
Abstract
Introduction
Clinical evaluation of suspected obstructive sleep apnea (OSA) is reliant on subjective reports of excessive daytime sleepiness, snoring, or witnessed apnea. 1 These require patient recognition or bed partner recall, either of which may be inaccurate or unavailable. Although clinical guidelines suggest utilizing reports of excessive sleepiness as the preferred method to target OSA suspects for evaluation, 2 this does not always reliably differentiate those patients with or without OSA. Direct measurement of the impaired brain function caused by sleep deprivation and hypoxia has the potential to augment clinicians’ suspicion of disease and objectively assist in patient risk stratification.
The King-Devick Test (KDT) in association with Mayo Clinic is a rapid number naming test used in baseline assessments and remove from play decisions for concussion. 3 The KDT is an objective physical measure of neurologic function, allowing assessment in a quick, easily administered manner. 4 Rapid number naming requires saccades, attention, and language, as well as other areas involved in reading. 5 It evaluates function of the brainstem, cerebellum, and cerebral cortex. 5 Abnormalities in saccadic eye movements have been shown to be associated with sleep deprivation, hypoxia, and cognitive impairment—issues frequently found in patients with OSA.6-8 Prior work has demonstrated significant KDT time differences related to neurologic conditions such as dementia and Parkinson’s disease.8,9 The test is effective at detecting acute hypoxic impairment, even at early presymptomatic stages, so has promise in OSA where patients may experience repeated hypoxic events.10,11 The KDT has been utilized in a few small studies of sleep restricted or deprived subjects, but had not been employed previously in a study of OSA suspect patients.7,8
Our objective was to obtain baseline KDT times for patients suspected of OSA presenting to the Mayo Clinic Arizona Sleep Center. We hypothesized correlation between slower KDT times (ie, worse function) and greater severity of OSA. We also hypothesized that patients with OSA who adhered to continuous positive airway pressure (CPAP) treatment would demonstrate improvement in brain function as measured by decreased KDT times compared with baseline.
Methods
The Mayo Clinic Foundation Institutional Review Board approved this pilot cohort study for human subject research. We enrolled patients from January 20, 2018 to March 27, 2018 and then completed follow-up assessments until July 31, 2018. Our subjects of interest for inclusion were patients referred to the Mayo Clinic Arizona Hospital Sleep Center by Sleep Medicine Division providers for initial evaluation of sleep disordered breathing concerns. These patients received initial information about the study purposes during their consultation with providers. Written informed consent was obtained by a research coordinator in the Sleep Center on the night of their scheduled polysomnography. Patients were screened for exclusion criteria (eg, visual impairment which precluded testing, previous OSA diagnosis and treatment) As this was a small pilot study intended to provide proof of concept and explore feasibility, we made a decision to include patients with neurologic illnesses in our cohort.
We recruited subjects until we accrued 60 participants. Our sample size of 60 patients was determined based on the following power analysis. Assuming type I error 0.05 and the correlation coefficient 0.36 (weak correlation between Apnea Hypopnea Index [AHI] and KDT), we had 80% power to detect that this correlation was significant. We presumed that half of patients would have moderate to severe sleep apnea (as defined by an AHI ≥15; 30 patients) and would be candidates for CPAP. Subjects who had less severe OSA, but who were offered CPAP by their sleep medicine provider, would also be included in the OSA treatment subgroup. This size treatment cohort would produce at least 80% power to detect a 0.55 standard deviation difference in the pre- and posttreatment KDT.
Data Collection
The KDT was administered by research coordinators. These individuals were trained on its use and demonstrated proficiency. Data were collected in a standardized fashion. We measured KDT times (in seconds) for the 60 accrued subjects in the evening of their scheduled polysomnography. Following testing, those who were diagnosed with OSA and treated with CPAP had a follow-up, posttreatment KDT administered by the coordinator at their compliance visit during clinic hours. This visit was accomplished between 60 and 90 days from the initiation of treatment.
