
Abstract
Introduction
Slesinski et al, 1 Millen et al, 2 and Wu et al 3 all observed that the utilization of dietary supplements (DSs) has risen across the globe over the past 20 years, especially in the United States. Alahmad et al 4 noted that this pattern has increased awareness and discussion of these supplements among researchers, health care professionals, and regulatory organizations. Pertaining to the US Dietary Supplements Health and Education Act 1994 (DSHEA) and the World Health Organization (WHO), 5 a DS is defined as a product, excluding tobacco, meant to supplement an individual’s diet. Supplements thus include minerals, herbs, vitamins, amino acids, dietary substances, and botanical products. Order No. 11 of the Public Health and Safety of the Society in the Emirate of Dubai and its 2007 Administrative Resolution No. 30 refer to DSs as health supplements (HSs), and this terminology will be used in this article.
Alongside the increase in consumption seen in the United States, Aina and Ojedokun 6 reported that DSs such as herbal supplements are becoming increasingly popular in developing nations. DSs are closely linked to health and can include approximately 1000 distinct chemicals. These can have adverse outcomes for users as a result of damaging chemical reactions occurring within the body. However, minerals and vitamins can be purchased easily over the counter, and consumers often do not have the input of health care professionals before taking supplements. Su and Li 7 and Rossler et al 8 explain that, prior to the arrival of modern medicine, health care worldwide relied heavily on herbs, and many underserved health care populations continue to rely on herbs for medical purposes, while the Consumer Products Safety Section (CPSS) 9 finds that consumers generally take DSs for a variety of reasons, including losing weight and boosting energy. Researchers, including Moyad, 10 Izzo and Ernst, 11 Van Strater and Bogers, 12 and Tsai et al 13 have all studied the potential for DSs to interact with other drugs, with Kemper et al 14 and Piening et al 15 arguing that the potential for damaging interactions demands diligence from health care professionals and greater awareness among consumers.
According to Chitturi and Farrell, 16 DSs are a key constituent of general health care services in many developing nations and are increasingly popular in these countries. A WHO 17 estimate asserts that 8 out of 10 people living in Africa and Asia depend on traditional medicines as their primary health care resource. Similarly, in developed nations, 7 to 8 out of every 10 people use alternative or complementary forms of medicine in their primary care. Barnes et al 18 argued that the majority of DSs are safe for use provided consumers are appropriately educated on the supplements and receive accurate advice. Thus, as Neergheen-Bhujun 19 stated, health care professionals must be prepared to discuss DSs with patients and advise them on their effective and safe use.
According to Tsai et al, 13 the wide variety of potential actions of DS makes the safety and effectiveness of these products a key concern, as the use of some DS products has been observed to cause adverse side effects. To illustrate, studies by Shaw and Palmer, 20 Izzo and Ernst, 11 and Alahmad et al 4 have implicated gingko biloba in the occurrence of epileptic seizures and found that anemia can result from the chronic usage of zinc. Moreover, the DS products themselves, as Tachjian et al 21 have reported, can have negative side effects, including allergic reactions, drug interactions, toxicity (in particular contaminant and adulterant) reactions and heavy metal poisoning. Managing these outcomes can necessitate resuscitation as well as the care of symptoms and other support.
The specific reason why a DS product has had an adverse effect can be indicated by the clinical features. According to the Ministry of Health (MOH), 22 DSs with marked toxic components or pharmacological effects can, by their nature, be poisonous, and health care professionals who treat patients who consume DSs must anticipate the potential for toxicity reactions. Moreover, Tsai et al 13 have highlighted that consuming DSs alongside certain medications can result in harmful interactions, and they reported that poisoning, synergistic effects, and the inactivation of one or more of the products being taken can occur. To illustrate, St John’s wort is typically consumed to alleviate depression of a mild to moderate scale, but Van Strater and Bogers 12 find that it has the potential to induce liver enzymes and can thus interact with several targeted therapy medications metabolized through the liver, including antidepressants. In addition, Moyad 10 has reported that taking gingko biloba, ginger, garlic, and other substances in conjunction with anticoagulants introduces a bleeding risk.
