
Abstract
Keywords
Introduction
People with serious mental illness (SMI) experience significant disparities in morbidity and mortality.1-3 There is a call to action to address the “deadly consequences” 4 of SMI and the “lethal discrimination” 4 toward people with SMI. Preventable and treatable medical conditions are the major contributors to this disparity, with cancer as the second leading cause of death.5,6 While there is considerable between-study variance, recent cohort studies reveal that women with schizophrenia have almost three times the risk of breast cancer incidence and mortality, with a standardized incidence ratio of 2.9.7,8 and a standardized mortality ratio of 2.8. 6 Women with SMI have low mammography screening rates. 9 Severity of diagnoses is strongly associated with lower initial and follow-up screening rates,10,11 as are larger health determinants such as lower income and limited access to health care. SMI, poverty, and poor access to care have a significant effect on a woman’s opportunity to learn about and discuss breast cancer screening with health care providers.
Shared decision making (SDM) is an effective intervention for complex risk communication. SDM is helpful for decisions about breast cancer prevention because of the individualized screening decisions. 12 Additionally, visual aids may increase understanding of mammography screening and are positively associated with SDM. 13 People with psychotic disorders can specifically benefit from SDM to promote autonomy, empowerment, and participation in care.14,15 Limited information is available on SDM for medical decisions in people with SMI, and this population is often not included in the decision-making process for medical conditions. However, most patients with mental illness want to be involved in their health care decisions. 16
The aim of this study was to examine the outcomes, feasibility, and acceptability of a pilot mammography decision support and navigation intervention (DSNI) for women with SMI living in supportive housing settings. This study was grounded in the preventive health model (PHM) theoretical framework, described in the next section. Our primary hypothesis was: The DSNI approach will increase knowledge, promote favorable attitudes, and decrease decisional conflict relating to screening mammography, as well as support mammography completion. This hypothesis was tested through baseline and follow-up surveys with the participants regarding knowledge, attitudes, and decisional conflict, and measure of the number of completed mammograms. Our secondary hypothesis was that the DNSI will be feasible to implement in supportive housing settings and acceptable to women with SMI. Feasibility will be measured by process measures of the decision support and navigation interventions of the study including percentage of women completing the decision support module, number of navigation attempts, number of completed navigation conversations, participant assessment of the intervention, and navigator reported barriers to navigation, and barriers to mammogram completion. Acceptability will be assessed through semistructured interviews with the participants regarding their experience with the decision support and navigation components of the intervention.
Theoretical Model
To our knowledge, there have been no reports in the literature on the use of theory-based intervention methods and SDM to increase mammography screening in women with SMI. The PHM, a well-accepted self-regulatory framework forms the basis for the intervention in this study, as shown in Figure 1. The PHM considers the “self-system” as critical in explaining the use of preventive health modalities, such as screening, that are intended to diagnose, risk-stratify, and prevent chronic disease. According to the model, the self-system includes both sociocultural health background; as well as cognitive, affective, and social representations about disease, risk, and available preventive health behavior alternatives.17-19 The PHM, which has been useful in predicting outcomes such as cancer screening intention and utilization,20,21 has also been used to develop the decision counseling intervention used in this study. Decision counseling is a mediated decision support intervention method that involves education about decision alternatives faced by patients, and clarification of a preferred alternative, for example, decision to undergo or not undergo mammography screening. Results of a decision counseling session set the stage for the definition of an action plan and implementation of that action plan, such as scheduling a mammogram. The PHM posits that a patient is more likely to implement the action plan, such as scheduling and completing a mammogram when they are assisted with navigation to address the cognitive, affective, and social obstacles to behavior detailed in theoretical model. These may include navigation elements such as assistance with making an appointment to receive a mammogram referral, arranging transportation to and from the appointments, and so on.

The preventive health model. SMI, serious mental illness.
Description of the Intervention
Two participatory research projects informed the development of the intervention and have been described elsewhere. 22 The DSNI consists of 2 elements: (1) an educational and decision support session followed by (2) ongoing navigation through mammography completion. The elements of the intervention and linkage to the PHM are described in detail below (Figure 2) .