While subjects were in the Sleep Center and after obtaining consent, the coordinator collected demographic information (eg, age, gender, weight, body mass index) as well as data necessary for calculation of a Sleep Apnea Clinical Score (SACS). 12 These include presence or absence of hypertension, a measured neck circumference, and reported frequency of snoring and witnessed apnea. Our research group has recently published a study providing external validation of the SACS and has proposed a care process model utilizing it for risk stratification along with selective use of oximetry.13,14 The SACS has been a commonly used clinical prediction tool at Mayo Clinic, especially in preoperative evaluations. 15
Data Handling
Polysomnography outcomes and other clinical data were transferred from the sleep lab database. This information as well as demographic data and the SACS were entered to a REDCap database. All study data were stored in a password-protected electronic database and were handled according to HIPPA regulations. A study number was assigned to each patient and all identifying information was removed. Demographic and clinical data were entered in REDCap by the study coordinators. The study statistician transferred the data to SAS format for statistical analysis. The database has been archived after study completion.
Data Analysis
Descriptive statistics summarized demographic and clinical characteristics of the cohort. We estimated the correlation between KDT and AHI and compared the mean KDT between patients with and without OSA by the 2-sample t test. For the OSA treatment subgroup, we measured the improvement in KDT before and after the use of CPAP by the paired t test. The utilization of CPAP was quantified by the number of nights used and the hours of use per night. We also examined the reduction of AHI achieved by CPAP treatment. The results were reported as point estimates and 95% confidence intervals (CIs). The analysis was conducted by SAS 9.4 (SAS Institute) and R 3.4.4 (R Core Team). All tests were 2-sided and P < .05 was considered statistically significant.
Results
