advocacy, Referral, Education). 7 The screen was evaluated in children 2 months to 10 years of age attending well-child visits. 8 The themes utilized were based on previous SDOH screening tools and expert information from social workers from other sites around the Pasadena and Houston area. The themes included assistance with school, childcare resources, access to health care, transportation, low-cost prescription information, legal assistance, immigration resources, housing, financial assistance, drugs, and exposure to violence. All the participants could select a maximum of 2 needs. For the pediatric residents and staff/faculty, there were additional Likert-based questions on perceptions of screening for SDOH at the visits. Institutional research board approval was obtained through Baylor College of Medicine (H-38844), Harris Health (6-07-1447), and the University of Texas School of Public Health (UTHSPH IRB Number: HSC-SPH-16-0900). The survey tools utilized are located in the Supplemental Appendices A1-A4.
Study Sample
Inclusion Criteria
Primary caregivers (≥18 years) of a child (0-17 years) who presented to the clinic for their well child/adolescent check-up were given a survey. If 2 adults were present with the child, only the self-identified primary caregiver filled out the survey. Members of the staff/faculty working at the clinic for at least 3 months and pediatric continuity clinic residents who had attended the clinic weekly for at least 6 months were eligible to participate in the study.
Data Collection Procedure
Survey completion was anonymous and implicit consent was obtained via a cover letter. The survey was available in English or Spanish for caregivers. Once the survey was complete, hard copies were placed in a locked box or cabinet. All responses were transcribed by research staff into Microsoft Excel and stored in a password-protected database. Caregiver data were analyzed and compared to the pediatric resident and staff/faculty responses.
The clinical team (pediatric continuity clinic residents, faculty, nurses, medical assistants, social workers, behavioral therapists, front office staff) were invited to participate through online software (SurveyMonkey). If they did not consent to participate, then the survey ended without asking any questions. The survey included the same preselected topics to choose from as the caregiver survey, with the exception of drugs and violence, which was added only to the caregiver survey. The clinical team survey also included Likert-type scale questions on perceptions of patient compliance and utility of screening on social determinants of health and an option for free-texting other additional needs. Data from the completed surveys were obtained from SurveyMonkey for analysis. Survey data were transcribed into an Excel file stored on a password protected database.
Data Analysis
The data analysis consisted of frequencies for categorical data analysis, with means/medians for continuous variables (Stata 13). Secondary data analysis consisted of chi-square test for categorical variables and t tests for normally distributed data. Further categorical variable analysis was by logistic regression.
Results
Demographic Survey Results
A total of 120 surveys were collected from caregivers. Ten surveys were excluded for failure to follow instructions, or with more than 2 needs being identified. A total of 110 surveys were included in the analysis. Twenty-three pediatric residents met the inclusion criteria and were approached to complete the survey. There were 20 fully completed surveys and 2 partially completed surveys over the 1-month study period (78.3% response rate). Of the 22 responses, a majority of the residents were female (72.7%). Twenty-nine staff/faculty met the study inclusion criteria, and all 29 were approached to complete the survey. There were 20 completed surveys with 1 partially completed survey (72.4% response rate). Demographic factors are included in Table 1. Some surveys lacked demographic data; however, their responses were included as part of the study.
Respondent Demographics.

PGY stands for postgraduate year after medical school graduation.
Caregivers, pediatric residents, and clinic staff/faculty could select a maximum of 2 social needs. Caregivers were most likely to report school concerns (issues with enrolling, meeting teachers, special needs, etc), health insurance (enrolling/accessing insurance for self and family), and issues with accessing high-quality childcare. Pediatric residents reported school-related needs with the highest frequency of responses (25%) followed by health insurance (18%). Housing had the least number of selections. The faculty/staff most frequently identified school needs as a concern for patients. Staff/faculty did not identify childcare as a need whereas the caregivers and residents did (Figure 1).