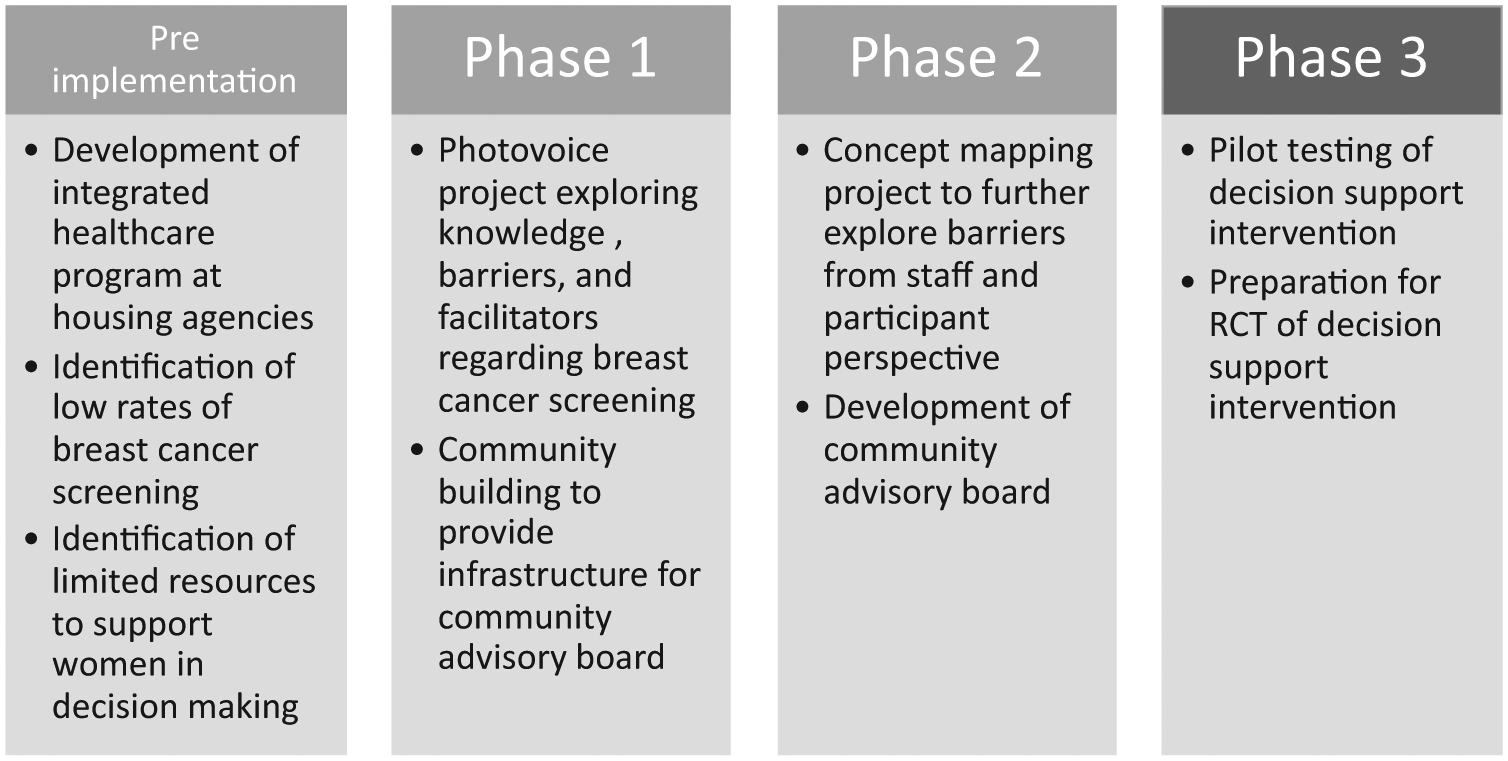
Participatory development process of the intervention. RCT, randomized controlled trial.
We designed the educational component to address the interpersonal self-system elements of the PHM such as perceived risk of breast cancer, anticipated outcomes of screening, sociocultural health background, and cognitive, affective, and social perceptions of breast cancer. To develop the educational module, we conducted a literature review and consulted with topic and design experts with the aim of adapting already published print and electronic materials focused on breast cancer risk, mammography experience, and vulnerable populations who may experience cognitive challenges and/or affective disorders. Women from the community were involved in the design and content development of the educational module on multiple levels to enhance sociocultural relevance for the population. Illustrations and quotes felt to be culturally meaningful and relatable were taken from the previous photovoice project. Women who participated in the preliminary projects provided voice-overs for some of the slides. The final module consisted of 32 slides designed for interactive review. Approximately 15 minutes were needed for the decision counselor to review the slides and to answer participants’ questions.