The study flow diagram can be seen in Figure 1. We approached 126 patients having polysomnography in the Mayo Clinic Hospital Sleep Center and 60 subjects were accrued. Most screening failures (48/56; 86%) were due to patients having a previously established OSA diagnosis. Only 10/126 approached patients (8%) actually declined participation. Demographic and clinical characteristics as stratified by OSA severity are seen in Table 1. Patients who had moderate or greater OSA were more likely to be obese, have diabetes and have a higher SACS.
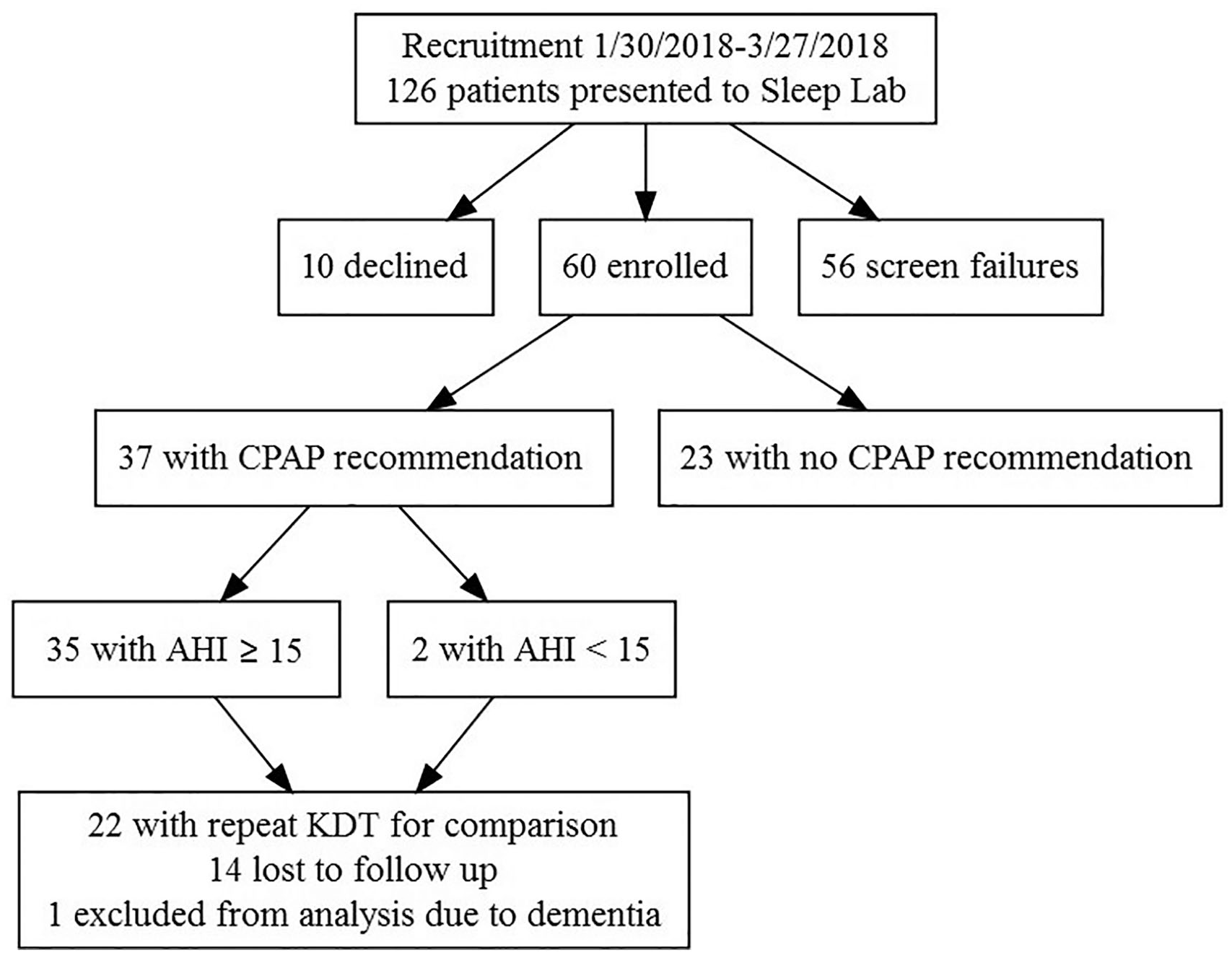
Study flow diagram.
Demographic and Clinical Characteristics of All Subjects by OSA Severity.

Abbreviations: OSA, obstructive sleep apnea; AHI, apnea hypopnea index; SD, standard deviation; ANOVA, analysis of variance.
ANOVA F test.
Fisher’s exact test.
Baseline Cohort Analyses
KDT time duration was correlated to AHI result on polysomnography neither as a continuous variable (Figure 2) nor as a categorical variable (Table 2) with our initial analyses of all 60 subjects. However, we noted that patients who had underlying neurologic illnesses (ie, mild cognitive impairment, dementia, and Parkinson’s disease) had prolonged baseline KDT times (as noted in Figure 3 and highlighted in red). We elected to remove these 3 participants from an adjusted analysis cohort. This updated analysis demonstrated that there was still not a significant association between KDT time and AHI as a continuous variable; Pearson correlation coefficient 0.10, 95%CI (−0.16, 0.35). There was now noted, however, a significant association in the adjusted analysis by examining AHI as a categorical variable (Table 3). KDT time was significantly prolonged for those patients with moderate or greater OSA (AHI ≥ 15) compared to those with no OSA or mild OSA (AHI < 15); 63.4 mean time in seconds versus 55.7 seconds; 95%CI (58.9-67.8), P = .03.

Correlation of King-Devick Test (KDT) time duration in seconds versus Apnea Hypopnea Index (AHI) from patient polysomnography.
King-Devick Test (KDT) Time Association With Obstructive Sleep Apnea (OSA) Outcome by Apnea Hypopnea Index (AHI) Categories.


Adjusted analysis of King-Devick Test time versus Apnea Hypopnea Index as a continuous variable after eliminating 3 subjects with underlying neurologic illness (highlighted in red).
Adjusted Analysis of Association of King-Devick Test (KDT) Time in Seconds and Obstructive Sleep Apnea (OSA) Outcome as Categorical Variable by Apnea Hypopnea Index (AHI).