Social needs as selected by caregivers (n=67, 117 responses), residents (n=20, 40 responses), and faculty/staff (n=20, 39 responses) *The resident and faculty/staff survey did not have the Drugs option.
Forty percent of the completed caregiver surveys were in Spanish. Those who completed the Spanish survey had nearly 6 times greater odds than English surveyed of marking “immigration” as a need when adjusted for caregiver gender. See Table 2 for comparison by survey language completion for all the topics.
Comparison of Caregiver Identified Needs by Language Completion (Spanish vs English) Adjusted for Caregiver Gender.

Odds ratio of greater than 1 indicates that Spanish caregivers had a greater odd of reporting that SDOH (social determinant of health) need.
Unable to calculate odds ratio as there were no English-speaking caregivers who identified drugs as an issue.
When comparing responses based on role of survey participant (caregiver, resident, staff/faculty), there was no statistically significant overall difference in SDOH needs identified (P = .26). Furthermore, when using multinomial regression analysis comparing survey participant role, there were no significant differences by topic area when adjusted for survey respondent gender. See Table 3 for comparison on survey respondent type adjusted for gender.
Comparison of Identified Needs by Survey Respondent Role (Caregiver vs Resident or Faculty/Staff) Adjusted for Respondent Gender.

Odds ratio of greater than 1 indicates that resident or faculty/staff had a greater odds of reporting that SDOH (social determinant of health) need. Drugs were not included as they were not part of the resident and faculty/staff survey.
Childcare for faculty/staff was not calculated as there were no responses marked for childcare.
Pediatric Resident and Clinic Staff/Faculty Perceptions on SDOH
Residents reported perceiving social factors as affecting the patients that they care for (100% strongly agree/agree); however, they also reported the screening for SDOH to be time-consuming (85% strongly agree/agree). Staff/faculty also reported perceiving SDOH as affecting the patients that they care for (85% strongly agree/agree) (Figure 2) . However, only 35% percent of staff/faculty agreed or strongly agreed that SDOH screening is time-consuming. When comparing screening perceptions between residents and staff/faculty, there was a difference regarding the statement “Assessing social determinants of health is time-consuming” (P < .01). There was no significant difference in other responses based on clinical role.

Comparing staff/faculty (n=20) and resident (n=20) perspectives on social determinants of health.
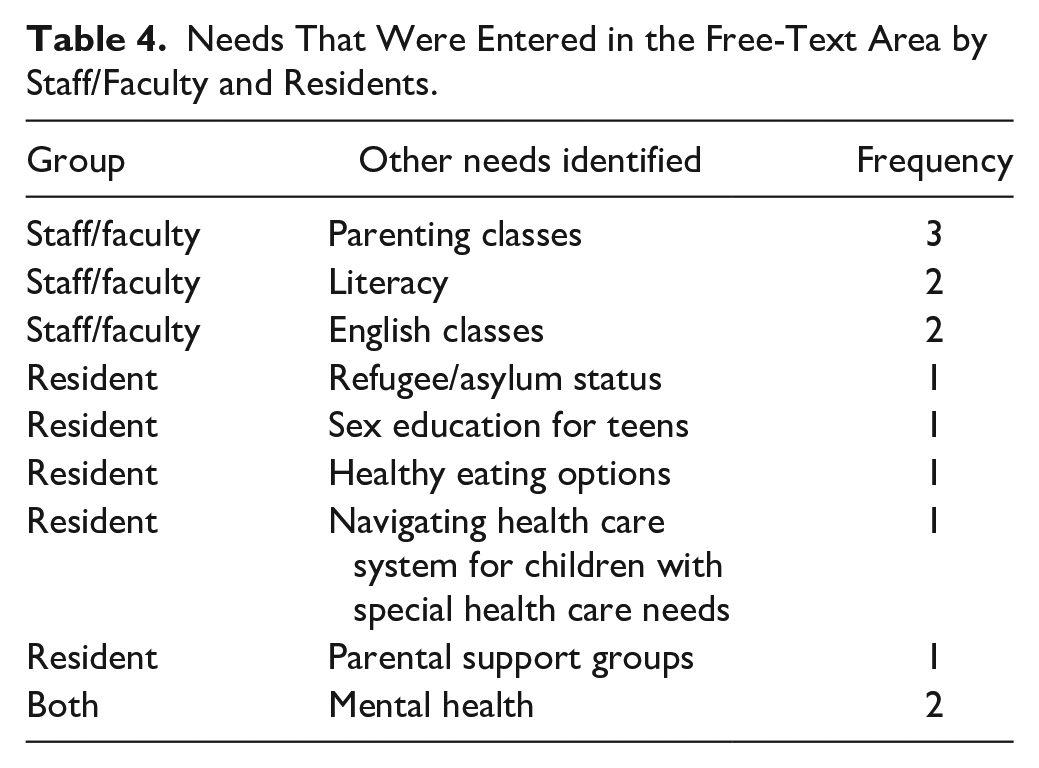
The residents and the staff/faculty were asked what other topics they identified as a need for this population. They described a diverse arena of topics, but the one topic that both groups identified was mental health (Table 4). See Table 4 for additional topics to consider.
Needs That Were Entered in the Free-Text Area by Staff/Faculty and Residents.
Discussion
