
Abstract
Background
The ultimate goal of the health system of each country is to promote the health of all people so that they can actively participate in economic and social activities, while having adequate health. 1 Undoubtedly, today the main strategy for countries to achieve this goal is primary health care (PHC). 2 PHC has been established in Iran since 1985 in the form of health care networks in different cities and villages. 3 In PHC, the first and widest community contact with the health system has taken place. Service provider units at this level include health houses, health posts, and rural/urban comprehensive health centers (CHCs). Health care providers in health houses include male and female Behvarz and in health posts include family health nurses. In comprehensive urban/rural CHC, general physicians, sometimes dentists, nutritionists, psychologists, and occupational and environmental health experts are usually working4,5 (Figure 1).

The structure of primary health care in Iran.
The performance and pattern of PHC in Iran has an international reputation and has been visited and praised by experts from various international organizations. 6 Today after about 32 years of PHC initiative in Iran in the form of health care networks, many achievements and successes have been obtained in promoting health indexes. 7 Despite the brilliant achievements, especially in rural areas, some challenges have emerged in recent years in the field of provision of health services, especially in urban areas. The most important of these challenges are the changing of disease patterns from infectious to chronic, the population aging, unsustainability of resources, hospital-centered health services, use of untrained physicians in managerial positions, deterioration of health centers’ building, changes in people’s needs, increasing urbanization and growing marginal areas of cities with special health needs.7,8 Therefore, the need for fundamental reforms in the management and provision of PHC, especially in urban areas, seems unavoidable. 9
Today, different strategies have been used to cope with the challenges of health care system in different countries. The most effective strategy can be public-private partnership (PPP) as a bilateral collaboration and a win-win policy, making use of the abilities of both sides to achieve their goals. 10 The private sector knows PPP as an opportunity for market growth and making profit that provides appropriate facilities and innovative management for the public sector.10,11 Public sector also use PPP as an efficient and cost-effective key mechanism to achieve goals and implement policies. 12
Another area that seriously addresses the potential use of PPP is the universal health coverage (UHC). UHC is the third goal of sustainable development goals, which most countries are aiming to achieve by 2030. 13 The UHC’s goal is to maximize health outcomes through the equitable distribution of financially and geographically accessible high-quality services, ensure efficient service provision, and low out-of-pocket payments in proportion to the individuals’ affordability. 14 Countries that seek to realize UHC should use all available resources, including the private sector. So, certainly, PPP is one of the basic strategies for achieving UHC. 15 In the Islamic Republic of Iran, in the upstream documents and in many legal articles, PPP has been addressed by national policy makers, which indicates the importance of this issue and support of higher levels of decision-making body.
Various experiences with PPP implementation in PHC have been reported in different countries. For example, the results of a study conducted in Kenya by Bakibinga et al 16 show that access to and utilization of health services for women, children, and infants has been improved through PPP implementation. The status of these centers has also been improved in the areas of infrastructure, human resources, information, finance, equipment, and supplies. 16 Another study by Baig et al 17 in India compared the 3 PHC models, including public, NGOs (nongovernmental organizations), and PPP centers, based on health indexes, managerial performance, and service quality in the view of service recipients. The results showed that there was no significant relationship between the 3 service models based on studied dimensions. In general, public centers were better than other models in access to services, medicines, and infrastructure. On the other hand, NGOs and PPP centers are better than public centers in the provision of laboratory services. All 3 types of service provision models had poor performance in the field of human resources and achievement of predetermined managerial goals. 17
In Iran, several studies have been conducted to measure the success of PPP, which show the positive outcomes of this policy. For example, the results of the study by Pour Dolati et al 18 study showed that the implementation of the PPP policy has led to improved case finding, patient satisfaction, and affordability. On the other hand, the results of the study conducted by Nikniaz et al 19 indicated that compared with public centers, PPP centers have better performance in maternity and child services.