The state between good health and illness is titled suboptimal health status (SHS), and this state is considered a reversible, subclinical phase of chronic illness. Any integrated preventative treatment plan must aim to achieve a customized, predictive and preventative medical regimen for a patient. Similarly, SHS involves the evaluation of a patient’s health and the provision of effective steps to improve health, prevent disease, and address the early stages of illness. SHS is a concept that is now emerging in a range of countries such as Australia (Davy and Patrickson 23 ), Canada, 24 and Japan. 25 Creating a DS health regimen that satisfies the needs and concerns of DS consumers specifically requires that knowledge about the health of these consumers be obtained and analyzed. Furthermore, counseling and other interventions targeted at enhancing consumers’ health will be required.
Presently, only a small amount of data are available on DSs and their associated effects on health. Dubai currently does not have a DS surveillance program. Elsewhere, the detection of safety concerns related to DS use are centered on the spontaneous reporting of problems or vigilance systems. Gavaza et al 26 and Piening et al 15 have explain that, when suspected adverse effects related to DSs are not reported within a relevant system by health care professionals or patients themselves, the recognition of threats to consumer safety can be delayed or missed entirely. Unsurprisingly, this can have a severe influence on public health. Consequently, the extent of the issue and its underlying causes must be identified, and public health policies must be adapted based on these findings. This study will examine the link between SHS and the consumption of DSs.
Methodology
Setting and Design
This is a survey-based cross-sectional research study conducted in 2 major Public Service Centers in the Emirate of Dubai, where the customer service employees invited the participants to complete the questionnaire. These 2 public service centers are considered major centers in Dubai that people regularly seek clearance and completion of their services. The questionnaires were administered to the participants during their visit to the service centers. The nature and main objectives of the study were clearly explained to every participant, and those willing to participate in the study were asked to clearly sign the provided consent form immediately before completing the study questionnaire. The study was conducted from June 2017 to October 2018.
Study Population (Inclusion and Exclusion Criteria)
The target population to be studied contained both nationals and nonnational residents in Dubai, UAE. All residents aged 18 years and older who had the will to participate were directly included in this study. Participants aged less than 18 years and those who did not want to participate were excluded. Participation was voluntary, and no incentives were offered to any participant who completed the survey form. Participants who had allergies and/or chronic disease and/or had taken prescription drugs during the last week were excluded from the study.
Sample Size
Because the prevalence of DS product consumption may range from 10% to 30% according to Kemper et al 14 and approximately 19% according to Hara et al, 27 we expected the current prevalence rate to reach almost 30% in this study. We set the alpha level to 5% in order to generate 95% confidence intervals. In addition, the precision (D) of the mentioned 95% confidence intervals was set to 5% in order to maximize the spectrum of the 95% at 10%. Pertaining to the aforementioned assumptions, the minimum acceptable sample size needed was n = 539 candidates if we assumed a nonresponse rate of approximately 40%. The final sample size was 618 participants.
Research Instrument Development
The validated questionnaire was tailored to the UAE population,28,29 and a well-structured, self-administered questionnaire was created and enhanced to highlight all the basic key points of the study in ways that were suitable to the local population of the UAE. The questionnaire was then examined by subject experts for content, layout, and relevance. The questionnaire was subsequently validated by 2 lecturers from the disciplines of medicine and clinical pharmacy at Ajman University; it was tested for content relevance and appropriateness, and small modifications were carried out according to their final comments. In addition, the questionnaire was piloted by 20 of the participants immediately before commencing the general distribution, and essential modifications were performed accordingly. Data that were collected from the pilot examination were not included in the final analysis of the data. The analysis of reliability of our instrument was carried out by calculating Cronbach’s α value. Cronbach’s α value of the questionnaire was .76, indicating acceptable internal validity.
Research Questionnaire Sections
The questionnaire was available in English or Arabic, depending on the respondent’s choice, and the questionnaire consisted of 4 main sections. The first section covered demographic information, such as age, sex, marital status, nationality, employment status, educational level, and monthly income. The second section evaluated the health and lifestyle characteristics, such as allergies (yes/no), chronic medical conditions (yes/no), prescription drug use in the past week (yes/no), smoking status (yes/no), and physical activity (yes/no). The third section assessed the consumption of different groups and categories of DSs. The fourth section assessed the SHS and included 25 questions in which the candidates were asked to explore how often they experienced any of different complaints listed in the prior month; the 25 questions were answered on a 5-point Likert-type scale (1 = never or almost never, 2 = occasionally, 3 = often, 4 = very often, 5 = always).
