
Abstract
Introduction
Musculoskeletal (MSK) conditions account for the third largest area of NHS program spending (£4.7 billion in 2013-2014).1,2 Following Lord Carter’s review for the Department of Health in 2016, 3 there has been an increased focus on high-cost procedures and interventions, and on defining, mapping, and collecting cost data. This focus includes areas such as elective surgical procedures and MSK trauma admissions.3,4 However, there has been significantly less attention given to defining costs and collecting widespread comparable MSK cost data in primary and community settings.
Unwarranted variation within the NHS acute sector has been estimated at a value of £5bn in terms of an efficiency opportunity. 3 This was estimated by reviewing all key resource areas such as clinical staff, pharmacy and medicines, diagnostics and imaging, procurement, back office functions and estates and facilities. 3 Identifying variation requires the use of these specific metrics as outlined in Lord Carter’s report and there has been a large focus on costing and efficiency in acute care, leading to clear examples of unwarranted variation being identified within acute services. Hip prostheses, for example, have been shown to vary in cost from £788 to £1590 across NHS Trusts, with those buying the most not paying the least. 3 This work is developing within the Model Hospital, 4 a digital information service set up to support secondary care providers to improve productivity and efficiency. The Model Hospital demonstrates how appropriately applied metrics can allow for a useful comparison of services and their efficiency. However, similar economic metrics have not yet been formalized or evaluated for MSK primary and community care in the United Kingdom.
Economic evaluation is “the comparative analysis of alternative courses of action in terms of both their costs and consequences.” 5 The objectives of health economic analyses are to identify, measure, value, and compare costs and consequences of alternative treatments/pathways of care. 5 Economic evaluation techniques therefore provide the framework for capturing costs and outcomes/benefits of different health interventions. 6 In this review economic costing methodology will be explored, with the aim of identifying the most important cost variables for making resource use comparisons within primary and community MSK settings. The quality of costing methods will also be evaluated to determine the strength of these findings.
Graves et al 7 described 12 criteria for specifically assessing the quality of costing methods of economic analyses. These criteria include, for example, stating and justifying the perspective, distinguishing between short and long run costs, and reporting methods for estimating quantities of resources. Graves et al 7 reviewed 45 economic analyses against the 12 criteria in 2002, and concluded that more attention should be given to costing methods to ensure the accuracy of costing estimates.
Mogyorosy and Smith 8 also reviewed methodological issues with costing health care services across Europe in 2005 and highlighted the usefulness of defining cost drivers. Cost drivers are variables such as medical visits that affect costs over a given period of time and can be directly linked to changes in costs. 9 It is important to identify the most relevant cost drivers for a specific setting as these can help explain changes or differences in overall costs of care. It is also sometimes sufficient and necessary to limit data collection (or costing) to the key cost drivers. 10 Activity-based costing looks to improve the accuracy of cost estimation by using multiple cost drivers. 8
Costing within economic analyses will differ dependent on the perspective, which can include a health perspective looking at direct costs to health managers, or a societal perspective looking at direct and indirect costs, including productivity losses. 11 In this review, only direct health care costs will be examined in detail as the review looks to identify key drivers of MSK health care costs only.
This review aims therefore to evaluate the quality of costing methods used within MSK economic analyses and also to identify the most important cost drivers (provider variables) that could be reported by individual primary care and community MSK services and used to develop a system level methodology to broadly cost and compare these services. The perspective will be that of a health service perspective looking at costs incurred by MSK patients being predominantly treated in community/primary care, as this is the area at present where a clear methodology is lacking.
Method
This review followed protocol guidance set out within the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement 12 (see Supplement 1 for PRISMA Checklist).
Eligibility Criteria
Inclusion criteria were the following: all types of economic analyses, economic analysis needed to be the primary focus of the study and clearly stated from the outset, studies published within the past 10 years (January 2008 to May 2018) in order to ensure applicability of costing approaches, English language papers only (due to resource limitations of the review), studies primarily set within community or primary care health settings to support the focus of the paper, patient population to include patients undergoing treatment for most prevalent MSK disorders (back, neck, shoulder, knee or all MSK conditions,13,14 studies needed to report disaggregated health care costs, and papers needed to be published in full within a peer-reviewed journal.