The decision support component was grounded in the intrapersonal decision-making support system of the PHM and focused on intention and planning as well as preference clarification. Decision support was delivered using the Decision Counseling Program (DCP) and a research assistant formally trained as a decision counselor. The DCP is an online software application that guides the decision counselor and participant through a structured encounter. Following the script, the decision counselor elicited major factors that would influence the participant to have or not to have a screening mammogram (pros and cons), determined the level of importance the patient assigns to each factor (not important to overwhelmingly important), entered the reported factors and factor weights into the DCP, and computed a screening likelihood score (low to high) indicating preference toward having a mammogram or not having a mammogram.
To support planning and action, the decision counselor used the DCP to print a 1-page summary of the session for the participant. The decision counselor instructed the participants who preferred mammography screening to follow-up with their primary care provider and obtain a referral for a mammogram.
The navigation component of the intervention correlates with the intrapersonal decision-making support system and the macro system of the PHM. Preliminary navigation and support occurred at the conclusion of the decision counseling session. The research assistant contacted study participants by phone or in person monthly to offer support of their preferred decision and assistance as needed with elements of the macro system, such as scheduling a mammogram, obtaining a referral, arranging transportation, and following up abnormalities if necessary. We referred study participants without a primary care physician to the [Project HOME] federally qualified health center.
Methods
Study Procedure
Participants were encouraged to attend a baseline and 1-month follow-up intervention session. At intervention session 1, participants met one-on-one with the decision counselor/research assistant for an initial 90-minute educational and decision counseling session. Intervention session 2 occurred one month later and consisted of an in-person navigation session to further assist participants who indicated they wanted to have a mammogram. Participants and their care managers were contacted by project staff via telephone during the 6 months between session 1 and the final data collection session to offer information and practical navigation support. The research assistant documented all attempted patient navigation contacts.
Study Setting
We implemented this study in partnership with [Project HOME] and [Pathways to Housing PA], two nationally recognized agencies working to end homelessness for people with SMI in [Philadelphia] through permanent supportive housing.
Recruitment and Sampling
We recruited participants through a combination of recruitment flyers posted at the residences, presentations at tenant meetings, word of mouth, and care coordinator referral. To be eligible for participation, women needed to (1) be age 40 years or older (following the then current American Cancer Society 2003-2015 Breast Cancer Screening recommendations) 23 with an SMI diagnosis, (2) have not received a mammogram in the past year by self-report, and (3) be part of the [Project HOME] or [Pathways to Housing PA] supportive housing programs. Exclusion criteria included decisional impairment or active psychosis, as verified by the participant’s psychiatrist. All participants approached agreed to be part of the project. The original sample included 23 participants, 1 participant passed away from chronic medical problems unrelated to the study, and 1 participant was found to be ineligible after enrollment. Therefore, the final sample included 21 participants.
Data Collection
At study session 1, participants completed a baseline survey before the education and decision counseling session and took part in a semistructured interview. At session 2, the participants completed a 1-month follow-up survey. Participants also completed a 6-month follow-up survey and took part in a second semistructured interview.
Measurement Instruments
We administered in-person surveys at baseline, 1 month post baseline, and 6 months post baseline. To potentially identify any relationship between the participants’ mental health and study participation and experience, we included measures of psychiatric symptoms and mental health recovery.24-26 We included a survey based on the PHM, which is used to predict outcomes in cancer screening intention and utilization.27,28 Two additional surveys were included to identify changes in breast cancer knowledge and decision conflict.29,30 Further details of the measurement instruments are listed in Table 1.
Description of measurement instruments.

The semistructured interview after session 1 was designed to explore the participants’ experience of the experiences and attitudes toward the education and decision support session, with specific questions exploring certain constructs of the PHM, including the relationship between the educational module and the intrapersonal support system and the relationship between the decision support session and the interpersonal decision-making support system. The purpose of the 6-month semistructured interview was to elicit the participants’ experiences and attitudes toward the navigation experience. Specific questions considered additional constructs of the PHM, including any changes in the intrapersonal support system and the interpersonal decision-making support system. Additional interview questions explored the PHM construct of empowerment and values clarification as related to participants’ experience of control over their health.