Ethical Considerations
The study was approved by the Institutional Ethical Review Committee of Ajman University, and an official approval letter was released to facilitate the distribution and collection of the questionnaire. Enrollment in this study was completely voluntary and without any compensation. Prior to collection of the data, the exact objective of the questionnaire was discussed, and the participants were also informed that completion and submission of the questionnaire required their official consent; as such, all participants signed the given informed consent form. Moreover, anonymity of all participants was preserved in the study, as the data were deidentified.
Data Analysis
The collected data were analyzed using SPSS version 23. We summarized the qualitative variables using frequencies (percentages) as needed. Quantitative variables were analyzed using the mean ± standard deviation (±SD). A suboptimal health status score was created to examine the health status of the study subjects. A SHS score was defined as the proportion of questions for which the answers were “occasionally,” “often,” “very often,” and “always.” The SHS score ranges from 0% to 100% and may be utilized as a good representative of the total SHS. We used a simple binary logistic regression to test the possible association between DS product consumption and SHS. A P value <.05 was selected as the criteria on which to build decisions regarding statistical significance.
Results
Demographic and Socioeconomic Characteristics
A total of 618 participants were enrolled in the study and answered the full questionnaire. Among these, 51.8% (n = 320) were female and 48.2% (n = 298) were male. Of the total, 14.1% (n = 87) were aged 18 to 24 years, 36.4% (n = 225) were aged 25 to 34 years, 28.3% (n = 175) were aged 35 to 44 years, and 21.2% (n = 131) were aged >44 years. More than half of the participants were married; 67.8% (n = 419) were married and 32.2% (n = 199) were single. The vast majority were employed (84.1%; n = 520). Regarding education, 18.8% (n = 116) had a high school education, 61.2% (n = 378) had a bachelor’s degree, and 20.1% (n = 124) had a postgraduate education. The monthly income was ≤5000 AED for 18.1% (n = 112), 5000 to 9999 AED for 23.5% (n = 145), 10 000 to 14 999 AED for 25.9% (n = 160), and ≥15 000 AED for 32.5% (n = 201).
Among the participants, 393 participants (63.6%) were nonsmokers, and 225 participants smoked (36.4%). Of the total participants, 110 (17.8%) had allergies, 85 (13.8%) had diseases and 144 (23.3%) had taken prescription drugs in the past week. The majority of the study participants (71.8%) reported weekly physical activity. For more details, see Table 1.
Number and Percentage Summaries of the Demographic, Health, and Lifestyle Characteristics.

Prevalence and Use of Dietary Supplements
In this study, 317 participants (51.3%; 95% CI: 47.3%-55.3%) reported the use of DSs. The categories of DSs used by the participants are shown in Table 2. Among the 317 participants who ever used DSs, vitamins (89.9%) and minerals (58.7%) followed by dietary fibers (30.6%) and herbal/botanical supplements (30%) were the most commonly used among all categories of DS products. For more details on the other categories, see Table 2.
Number and Percentage Summaries of the Dietary Supplement (DS) Product Categories (n = 317).

The Influence of DS Consumption on Suboptimal Health Status
Of the total, 236 participants (38.2%) had allergies or/and chronic disease or/and had taken prescription drugs within the past week. To control for the effect of these confounding variables on suboptimal health status, we excluded those participants, and those remaining (n = 382, 61.8%) were considered valid for subsequent analyses.
There was a significant association between DS consumption and suboptimal health status (P < .001). DS consumers were more likely to score higher in suboptimal health status compared with non-DS consumers. The average suboptimal health status score was 64.6% (95% CI: 60.6%-68.6%) for DS consumers compared with 54.4% (95% CI: 50.8%-58%) for non-DS consumers. Moreover, DS consumers had a 1.5-fold increased odds of suboptimal health status when compared with non-DS consumers (95% CI: 1.4-1.7).
The results of each of the questions related to suboptimal health status for DS consumers and non-DS consumers are shown in Tables 3 and 4.
Number and Percentage Summaries of Suboptimal Health Status for All Consumers and Nonconsumers Without Allergies, Chronic Diseases, or Medications (n = 382).

Mean Score for the Questions on Suboptimal Health Status for All Consumers and Nonconsumers Without Allergies, Chronic Diseases, or Medications (n = 382).