In 1998, health cooperatives were designed by senior managers at the University of Medical Sciences and rolled out in a pilot study at the provincial level in East Azerbaijan Province (EAP). Health cooperatives were a model of PPP that provided the PHC services in the form of a clear and integrated service package using a market-controlled pattern and private sector approach. Through continuous evaluation and based on the quality of services, the public sector’s reimbursement was based on pay for performance and capitation. 20
Since early 2014, the initial design for the establishment of health complexes (HC) began as a fundamental strategy for strengthening the health system and moving toward the UHC. This was based on the study of upstream documents, successful reports from other countries, health cooperatives’ experience in the EAP, and a comprehensive analysis the current state of public and private sector. Modification and finalization of the HC plan was carried out based on the views of the Deputy of Health of the Ministry of Health (MOH), the University’s Board of Directors, experts, and consultants from different departments of medical university. The executive guideline, the contract text, and the service package were drafted during April and May 2014. After the approval in the University’s Board of Directors, the rollout of the first HC took place in June 2015, and following initial evaluations and revisions to the plan, the launch of other HCs began in February 2015. Since May 2015, the rest of the province’s cities were gradually covered. 20
Although health cooperatives and HCs have both been implemented with the aim of PPP implementation in primary health care, there are some differences between these 2 models. Health cooperatives covered between 9 and 17 000 people, while the population covered by HCs is between 40 and 120 000. HCs consist of several health centers, which one of them is CHC. The population covered by each of these centers approximately equivalent to covered population by a health cooperative. The CHC has 4 specialist physicians (internist, pediatrician, gynecologist, and psychiatrist) who provide specialty services for referrals by family physicians and family health nurses who work at health centers. The nutrition and mental health services added to the service package provided by HC compared with health cooperative. More information on health cooperatives and HCs is provided studies by Tabrizi et al, 20 Farabakhsh et al, 21 and Bakhtiati et al. 22
Given the passing of about 4 years of implementation of PPP in the provision of PHC policy in EAP, it is necessary to review the performance and achievements of this policy. The purpose of this study was to analyze the PPP in PHC policy in EAP.
Methods
In this study, the policy analysis triangle framework was used. This model that designed in 1994 by Walt and Gilson 23 to analyze health policy, covering 4 sections. In each section of the policy triangle, the following information examined:
Research Environment
This study was conducted in EAP, the largest and most densely populated province in the northwest of Iran. Based on the population and housing census in 2016, the population of the EAP was 3.9 million, of which 2.809 million (72%) settled in urban areas, of which 530 000, (19%) settled in city marginal areas.
Participants
The participants were informed experts from the following organizations and sectors: Senior officials and managers from the Vice Chancellor for Health of University of Medical Sciences (VCH) and its subordinate units, senior officials and managers from health networks and Tabriz district health center, and experts and authorities from private sectors.
Data Collection
The required data were gathered using qualitative methods. Initially, the required information extracted from the documents related to the development and implementation of the policy (including the regulations, minutes, instructions, recalls, contracts, and other related documents) in the information system of the VCH. In the next stage, interviews were conducted with stakeholders and individuals involved in the implementation of the policy.
At the last stage of the study, semistructured interviews were conducted with 14 current and former managers of the VCH, district health networks’ managers, faculty members with a history of executive and scientific work on PPP, and managers of private HCs. The sampling method was purpose based and participants were selected heterogeneously. Inclusion criteria for participants were having at least 5 years of management experience or executive activity in relation to the providing PHC services, faculty members with a background in PPP research, having at least bachelor’s degree in medical sciences, having enough knowledge in PHC (publishing books, papers, reports, etc), and having the desire and ability to participate in the study.
Interview sessions were planned and implemented based on the willingness of the participants and with prior notice and sending information sheets including the objectives, methodology and interview questions. Each session lasted between 40 and 150 minutes, and the participants were free to leave the study if they deprecate the process of sessions and how to use the results. With the consent of the participants, their conversation was recorded and after each interview transcribed immediately. In addition, notes were taken during the interviews.
To increase the consistency and accuracy of the study, 4 criteria proposed by Guba and Lincoln 27 (including credibility and confirm ability, dependability, and transferability) were applied. In order to obtain credibility and confirm ability criteria, submergence and review by research colleagues and participants and expert opinions were used. For dependability, 2 people were used for coding. Finally, for transferability, the experts’ opinions, as well as heterogeneous and purposeful sampling, were used.
Data Analysis
Data were analyzed by content analysis method. The text of the interviews was reread several times to fully understand the concepts and themes; then the data were coded, then main themes were extracted from the primary codes. Data encoding was done by two researchers. In data analysis, criteria of acceptability, transparency, integration, repeatability, and reliability were applied. Results from the review of documents are presented descriptively in the results section. MaxQDA10 software was used for content analysis.