Searches
Medline, AMED, EMBASE, CINAHL, HMIC, BNI, and HBE electronic databases were searched. Searches were limited to papers within the past 10 years only to ensure applicability when looking to review costing methods. Search terms were grouped into core areas of type of economic evaluation such as cost benefit or cost utility, 6 study type such as analysis or evaluation, and prevalent MSK condition such as back, neck, knee, or shoulder.13,14 Searches were combined using Boolean logic (AND and OR). Additional gray literature was identified using reference lists of included articles. Included studies were required to have a combination of key search terms (Table 1) within the study title, to ensure studies were focused on economic evaluation, and not on intervention effectiveness.
Search Terms.

The review did not set out to identify every economic analysis within the field of MSK, but to systematically identify economic analyses within the field of MSK from community/primary care settings that met the inclusion criteria, using a structured, transparent, and reproducible search methodology. The full electronic search strategy for searching the database Medline can be viewed within Supplement 2.
Selection Criteria
One reviewer (RB) reviewed search results and identified those based on title and abstract unquestionably excluded from the review, and those appropriate for full review. The same reviewer (RB) and a second reviewer (JH) then independently read full papers for identified studies and determined eligibility based on inclusion/exclusion criteria to ensure all criteria were met for inclusion into the systematic review.
Data Extraction
Data were extracted using an extraction sheet made up of study descriptors such as author, year, title, objectives, setting, population, study size, perspective, outcomes, cost variables, cost year, costing sources, and analysis type, for example, cost-effectiveness analysis (CEA), cost utility analysis (CUA), cost benefit analysis (CBA), cost consequence analysis (CCA). This was followed by the 12 quality criteria described by Graves et al. 7 Two reviewers independently extracted data (RB and JH), one reviewer had a clinical MSK background (RB) and one was a health economist (JH). All health care costs were extracted and included whether the cost was for treatment within primary, community or secondary care as although the studies were predominantly set within primary care/community clinics, costs were still borne by the health care system across all settings (eg, if a patient was sent for an investigation or consultant opinion).
The focus of the study was restricted to costs and therefore outcomes and specific interventions were not reviewed. Detailed costs were reported and analyzed for the usual care/control groups only in order to allow for broad comparisons of key cost drivers to be made across studies. Due to the broad focus of the review (including all common MSK conditions) cost drivers were ranked for each study rather than being directly compared.
Quality of Costing Methodology
Quality of costing methods within included studies was evaluated using 12 criteria described by Graves et al 7 and following this guidance organized into 4 predefined categories; general costing issues (criteria 1-4), methods used to determine the quantities of resources (criteria 5-7), methods used to determine the value of resources consumed (criteria 8 and 9), and reporting of data (criteria 10-12). 7 Quality of costing methodology within studies was evaluated independently by 2 reviewers (RB and JH) and inputted directly into the extraction sheet. A third reviewer was then available (ML) if agreement could not be reached.
Results
Search Results
A total of 751 records were identified through electronic searching of relevant databases. This gave 344 records after electronic duplicates were removed (see Figure 1 for detail).

Flowchart of search results.
Following initial review of titles and abstracts 276 articles were excluded for failing to meet the eligibility criteria. Following full review of the remaining 68 articles against eligibility criteria by the 2 reviewers, 22 studies were suitable for inclusion in the review. The main reasons for exclusion were the following: not providing disaggregated costs to determine patient-level health care costs, not being undertaken from the right clinical setting, being a secondary analysis rather than a preplanned economic analysis, being an abstract only, or being a model or review rather than a primary study.
The majority of studies were economic analyses conducted alongside randomized controlled trials (n = 21) or other trial-based analyses (n = 1). 15 See Table 2 for characteristics of included studies.
Characteristics of Included Studies.

Abbreviations: C, community; RCT, randomized controlled trial; CEA, cost-effectiveness analysis; CBA, cost benefit analysis; CUA, cost utility analysis; CCS, const consequence analysis; BMI, body mass index; LBP, low back pain; MSK, musculoskeletal; OA, osteoarthritis; PC, primary care; SC, secondary care.
Quality of Costing Methodology in Included Studies
The results of quality assessment of costing methodology are summarized in Table 3, following criteria set out by Graves et al. 7
Quality of Costing Methodology in Included Studies (Criteria Defined by Graves et al 7 ).