OSA Treatment Subgroup
Thirty-seven participants were offered CPAP, 35 with AHI ≥ 15 and 2 with lower AHI (see Figure 1). We elected to exclude the one patient with a diagnosis of dementia, who was on CPAP, from the treatment subgroup in order to be consistent between the pre- and posttreatment cohorts. Twenty-two of these 36 total patients initiated CPAP treatment and followed up for a CPAP compliance visit (61%). This was when their repeat KDT time was obtained. Of the 14 patients with OSA who were non-adherent with CPAP treatment and follow-up recommendations, 5 never began treatment, 6 started treatment but did not return for their compliance visit with clinical providers, 2 were “winter visitors” to Arizona and were away during the follow-up period, and 1 returned for a CPAP compliance visit but was missed and did not complete the repeat KDT. No significant differences were noted in demographic or clinical characteristics between those who adhered to both treatment and follow-up plans and those participants who did not. Patients treated with CPAP were highly compliant, with a mean use of CPAP for 28.3 days out of the past 30 and a mean of 6.4 hours of use per night. Mean AHI pretreatment was 29.8 and mean AHI posttreatment with CPAP was 3.6; P < .001, mean difference −27, 95% CI (−35.1, −18.2).
CPAP treatment was associated with a significantly improved KDT time, reflecting improvement in neurologic function. KDT time was noted to be 63.5 seconds mean pretreatment versus 55.6 mean seconds posttreatment, creating a −6.6 seconds mean difference, P = .02, 95% CI (−12.0, −1.13) (Table 4).
King-Devick Test (KDT) Time Pre- and Posttreatment With Continuous Positive Airway Pressure (CPAP).

Discussion
Patients with sleep disordered breathing who have moderate or greater OSA on polysomnography may be more likely to have neurologic dysfunction as demonstrable by slower times on the KDT. This testing difference might not be perceptible, however, if patients have concomitant underlying nervous system illness at baseline, such as Parkinson’s disease or dementia. The treatment effect of CPAP on the associated neurologic dysfunction found in patients with OSA was demonstrated by significant time improvements on the KDT at participant follow-up. Using this tool might create objectivity regarding the subjective improvements many patients report with OSA treatment.
The ability to describe a “normal” KDT is limited. No conclusive normative data yet exist across large populations based on a patient’s age, gender, other demographic factors, or medical characteristics. Comparison of the current patient performance on KDT against their personal baseline is the optimal way to utilize these data.
The KDT is most often used in baseline assessment of neurologic function in athletes at risk for concussion. 3 In this scenario, the baseline assessment allows for comparison with KDT time after a head injury event, when it may demonstrate a slower time. This provides objective evidence of neurologic performance impact. Return-to-play decisions can be made based on noted improvement over time back to baseline.
While the obstruction noted in OSA is rightly conceptualized as being a result of a pulmonary airflow abnormality, the physiologic effects are demonstrated in multiple organ systems, including the neurologic system. Demonstration of the treatment efficacy of CPAP has traditionally been confirmed by resolution of that obstruction via recordings of decreased AHI to normal (ie, <5). While the American College of Physicians’ Guidelines on Management of OSA in Adults noted moderate quality evidence that “CPAP improves sleep measures compared with control or sham devices in patients with at least moderate OSA (AHI score ≥ 15 events/h), there was little or no evidence on CPAP on other important clinical outcomes.” 16 There are now some initial compelling data that saccadic eye movement testing, such as with the KDT, might provide opportunity for an objective pre- and post-CPAP comparator tool to confirm improvement in neurologic function. Objective physical measurement of neurologic improvement has potential to augment standard OSA management.
Unfortunately, in this small pilot study designed to test feasibility and demonstrate proof of concept, the confidence intervals in KDT time ranges noted between “normal” and “abnormal” subjects overlap, making their clinical significance unclear. However, a larger, multicenter study enrolling more subjects, perhaps with age and gender matched asymptomatic controls, might provide an opportunity to develop needed normative data or, at a minimum, generate risk stratification thresholds to aid clinicians caught in diagnostic dilemmas about how best to proceed in the work up of OSA suspect patients. Use of the KDT, perhaps in combination with clinical predication rules like SACS, 12 has potential to optimize risk stratification by proving more objective, easily obtainable clinical information which could then allow prioritization of testing for those with demonstrated neurologic dysfunction from their sleep-related breathing issues.