Ethical Approval
The study had been approved by the Ethics Committee of the authors’ institute (Ethical Number: TBZMED.REC.1397.597). Ethical issues (including the informed consent of the participants, plagiarism, duplication, etc) are fully respected by the authors. The confidentiality principles are respected in the information of individuals. The individuals have been assured that the results of the study would be used only for the purposes of the study not in any other cases, and each person was allowed to leave the study at any stage of study without any loss.
Results
The findings of this study are presented in 4 sections: context, content, stakeholders, and process.
Context
Contextual factors were classified according to the Licher’s method 25 (Table 1).
Contextual Factors of Public-Private Partnership in Primary Health Care Policy in East Azerbaijan Province, Iran.

Abbreviations: HEP, health evolution plan; PHC, primary health care; PPP, public-private partnership; HC, health complex; MOH, Ministry of Health; VCH, Vice Chancellor for Health of University of Medical Sciences; UHC, universal health coverage.
Content
Policy Objectives
One of the important issues in this section is the objectives of the PPP in PHC policy. Different participants had stated different objectives for this policy, which were addressed in 6 themes (Table 2).
The Objectives of Public-Private Partnership in Primary Health Care policy in East Azerbaijan Province, Iran.
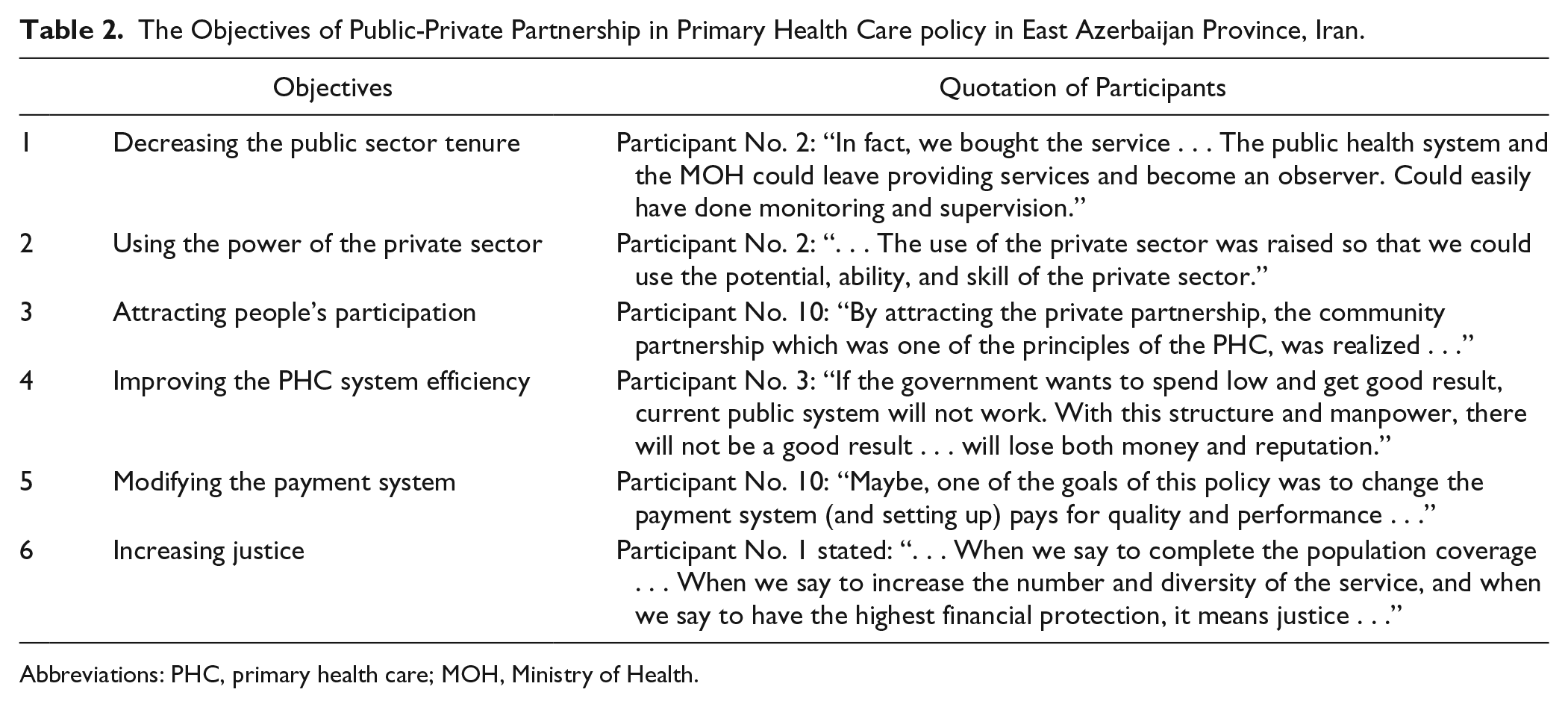
Abbreviations: PHC, primary health care; MOH, Ministry of Health.