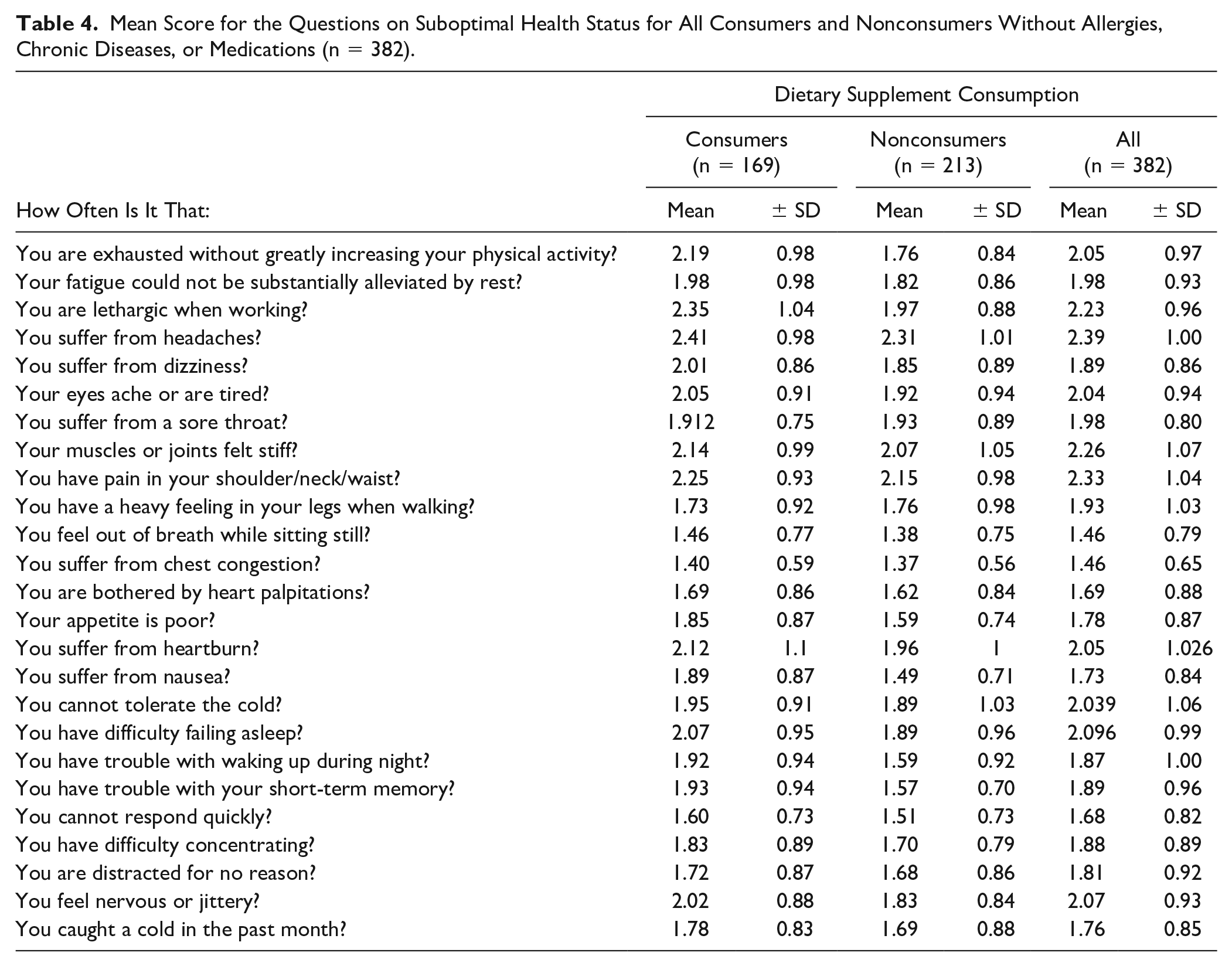
Table 5 displays the results of the binary logistic regression model to determine the effect of DS consumption on the suboptimal health status of the participants. All variables suspected to be associated with suboptimal health status were included and adjusted for DS consumption. The crude and adjusted odds ratios in this table show the magnitude of the association, and their corresponding P values indicate whether the association was statistically significant by using the cutoff value of .05. The results of this analysis showed that the consumption of DSs has a statistically significant statistical, even after the adjustment of all confounding factors.