Costing Criteria
Category 1: General Costing Issues (Questions 1-4)
The majority of studies stated the economic perspective (Q1) (21 out of 22) with a mixture of health care perspective (n = 4), societal perspective with disaggregated costs (n = 9), both health care and societal perspective stated (n = 8), and one with no perspective stated but with disaggregated health care costs. The majority of studies did not fully justify their perspective (Q2) but simply stated it within their introduction or methods (7/22 fully justified stated perspective, and 7/22 partially justified). Studies scored as “partial” for Q2 did not give an explicit statement but gave some form of justification within the introduction/methods for their approach such as discussing at length the societal burden of the MSK condition then adopting a societal perspective. All studies apart from one study 16 (and the study without a stated perspective 17 ) gave cost data that satisfied the stated perspective (Q3).
Category 2: Methods Used to Determine the Quantity of Resources Used (Questions 5-7)
As within the review by Graves et al, 7 studies rarely made a distinction between short- and long-run costs (Q4) (only 1/22 studies 18 ). Methods for quantities of resources used by patients (Q5) were largely based on patient self-report cost diaries either collected through a questionnaire or through interview that detailed resource utilization such as clinical visits to GP (general practitioner), practice nurse, physiotherapist, hospital outpatient appointment, day case and other hospital admissions, A&E (accidents and emergencies), and prescriptions, 19 (21/22 studies used some form of self-report questionnaire). Other methods included using clinician inputted data 18 and extracting data from medical databases.16,20 The study by Pinto et al 21 used the Osteoarthritis Cost and Consequences Questionnaire (OCC-Q) to collect cost data from patients, and then cross-checked this information against national GP and health information databases. All studies met this criterion.
The majority of studies (20/22) described their methods for allocating time for human resources (Q6). Included studies mainly used the national average times for each type of health care consultation to estimate costs, other studies split time for group sessions between participants,22,23 and some were unclear. 20 Methods for allocating prices between patients (Q7) were also often only clear within intervention group sessions where the cost was split between patients, 23 or through splitting the cost of intervention training, 24 although some studies detailed splitting the cost for shared capital costs such as staff travel and space provided by the NHS. 22
Category 3: Methods Used to Determine the Value of Resources Consumed (Questions 8 and 9)
The majority of studies (19/22) gave methods for the estimation of prices, unit costs, or charges (Q8), with most studies counting all resource inputs for each patient such as visits to the GP or physiotherapist, and multiplying each by the unit cost to provide the direct cost for each group of patients and then calculating the mean resource cost per patient. Published estimates of unit costs were used by the majority of studies, including, for example, UK NHS Reference Costs and Unit Costs of Health and Social Care publications by Curtis and Burns 25 for secondary care and primary care costs respectively,15,18,19,26-28 the Danish National Health Insurance Service Register (primary care), Danish National Patient Register (secondary care) and Danish National Prescription Registry (medication), 16 the Dutch Guidelines or Dutch Central Organisation for Healthcare Charges (primary and secondary care costs) or the Royal Dutch Society of Pharmacy (medication),29,30 or private practice charges.21,31 Lamb et al 22 stated that intervention costs were estimated using in-trial analysis but did not give reference to the full costing methods. All studies used more than just hospital charges to calculate costs (Q9), including, for example, medication costs in addition to hospital charges20,31 or using a variety of costing resources.
Category 4: Reporting of Data (Questions 10-12)
The majority of studies reported the year cost data were collected (Q10), with only 3 studies omitting this level of detail.19,30,32 The base cost year was also reported for most studies (Q11) with this information not present in only 1 study. 32 Adjustments for costs made in different time periods (Q12) were frequently not necessary due to the majority of studies being run over a 12 month period and therefore not needing to discount for different time periods, with the exception of Barton et al 33 who discounted at a rate of 3.5%. The majority of other studies stated adjusting prices for inflation to match base cost year.15,16,18,21,22,34
Cost Drivers
Detail of cost drivers extracted across studies included; highest resource unit cost, highest resource utilization, and highest mean resource cost per patient, where available. There was minimal detail however within some studies; for example, Barton et al 33 had a key cost driver of “visit costs” but this was not broken down between different types of clinicians. In contrast, detailed visit costs were broken down and provided in the study by Hollinghurst et al, 18 providing detail of; hospital care/A&E visit costs, GP home visit costs, GP surgery visit costs, GP out-of-hours costs, GP telephone consultation costs, district nurse home visit costs, practice nurse consultation costs, practice nurse telephone consultation costs, and health care assistant/phlebotomist costs.