Data Analysis
To assess outcomes, we tracked the participants’ preferences regarding breast cancer screening following the DCP and considered the difference between the baseline and 1-month scores on each outcome (the 6-month surveys were dropped from analysis because of low response rate [n = 8]). We estimated the mean pre/post change and 95% confidence interval via a paired t test. We analyzed demographic information using mean and standard deviation for continuous variables and frequency counts and percent for categorical variables.
To examine the feasibility of the intervention, we tracked process measures of the navigation component and conducted qualitative baseline and 6-month follow-up interviews about the experience with selected participants. Process measures of the navigation component included number and type of contacts and review and summary of the navigation logs. To assess acceptability, we analyzed the interview transcripts using a modified grounded theory approach 32 and NVivo10 software. 33 A 5-person coding team began by individual inductive, open coding of the data into categories and concepts of meaning, then as a group the team considered relationships among the codes through axial coding and concluded with a process of selective coding, identifying emergent themes.
Approvals
The project received approval from the [Thomas Jefferson University] Institutional Review Board, the [City] Institutional Review Board, and by [Project HOME] and [Pathways to Housing PA] administration. All participants completed an informed consent, and a records release form allowing the study team to contact their primary care provider and/or mammogram facility to obtain results of their mammogram and any additional follow-up testing. Each participant was compensated $20 and 2 transportation tokens (if traveling from their residence) for each of the 3 study sessions they attended. Data collection took place in 2014; data analysis took place 2014-2016.
Results
Outcomes
Table 2 shows the demographics. The 21 participants were mostly African American women with a high school degree or above. Over half the women smoked cigarettes (62%), and one-fourth reported a family history of breast cancer (24%). Regarding knowledge, attitudes, and decisional conflict, there was no change in breast cancer knowledge or orientation toward screening. The Decisional Conflict Scale decreased significantly from baseline to 1-month postintervention (P = .01, 95% CI 2.00-15.38), implying a decrease in concerns related to mammography. In general, the participants scored in the high range in measures of psychological recovery and breast cancer knowledge, reported low psychiatric symptoms, and were oriented toward screening. There was no relationship between psychiatric symptoms or mental health recovery and measures of breast cancer knowledge, orientation toward screening, or decisional conflict. Table 3 shows the results of the baseline and 1-month post surveys.
Demographics of mammogram decision support participants.

Pre-Post Survey Results.

In the individual results from the DCP, the scores of 17 participants indicated that they (71%) preferred to have a mammogram, three preferred not to have a mammogram, and one participant was unsure. A total of 14 participants (67%) reported receiving a mammogram.
Feasibility
All women were able to complete the education and decision counseling session. The research assistant was able to deliver components of the navigation process. The patient navigation process resulted in 270 attempted contacts (phone calls and emails) (M = 12.86, SD = 10.61) by study staff to the 21 participants and/or their case managers) (mean attempts per participants = 12.86, SD = 10.61). Of those attempts, 61% (165) navigation conversations occurred with the 21 participants and/or their case managers (mean conversations per participant = 7.86, SD = 4.84). Case managers provided additional navigation support for 71% of the participants. Identified barriers to navigation included missed phone calls, participant availability, participant willingness to speak, and staff availability. Barriers to mammogram completion included missed appointments, need for referrals, and need for prior mammography films.
Acceptability
Baseline (N = 10) interviews revealed the participants were generally enthusiastic about the education and decision counseling element of the intervention. In terms of the interpersonal self-system, participants appreciated learning about anticipated outcomes. For example, one participant felt it was helpful to learn about the process for having a mammogram, when it comes to someone that never had one before that will help greatly because it gives you step by step of everything and I wish [/tests were/] like that to make it more easier and take the fear away from a lot of people. (P3).