This study elicited caregiver, pediatric resident, and staff/faculty views on which social needs, if addressed, could affect the care of patients in this clinic. The most frequent needs identified by caregivers were health insurance and availability of childcare. Health insurance was a frequent need identified by caregivers, residents, and staff/faculty. This may be due to the clinic serving mixed immigration status families who may not all qualify for public insurance options. Based on this information, the clinic could consider health insurance access as a topic to address for families.
While health insurance was identified frequently, immigration was a need that Spanish survey respondents had increased odds of reporting. While, this result is not surprising, the implementation of a tool with different sets of screening questions based on population such as language could be a potential solution to address the need of the Spanish-speaking population. However, not all Spanish-speaking respondents had marked immigration as a need and there is concern for implicit bias when administering different tools based on the population characteristics.
This study shows that there was no statistical difference in the perceived needs by survey respondent type. This could be reflective of the fact that within the current clinical encounter the pediatric residents, and staff/faculty are able to elicit a history and have an understanding of the community they serve. An article by Garg et al 9 discusses that the creation of validated SDOH screening tools were for research purposes and that in the clinical setting the context of the family needs to be incorporated into the tools. In some clinical settings that have close community linkages, universal SDOH screening may not be necessary and a thorough social history during the visit could suffice. However, in a busy practice, a universal SDOH tool maybe needed.
Patient desirability of resources also plays a key role in SDOH screening and resource delivery. A study looking at whether providing food assistance referrals could help identify needs, showed that 106 caregivers reported food insecurity, but of those 106 only 57 selected the option to receive a referral. 10 Furthermore, an additional 50 caregivers that did not screen positive for food insecurity had requested a food assistance referral. 10 While this study survey asked caregivers what needs they identified, the SDOH screening tool that will be implemented in the clinic needs to include patient desire for services. Eliciting caregiver perspectives on universal SDOH screening and more specifically resource delivery needs to be undertaken.
The residents overall perceived a strong connection between social determinants and child health. There was a difference in responses between residents and staff/faculty on whether or not SDOH screening is time-consuming. The residents obtain the initial history and then work together with the supervising faculty to develop a plan of care. Since the residents typically spend the most time interacting with the patients this may reflect their perception that SDOH screening is time-consuming.