Unit Costs
The highest unit costs were consistently found to be outpatient visits/medical specialist visits, hospital admissions (day case and hospital stay), and imaging (magnetic resonance imaging [MRI], computed tomography [CT]). This demonstrates that the secondary care costs make up the highest unit costs within MSK health care (see Table 4 for further detail and drivers).
Highest Unit Costs. a


 Top 2 (first/second) unit costs within studies
Top 2 (first/second) unit costs within studies
 Next 2 (third/fourth) top unit costs within studies
Next 2 (third/fourth) top unit costs within studies
Abbreviations: GP, general practitioner; MRI, magnetic resonance imaging; CT, computed tomography; PT, physical therapist; MT, manual therapist.
Cost drivers only included within this table if they were within the top 4 unit costs within at least 2 studies. Costs are in different currencies and so cost years are not directly comparable. Mean costs per patient reported for control/usual care/reference group.
Resource Utilization
The highest resource utilization across studies was found to be; primary care visits to the GP, outpatient/medical specialist visits, and physiotherapy visits (see Table 5 for further detail and drivers).
Highest Utilization. a
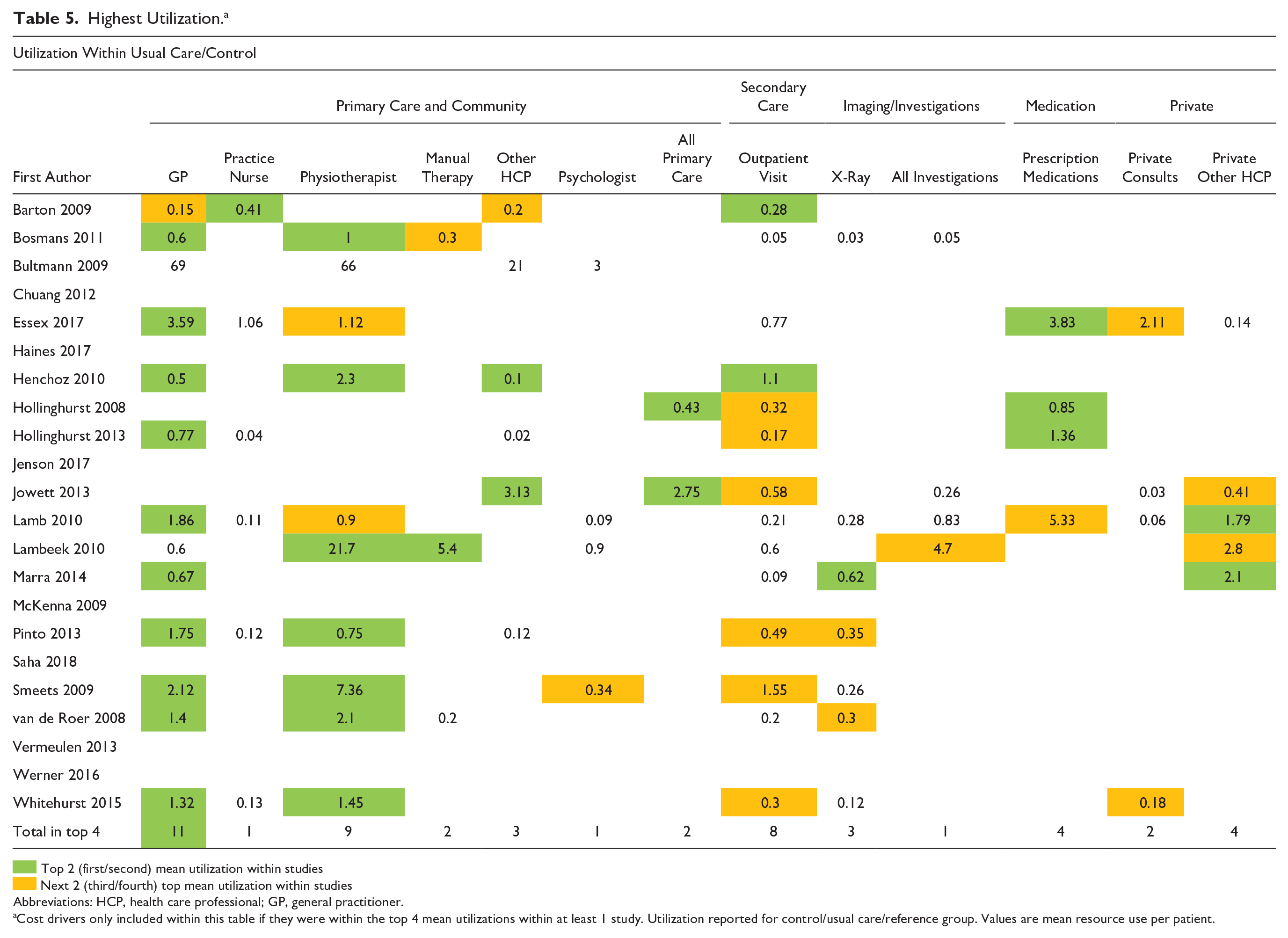

Top 2 (first/second) mean utilization within studies
Next 2 (third/fourth) top mean utilization within studies
Abbreviations: HCP, health care professional; GP, general practitioner.