For patients who are found to have no OSA or mild disease and, therefore, are not candidates for CPAP, use of the KDT to monitor patients over time also conceptually holds promise. Conceivably, patients could check their KDT time at home on a regular basis and return for clinical reassessment with their providers if their objectively measured brain function was to worsen.
Assessment of CPAP treatment effect by KDT has potential to augment OSA patient management. While resolution of obstruction is noted at CPAP compliance visits via the AHI returning to normal, there may be equal import in demonstrating the improved brain function for an individual patient. It is possible that this knowledge could be a powerful motivator for behavioral changes for patients and create increased incentives for continued adherence to treatment. This hypothesis could be evaluated in future patient-oriented outcome studies. The KDT time could be used as an objective measure quantifying a patient’s subjective sense of improved wellbeing after treatment.
Conceivably, monitoring of KDT time may have utility for individual patients with milder disease or for those receiving non-CPAP treatments, such as mandibular advancement devices, positional therapy, and surgical interventions. Worsening times on the KDT could alert patients that there is a need for clinical reevaluation with their physicians.
Strengths and Limitations
These data are generated in a small number of subjects at a single institution, which potentially limit their generalizability to other settings. Our sample size calculations were set based on the smallest necessary enrollment cohort needed to find differences in KDT between those with and without disease. For convenience in this pilot study, we only included those being tested in a sleep lab with polysomnography and did not seek to include those who had home based testing. We recognize the need in future studies to control for confounding factors for neurologic performance on this function test, such as age and medical condition, especially dementia, Parkinsonism, and other issues. We would contemplate retesting all subjects to examine more fully if there might be improvements in testing based on learning and repetition. Preforming the KDT on age and gender matched controls that were not suspected of OSA might help generate needed normative data.
This pilot study offered no patient reward or inducement for participation. We relied on the typical clinical processes of appointment scheduling and reminders for follow up to occur in the CPAP treatment group. This is when we documented compliance and obtained the follow-up KDT. The rates of adherence, while admittedly not ideal, reflect the imperfection of routine clinical practice. Despite lower than expected numbers of CPAP treatment patients completing all study follow-up procedures, significant improvements in KDT times from baseline were still noted.
Completing implementation and dissemination studies in both sleep medicine specialty practices and, as importantly, in the primary care setting, would discover if both clinicians and patients considered these concepts to be valuable. We have, however, now generated proof of concept, as hoped, and demonstrated the feasibility of measuring neurologic dysfunction in OSA patients by way of the KDT.
Conclusions
A novel, objective physical measure of neurologic function, the KDT, has demonstrated potential for measuring baseline abnormalities in patients with OSA of moderate or greater severity. Significant neurologic improvement can be objectively measured after patients are treated with CPAP. Future studies may discover KDT time thresholds for various AHI diagnostic levels in OSA suspect patients, possibly aiding clinicians’ risk stratification and management decisions.
Footnotes
Authors’ Note
Posters of this work were presented at the North American Primary Care Research Group Annual Meeting November 12, 2018 in Chicago IL USA, the International Forum for Quality and Safety in Healthcare, Glasgow Scotland United Kingdom, March 28-29, 2019 and at Optometry’s Meeting, St. Louis MO USA, June 19-23, 2019.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lori Grover, OD, PhD, was Senior Vice President for Policy, King-Devick Technology, during the conceptualization and conduct of this project and reports a current financial interest in the company.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Mayo Clinic Arizona Research Committee Small Project Grant (#17-003889). The use of the REDCap database is supported by Mayo Clinic Center for Clinical and Translational Science, which is supported by CTSA Grant Number UL1 TR000135 from the National Center for Advancing Translational Science (NCATS). King-Devick Technology provided in kind funding for the use of the King-Devick Test in association with Mayo Clinic for this study.