Limitations
This study has important limitations. First, this was a written survey and caregiver responses may have been limited by literacy level. Second, the caregiver survey had drug use and violence as an option, but these were missing from the resident and provider survey since the caregiver survey was implemented later. Third, the response rate was not collected for the caregivers due to clinic flow issues. Fourth, social desirability bias, while minimized through an anonymous survey, potentially could have discouraged families from reporting certain needs. This could possibly explain why caregivers did not identify violence as an issue. Social desirability was a potential source of bias for the perception questions for the residents and for staff/faculty. Since residents may have received some education on SDOH during their training, this may have resulted in their choosing to agree with statements like “Social determinants of health impact the patients I care for”. Fifth, the caregivers reported their individual preferences while the residents and staff/faculty were reporting population-based data, which might explain some of the differences that were seen. Despite these limitations, this study provided the clinical team with important information on which social needs to prioritize.
Conclusion
This study expands understanding on the perceived social needs of the PA-PAHC from 3 different groups. These results suggest that health insurance access should be prioritized, as all three groups identified health insurance as a need. Next steps include devising a screening plan for assessing health insurance access for caregivers/family members and referral mechanisms. By targeting all families for screening, the hope is that those families that have mixed insurance status could have a mechanism to seek care. Potential referral processes range from having the various health insurance application forms (Medicaid/CHIP, and the county indigent charity care program) in the clinic rooms to hiring an enrollment specialist to assist caregivers with the application process. Information regarding health care access could be highlighted to illustrate the needs of this population, inform stakeholders, and lead to future community-based interventions.
These results also show that pediatric residents and staff/faculty view social determinants as affecting child health. The medical assistants/nursing staff currently perform the food insecurity screening verbally with the pediatric residents and faculty being responsible for disseminating resources. Given the shift in the role of screening, it will be interesting to elucidate staff opinion and the pediatric resident opinion on if they find screening to be time-consuming. Dissemination of these results to faculty, staff, and residents will inform decision making about how to address health care access for caregivers/family. In addition, eliciting caregiver perspectives on SDOH screening preferences and resources delivery needs to be undertaken. Further exploration should include trainees in the research, advocacy, and community partnership development process.
Supplemental Material
Swamy_SDOH_A1_20200409 – Supplemental material for Caregiver and Pediatric Health Care Provider Views on Social Needs Identification
Supplemental material, Swamy_SDOH_A1_20200409 for Caregiver and Pediatric Health Care Provider Views on Social Needs Identification by Padma Swamy, Ana C. Monterrey, Margaret S. Wood, Catherine L. Troisi and Christopher S. Greeley in Journal of Primary Care & Community Health
Supplemental Material
Swamy_SDOH_A2_20200409 – Supplemental material for Caregiver and Pediatric Health Care Provider Views on Social Needs Identification
Supplemental material, Swamy_SDOH_A2_20200409 for Caregiver and Pediatric Health Care Provider Views on Social Needs Identification by Padma Swamy, Ana C. Monterrey, Margaret S. Wood, Catherine L. Troisi and Christopher S. Greeley in Journal of Primary Care & Community Health
Supplemental Material
Swamy_SDOH_A3_20200409 – Supplemental material for Caregiver and Pediatric Health Care Provider Views on Social Needs Identification
Supplemental material, Swamy_SDOH_A3_20200409 for Caregiver and Pediatric Health Care Provider Views on Social Needs Identification by Padma Swamy, Ana C. Monterrey, Margaret S. Wood, Catherine L. Troisi and Christopher S. Greeley in Journal of Primary Care & Community Health
Supplemental Material
Swamy_SDOH_A4_20200409 – Supplemental material for Caregiver and Pediatric Health Care Provider Views on Social Needs Identification
Supplemental material, Swamy_SDOH_A4_20200409 for Caregiver and Pediatric Health Care Provider Views on Social Needs Identification by Padma Swamy, Ana C. Monterrey, Margaret S. Wood, Catherine L. Troisi and Christopher S. Greeley in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We would like to thank the leadership at the Pasadena Pediatric and Adolescent Health Center. We would like to thank Mark Meyer for providing edits to the document. We also would like to thank the research participants without whom this study would not have occurred.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.