Contract
The policy design team from the VCH, with the help of members of the University’s Legal Affairs, Vice Chancellor for Resource Management Affairs of University of Medical Sciences, university security department, and representatives of private sector, developed the initial contract considering current conditions. This contract included the following items:
Stakeholder Analysis
The characteristics of the stakeholders have been determined by kind, position, motivation, and effect (it should be noted that all the characteristics were not exactly extracted from the interview but, based on the experience of the research team, the status of the stakeholders was determined on the basis of these characteristics; Table 3).
Key Stakeholders of Public-Private Partnership in Primary Health Care Policy in East Azerbaijan Province, Iran.

Based on the information obtained from stakeholder analysis in the present study, a stakeholder position map was designed at three levels of national, university, and other organizations out of health system. In this study, University of Medical Sciences was considered as the main responsible organization for this policy (Figure 2).

Position map of key stakeholders of public-private partnership in primary health care policy in East Azerbaijan Province, Iran.
Process
The study results in this section are discussed in 4 sections “agenda setting,” “policy design,” “policy implementation,” and “policy evaluation.”
Agenda Setting
In this section, the factors leading to the setting this policy as the agenda is presented in the form of problems, policies, and political streams (John Kingdon, 1984, 26 Figure 3).

The flow of multiple streams about the agenda setting of public-private partnership in primary health care policy in East Azerbaijan Province, Iran.
Development Process
The development and preparation of the policy is illustrated in Figure 4.

The process of developing public-private partnership in primary health care policy.
Implementation
The dimensions of the implementation of the policy were examined in 7 areas (Figure 5).

The implementation of public-private partnership policy in primary health care in East Azerbaijan Province, Iran.
Further details like the human resource composition, reimbursement methods to HCs, and so on are being published in other under review papers.
Evaluation
(a)
(b)
The Weaknesses and Strengths of Public-Private Partnership in Primary Health Care Policy in East Azerbaijan Province, Iran.

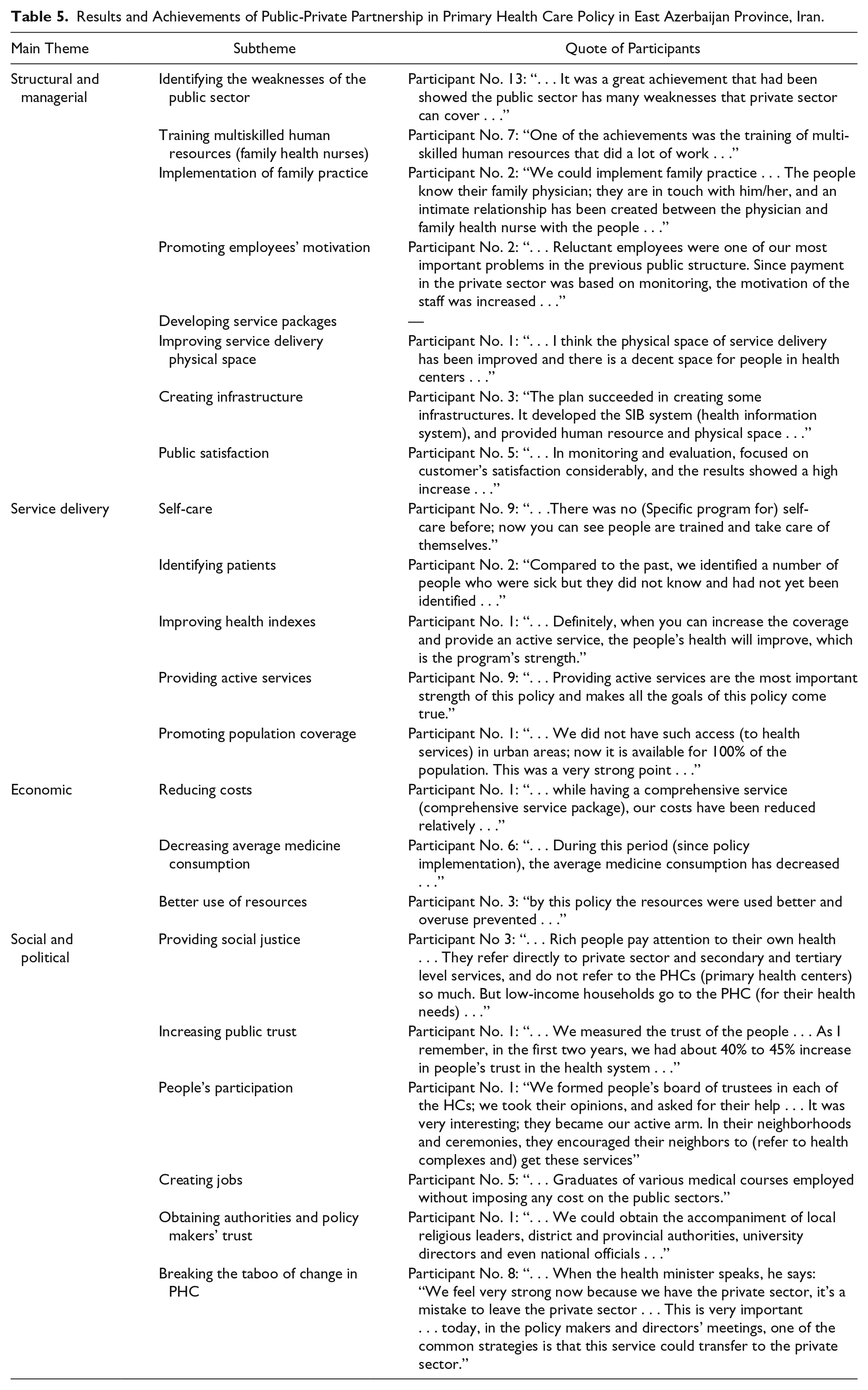
Results and Achievements of Public-Private Partnership in Primary Health Care Policy in East Azerbaijan Province, Iran.