Logistic Regression Analysis of Suboptimal Health Status (Dependent Variable) and Dietary Supplement (DS) Consumption (Independent Variable).

Crude (not adjusted).
Adjusted for allergy.
Adjusted for chronic disease.
Adjusted for prescription medication.
Adjusted for smoking.
Adjusted for physical activity.
Adjusted for age.
Adjusted for sex.
Adjusted for allergy, chronic disease, prescription medication, smoking, physical activity, age, and sex.
Discussion
The use of DSs is on the rise globally and presents a significant concern for public health authorities. Many people regard DSs as a safer and more efficacious alternative to standard prescription medicines. DSs are widely available, do not require a prescription and are heavily marketed, meaning many people choose them for numerous illnesses. This research has examined the consumption of DSs and their association with poor health. As far as we can ascertain, no research similar to this has been previously undertaken in the UAE.
The findings of this research study have demonstrated that using DSs is widespread in the UAE, with 51.3% (95% CI: 47.3%-54.3%) of respondents stating that they had at some point used a DS. This is similar to the findings from the United States (52%), 30 the findings from Australia (56%) 31 and the findings of the Health and Nutrition Examination Survey (53%).32-34 The results also indicated that, compared with other nationalities such as Iranians (36.3%), 35 Irish (23%), 36 Croatians (30.5%), 37 Jordanians (27.4%), 38 and Portuguese (16%) (Marques-Vidal), 39 UAE citizens utilized DSs at a greater rate; however, the UAE participants did not use DSs as much as those in Columbia (73%) 40 or Serbia (68.1%). 41 The fact that this research does not match previous findings may be attributable to lifestyle elements and socioeconomic variations among the respondents.
The findings of this research have also demonstrated that the types of supplements most commonly employed by the subjects were vitamin and mineral supplements. This is in line with the findings of many other studies that have demonstrated that multivitamins and minerals are widely used.32-34,37,40,42-48
Research in 2012 assessed the use of supplements containing ephedra, which has been suggested to have a correlation with certain conditions and unexpected death. Among the 48 deaths that had a temporal relationship with using supplements, 18 subjects died from atherosclerotic coronary disease (37.5%), 16 subjects died from sudden unexplained death (33.3%), and 6 subjects died from hypertrophic cardiomyopathy (12.5%). This research came to the conclusion that idiopathic sudden death and atherosclerotic coronary disease were more common among those taking supplements. 49
As this research is epidemiological, it is hard to ascertain the relationship between the use of DSs and their impacts on managing disease and malnutrition because supplements cannot be separated from other efforts to improve health. In the work we have reported, we have examined the relationship between using DSs and SHS. Our results demonstrated that SHS was considerably more prevalent for subjects who had sometimes used DSs in comparison to those who had never used them (P < .001).
DSs are becoming more popular globally, and the expansion of the market for such products in Dubai mirrors this. Consuming any pharmacologically active substances could have a potential negative impact on health. Additional hazards regarding the consumption of DSs are the possibility of DS interactions with medicinal drugs or other supplements, contamination, or adulteration. Investigation into the potentially negative influence of health supplements on public health is required.
There were a number of limitations to this research. First, as with all cross-sectional designs, cause and effect cannot be inferred, and the direction of the correlations between the independent and dependent variables cannot be inferred. Although there is reasonable confidence that the results can be generalized, the results may have been influenced by selection and response bias. This possible bias has not been further investigated by comparing the nonresponders with the responders. As the research was undertaken in Dubai, it cannot be directly generalized to other states in the UAE.
Conclusions
This research has offered significant new information regarding the use of DSs and their associations with SHS in Dubai and the UAE, filling a gap in the available knowledge. The results of this research may be employed for the development of health policies and programs regarding dietary supplements in Dubai that will assist in minimizing the risks and possible adverse effects of using such supplements. This research also demonstrated that an educational program for the population of Dubai with information regarding the health risks of using supplements would be ideal. The resulting program could make the population more aware; it could help the healthcare professionals in Dubai to develop policies regarding the use of health supplements; and deal with the negative health outcomes from DS use.
Footnotes
Acknowledgements
We would like to thank our colleagues for their participation in this study and their support of our work in this way; they helped us obtain results of better quality.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.