Cost drivers only included within this table if they were within the top 4 mean utilizations within at least 1 study. Utilization reported for control/usual care/reference group. Values are mean resource use per patient.
Mean Resource Use Cost per Patient
Thirteen studies gave data on the mean resource use cost per patient allowing for analysis of key drivers of costs within studies. Analysis of these studies shows that important drivers of MSK health care costs (starting with highest costs) were the following: primary care visits to the GP, outpatient/medical specialist visits, and physiotherapy visits. This demonstrates that predominantly high levels of utilization of key resources were driving cost, with the top 3 drivers exactly matching those for highest utilization (see Table 6a; this table is available with costs converted/inflated to GDP 2018 within Supplement 3 as Table 6b). Converted costs, however, need to be viewed with caution due to the significant heterogeneity between studies including heterogeneity in MSK conditions treated, health systems, time horizons, and costing methods. Costs therefore cannot be directly compared and have instead been ranked within individual studies in order to identify the highest cost drivers.
Highest Mean Costs per Patient. a


Top 2 (first/second) mean costs within studies
Next 2 (third/fourth) top mean costs within studies
Abbreviations: GP, general practitioner; ET, exercise therapy; HCP, health care professional; MRI, magnetic resonance imaging.
Cost drivers only included within this table if they were within the top 4 mean costs within at least 1 study. Mean costs reported for usual care/control/reference group.
Discussion
This review captured MSK economic analyses across a number of varied health systems/nations, including the United Kingdom, the Netherlands, Denmark, Norway, Switzerland, Sweden, Italy, the United States, Canada, Australia, and New Zealand, and focused on trials providing treatment primarily within primary and community health care settings.
Quality of Costing Methods
Only one study 18 satisfied all of the costing criteria reported by Graves et al. 7 The lowest conforming study satisfied 7 of the 12 costing criteria (58%), 17 which could imply errors in costing methods. 7 In all, 14/22 (64%) of studies, however, satisfied at least 10 or more criteria.
In the review by Graves et al 7 in 2002, only 2 out of the 12 costing quality questions (Q5 and Q8) were satisfied by more than 67% of included articles. In this review 10 of the 12 questions (all except Q2 and Q4) were satisfied by more than 77% of included articles.
The quality assessment of costing methods within this review demonstrates that more attention still needs to be given to the costing methods used to estimate individual patient costs with particular attention needed to clarify short- and long run-costs and to fully justify the chosen perspective. There appears, however, to have been a significant improvement with costing within economic analyses when these results are compared with the previous similar review of 45 economic analyses by Graves et al 7 in 2002.
Key Cost Drivers
The highest resource unit costs were secondary care–based costs, in contrast to the highest resource utilization, which included primary, community, and secondary health care drivers, such as GP visits, physiotherapy visits, outpatient/medical specialist visits, and prescriptions. When these were evaluated together to give the mean resource use cost per patient, the same cost drivers for utilization were driving mean resource use costs per patient, showing that the high level of utilization rather than the initial unit cost seems to be the predominant factor in driving mean costs within MSK health care in this setting (see Tables 4-6). These findings therefore support a shift in focus for those commissioning and evaluating MSK services, from high-cost procedures (such as surgical interventions and inpatient stays) within MSK health care (largely at a secondary care level) to high utilization of key resources such as GP visits and physiotherapy visits within primary care and community settings, with further scrutiny of the cost-effectiveness of the entire pathway of MSK health care provision.