Discussion
About 10 million people in Iran live in the marginal areas of big cities. Regarding the poor health in the marginal areas of cities, MOH has considered health interventions in order to improve the health status of these areas. 13 Implementation of the HEP in EAP has different features and structure and this province has many innovations in this field. In this study, PPP in the provision of PHC policy in the EAP has been analyzed.
Context
The results of the study showed that the support of PPP by the political parties was one of the factors influencing the implementation of this policy. But this support was only provided in the early stages of implementation; later political support diminished, which causing problems with the execution of the plan. Economic problems and financial resources unsustainability can also be due to weak political support. In the study of Christia et al 31 in Guatemala, major changes to the PPP in PHC program due to election and government change was one of the challenges of the plan.
On the other hand, it seems that the coincidence of implementation of this policy with the implementation of the HEP in the country, which brought a lot of financial resources to the health system, have led to all required budget for PPP policy be provided. When the government faced economic fluctuations, the health budget also fell sharply, and the PPP in PHC policy is no exception, and since then, there have been many problems that could jeopardize the existence of the policy. In a study conducted in Bangladesh by Islam et al, 32 an assessment of PPP policy in providing PHC in urban areas, showed a reduction of state aid from 26% of the total project budget in the early stages of the plan to 12%, can led to uncertainty in the project’s continuity in the following years.
In general, most participants believed that because of the availability of technical expertise in the public sector, especially the scientific capability and experience of the policy designer team, there was no way to official and policy makers to opposite this policy. Also, technically, especially in the field of human resources, there was no such problem which can drop the existence and continuity of the policy into trouble. The only technical problem was the shortage of physicians, which has been one of the main concerns of health system in PHC sector since past. This is considered due to better working conditions in other sectors in comparison with PHC. The results of the study carried out by Islam et al 32 showed that physicians are reluctant to attend in PHC, due to lack of professional development and low salaries.