Participants commented on both helpful and unhelpful elements of the education module in terms of overcoming cognitive and informational barriers. For example, one participant commented on the usefulness of the visual information, you were talking and the pictures were there to see you know, what you was talking about . . . the more you talk about it, it’s altogether different looking at it, than just to talk and not know what you are looking at. (P9)
However, participants found the varying age recommendation confusing, It sounds like it’s pretty subjective, whatever organization I choose to follow and I don’t really know how to make that decision, I’ll defer to my doctor. (P5)
Participants also suggested the educational module include more information on anticipated outcome, for example what to do if the mammogram is abnormal. One participant gave an example, if they would find a lump, and it was cancer, what kind of treatment would they give, chemo . . . radiation treatment or operate? (P10)
In the 6-month follow-up (N = 11) interviews, multiple participants commented that the decision-counseling program “made me think,” and spurred some participants from intention to action; In the words of one participant “I realized it’s that time now to stop thinking and talking about it and just do it,” (P6BL). “I already made up my mind but then on the uhm helped me to uh keep my decision.” Women were mixed on the navigation experience. For example, one participant found the experience, was definitely great. Anything that was gonna keep me focused on what I needed to do, I mean like I—I don’t mind people tracking me down if that’s what they wanna do . . . I mean, they try to find you and they can’t find you. ‘Cause now you wanna be found now. (P0127)
However, some women found they did not need that level of support, I’d rather the people help the people that don’t know. Then you waste your time with someone that do know . . . ‘Cause I talk to a lot of women here and some of ‘um are just dumbfounded and they need to have people like her. I—I’m on top of myself. (P07)
Discussion
The purpose of this study was to examine the outcomes, feasibility, and acceptability of a mammography decision support and navigation intervention women with SMI living in supportive housing settings. We partially confirmed our primary hypotheses. While there were no significant changes in knowledge, attitudes, or intention to screen (likely because of high baseline levels of knowledge and orientation toward screening), there was a statistically significant decrease in decisional conflict. The results in this population of women with SMI support previous research findings of lower decisional conflicts after decision aids were used in other populations.35,36 The uptake of mammography was 67% in this population of women with SMI who were not up to date with screening at baseline, which is encouraging. However, this is still below the 81% target rate for screening recommended by Healthy People 2020. 37 Our findings support previous research showing better health outcomes for those with a mental health diagnosis as a result of active participation in decision making. 38
We confirmed feasibility and acceptability by verifying that all the participants approached agreed to participate, and were able to complete the educational module, decision counseling session, and survey. There was an 86% study retention rate. Qualitative interviews confirmed and extended the quantitative findings by specifically providing information on the acceptability of the visual educational and SDM format and also provided concrete suggestions for improving several elements of the intervention, including the educational component and the navigation component.
While the patient navigation component was feasible, care managers were instrumental in communicating with participants who were difficult to reach by phone. The findings from this research support previous findings which have shown that patient navigation and telephone interventions are feasible interventions for mammograms.39,40 However, research in vulnerable populations have noted difficulty with phone communication, 33 and have reported on the importance of community outreach and home visits. 41 The process and outcome measures support the constructs of the PHM in that the intervention supported (1) increased access to and coordination of screening, (2) decreased decisional conflict, and (3) increased uptake of mammography screening.
The generalizability of the results is limited by the small sample size and specific population. Our study was not designed to explore a causal relationship between the intervention and the increase in mammography screening. This study was part of a larger community-based participatory research project that gained insight from women in the community throughout the process.
This study evaluated a novel intervention developed with the input of a population often excluded from research. Findings from this study are a valuable contribution to the scientific literature as previous community-based research identified low mammography screening rates in this population.10,11 The project provides specific information on how limited resources could be utilized to improve health outcomes at supportive housing agencies through the use of population specific education, SDM, and tailored navigation. Recommendations to improve this intervention include further education of the onsite supportive housing care managers and peer support staff about mammography planning and scheduling and closer, going communication between the medical staff and the supportive housing staff to enhance the efficiency of the intervention. Next steps include a randomized controlled trial of an improved and modified decision support intervention in a community mental health center setting. A key additional planned innovation is to trained peer specialists to serve as decision counselors and navigators.
Footnotes
Acknowledgements
The authors gratefully acknowledge the support and mentoring of Richard Wender, MD, Chief Cancer Control Officer of the American Cancer Society.
Authors’ Note
The research presented in this article is that of the authors and does not reflect the official policy of the American Cancer Society.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by a Cancer Control Career Development Award 123369-CCCDA-12-213-01-CCCDA from the American Cancer Society (PI: L. Weinstein). Publication made possible in part by support from the Thomas Jefferson University + Philadelphia University Open Access Fund.