We summarized the key drivers of MSK health care costs within an international context, and found that the highest mean costs across studies (in order) were for: GP visits, physiotherapy visits, outpatient medical specialist visits, prescription medication, and Hospital Admissions (day case and elective stay grouped together). These 5 drivers captured over 70% of the costs in the majority of studies with fully disaggregated costs (7/11 studies). Recommendations from the review would be to collect detailed costs for the above key drivers particularly with regard to GP, physiotherapy, and outpatient visits, which formed over 50% of the costs across the majority of studies (8/11 of those with fully disaggregated costs; these 3 drivers alone captured over 75% of costs in 2 recent studies.16,35 This detail might include capturing standard treatment times within clinics (such as 30- or 45-minute physiotherapy consultations) and grade of treating clinician (basic grade or advanced level) in order to further improve the accuracy of costing for the most important cost drivers. Hollingsworth et al 18 was the only study to detail the treating clinician grade to further improve the accuracy of their costing calculation and overall provides a useful exemplar of high-quality costing methods within community MSK health care. Grieve et al 36 supports this individualized approach, highlighting that cost-effectiveness analyses using average unit costs can report inaccurate incremental costs. Clearly, some studies were restricted by the research costs and practicalities of collecting this level of data, however, capturing this detail would improve the accuracy of costing information in this setting as these are key cost drivers that are not standardized across MSK services, as was too often assumed. This is particularly relevant as significant system changes are made within MSK health care such as the introduction of first contact practitioners (FCP) in the United Kingdom, where GPs are being replaced in certain areas by advanced MSK physiotherapists to assess and manage MSK patients in primary care. 37 Using a standardized mean unit cost for the physiotherapist contact in these instances would not take into account the seniority of clinicians used or the differing consultation times allocated, and could therefore lead to inaccurate evaluations of cost.
Additional costs that are useful to collect dependent on the perspective of the economic review are; private health care professional costs (such as private physiotherapy, acupuncture, osteopathy), equipment (including patient aids, orthotics, etc) and imaging costs (MRI/X-ray were the most important of these).
Limitations of the Review
Limitations of this review were that not all MSK economic analyses were included within the review, which means that our results cannot be generalized to all MSK economic analyses. Non-English studies were also not included due to the resource limits of this review. Only direct health care costs were reviewed, future studies incorporating additional societal costs would be useful to further inform population level health systems. This study was a broad review of MSK economic analyses and due to this breadth, there was a large amount of heterogeneity between studies. This means that caution needs to be applied when looking to make direct comparisons between studies. Future research in this area focusing on one health system or one condition would allow for a more detailed and in-depth analysis of direct costs. Further review of other sources of activity/spend data alongside prospective studies evaluating the cost drivers identified within this review in primary/community MSK services would also be useful to further explore and validate findings.
Conclusion
This review provides a detailed overview of the quality of costing methods used within MSK economic analyses and has identified key drivers of MSK health care costs for patients accessing treatment in community and primary care settings. The quality and accuracy of costing data in this setting need more attention around capturing the grade of treating clinicians and specific consultation length for clinical visits to more accurately determine true patient-level costs as these factors were key cost drivers. If this information was collected in a standardized, accurate, and consistent manner, it could form a useful part of a standardized MSK data set (alongside key metrics measuring treatment outcome/performance) and help develop future benchmarking capabilities within these settings supporting national data evaluations and informing health care policy (such as NHS RightCare in the UK setting). 38 Such an approach would also support a future direction toward value-based care (health outcomes achieved per monetary unit spent) which looks to achieve good outcomes in the most efficient way, 39 helping form a system level framework for restructuring health care delivery for the future.
Supplemental Material
Submission_Supplementary_Material_Economic_Review_Editable – Supplemental material for Costing Methodology and Key Drivers of Health Care Costs Within Economic Analyses in Musculoskeletal Community and Primary Care Services: A Systematic Review of the Literature
Supplemental material, Submission_Supplementary_Material_Economic_Review_Editable for Costing Methodology and Key Drivers of Health Care Costs Within Economic Analyses in Musculoskeletal Community and Primary Care Services: A Systematic Review of the Literature by Roanna Burgess, James Hall, Annette Bishop, Martyn Lewis and Jonathan Hill in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: RB is supported by SWBH Your Trust Charity.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.