In general, cultural barriers did not affect the development of this policy, but there were some cultural problems in the implementation phase due to the issues such as lack of familiarity with policy in different organizational levels of public sector. It seems that proper public notification is necessary to justify all public sectors, other public organizations (health insurance companies, municipality etc), politicians and people before and after the implementation of the policy.
Content
From the findings of this study, it can be concluded the social justice was the main goal of policy implementation, although other organizational goals also were followed. The social justice is the driving force and the main goal of many reforms and interventions in health systems.33,34 The 2008 World Health Organization report highlights social justice as the main pillar and key component of PHC reforms. 35
Stakeholder Analysis
The number of university internal stakeholders who support the policy is considerable; hence the likelihood of formation a coalition is high. University officials can attract these stakeholders’ cooperation through involving them in redesigning and implementation process. There are various ways to get support of insurance companies and other university’s vice chancellors, who are neutral for this plan. They can be involved in the process of implementing or redesigning and modifying different parts of the plan. They should also be encouraged to engage in the implementation of this policy using various methods such as providing financial and non-financial incentives. They must be persuaded to support PPP in PHC policy and increase their power to the extent necessary.
On the other hand, private-sector physicians are considered to be opposing stakeholders who have moderate leadership and power, which their power should be reduced, or could negotiate with them and justify them about the benefits of the plan, or could offer incentives for their coordination with the plan. It seems that attracting the intra-organizational supporters will strengthen the position of the policy against private-sector physicians.
More decision-making power can be given to people and the private companies that support the plan, but lack leadership and have moderate to weak power, to increase their power and leadership. They can be invited to participate in the implementation process and solve the challenges and problems; which is one of the health socialization ways. Also, health education through mass media, creating various grassroots campaigns, and attracting people’s participation in identifying problems and planning to solve them are the other effective solutions that can strengthen these supporters and facilitate the health socialization.
In order to preserve the support of stakeholders who have high power and leadership, basic concepts and achievements of policy must be explained to them and get their help to solve problems and provide solutions for the challenges of PPP in PHC policy. For example, Department of Education’s influence on parents can be used to provide better health education and periodic health examinations services to students and households.
In order to attract the support of public sector employees who were the opponents with no leadership and low power, continuous and planned coordination meetings can be organized. It is also possible to explain the various dimensions of the plan to them and use their comments and assure them that the implementation of the plan will not endanger their interests.
Process
Agenda Setting and Development Process
It seems that the public sector’s inefficiency in providing PHC is the main problem stream that set PPP policy in agenda. The existence of facilitating laws and national and international goals, along with the presence of a policy designer team who had experience of implementation of PPP in the form of health cooperatives in 1998 and the positive outcomes of that plan, provided a platform for proposing this policy to improve current system.
On the other hand, the coincidence of PPP policy with the HEP was an opportunity to facilitate the development and implementation of this policy. Organizing coordination meetings and inviting managers who had participated in the experience of the health cooperatives, as well as inviting private sector representative and academic specialists to attend service package, monitoring, contract development, and calculating capitation, and meetings during the policy development phase are the strengths of this policy and kind of innovation.
Implementation
It seems that the considerable points in the implementation of this policy are coordination meetings, staff training method, establishment of referral system, and monitoring and evaluation method. But for the continuity of these strengths, it seems necessary to sustainability in management and policy implementation style.
Evaluation
Some of the weaknesses of this plan were predictable and correctable before the implementation, and they should have been considered by the design team. On the other hand, there were unpredictable problems and weaknesses that were identified during the implementation. Since there was not much experience in this field in Iran, incidence of some problems and weaknesses were not unexpected. But it seems that, as many participants suggested, a pilot study could help identify and resolve these weaknesses before implementation the plan on a wide scale.
The results of this study emphasized more on the “lack of infrastructure” as a fundamental weakness. It seems that the project’s executives considered solving of some infrastructure beyond the health system, because it requires a change in the national level by all beneficiary institutions and organizations which are not easily possible. On the other hand, the time limitation was one of the serious obstacles to the solution of the infrastructure problems of this policy, which could cause it to stop. It seems that the solution of the aforementioned problem requires comprehensive political support from the beneficiary upstream institutions. In the study by Dehnavieh et al,35 who examined the implementation of PPP in PHC policy as an experience in health system reform, lack of facilities, high workload due to lack of some human resources—specially physicians—unsustainability in financial resources, and lack of health insurance companies’ cooperation have been identified as the weaknesses of this policy.
The main strengths of this policy, in terms of high emphasis and consensus of participants, were improving access to services, active follow-up, providing secondary health services alongside PHC, changing the role of the public sector, accurate monitoring and evaluation, and setting up pay for performance and quality of service system. Despite the emphasis of public sector interviewees on the accuracy of monitoring and evaluation, the private sector representatives believed that there are some deficiencies in monitoring and evaluation system; which the quality and accuracy of the process could be improved through eliminating them. Stakeholders’ opinions indicate that one of the solutions to this problem would be to organize coordination meetings between the public and private sectors to achieve common language. Based on the results of the study by Dehnavieh et al, 36 decentralized planning, strengthening the engagement of the private sector, using the performance assessment methods more appropriately, using the prospective payment method, strengthening the referral system, strengthening service continuity, facilitating financial access, and increasing geographical access especially in marginalized areas, are the strengths of this policy.
The main achievement of this policy, in the view of interviewees, was the improvement of social justice (through the improvement of access, quantity, and quality of service) that all participants agreed on. The interviewees believed that the implementation of the plan had improved the access and utilization of poor and marginalized people. In the study conducted by Bakhtiari et al 22 exploring the results of PPP in PHC policy at EAP, it was shown that financial, physical and even cultural access (service acceptance) to PHC services has been improved. The results of the study carried out by Reeve et al 37 showed that, about 6 years after the strengthening of PHC in Australia, the quantity and quality of care provided to marginalized people have been dramatically increased, which was higher in deprived areas.
Despite the mentioned strengths and weaknesses, stakeholders have described this policy as relatively successful and helpful in solving the problems of the PHC system. This seems to be a good ground for gaining stakeholders’ support to form a unified and powerful coalition to address problems.
Study Limitations
Since this study is the policy analysis in a retrospective way, one of the limitations of the study is the recall bias that can affect the accuracy of the information. In a part of this study, the existing documents were used to extract information. Given that this information was not collected for research purposes, some of them were less suitable for study purposes.
Conclusions
Simultaneously with the implementation of the HEP in Iran, EAP developed and implemented PPP in PHC policy in order to achieve UHC, which have significant differences with the country model. Analysis of this policy showed that the implementation of the HEP at the country level and the political support for these reforms paved the way for implementation of PPP in PHC policy in EAP. The results of the study indicate that the main goal of this policy was to realize UHC with an emphasis on marginalized areas, expansion of service packages, and reduction of out of pocket payments. On the other hand, this policy has not faced serious opposition from the various stakeholders. Also, according to the results of the study, the main reason for the design and implementation of PPP policy in PHC was the public sector inefficiency to completely provide PHC to all people. The main part of the development of this policy in EAP was conducted by a team from VCH in cooperation with various departments of university of medical sciences and the views of national authorities of the health system were used to edit and correct it. This policy was implemented in the form of private HCs using a defined service package and capitation payment for a specific population on the margins of EAP’s cities. The results of qualitative and quantitative evaluation of this policy indicate it’s relatively successful. But the continuity of policy success requires comprehensive political support, sustainable financing, organizational and political sustainability, coordination between the university’s internal departments and between politicians and national level authorities, and the constructing culture among people and authorities through notification about the achievements and successes of the policy. Given the nature of health care, in a short period of time it is not possible to extract output and effectiveness data, except in a limited number of cases. So, designing a systematic and accurate program to measure and evaluate the success of this policy accurately, would be useful. Policy designers can use the extracted information to attract stakeholders and identify the strengths and weaknesses of the policy.
Footnotes
Acknowledgements
This is part of PhD thesis funded and supported by Tabriz University of Medical Sciences and Tabriz Health Services Management Research Center. Hereby, we appreciate all the participants from the private and public sectors in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study supported by Tabriz Health Services Management Research Center, Tabriz University of Medical Sciences. However, the Research Center played no roles in study design, data collection, analysis, writing or submitting to publication.