
Abstract
Introduction
The Centers for Medicare & Medicaid skilled nursing facility (SNF) 3-day waiver permits patients attributed to an Accountable Care Organization (ACO) to be admitted to an SNF or transitional care unit from an emergency department, outpatient setting, inpatient stay (<3 days), or observational status without Medicare’s requisite 3-day inpatient stay.
Methods
Our institution’s ACO implemented the waiver program in 2023. We report our experience with implementing the waiver and describe benefits and barriers, as well as interventions developed, outcomes achieved, and opportunities presented for patients and health care facilities.
Results
Through a streamlined process, patients can more readily access essential care, and health care facilities benefit from enhanced efficiency. Furthermore, the ACO can more effectively manage health care utilization and cost. Although the program offers benefits to patients, their families, and health care facilities, implementing and maintaining the program has challenges, with barriers including underdeveloped workflows, gaps in staff education and communication, difficulties in patient identification, and challenges with specific facility requirements.
Conclusions
The SNF 3-day rule waiver has been valuable in enhancing patient care and optimizing health care delivery within our ACO. Ongoing efforts to refine processes and address challenges will further improve the program’s effectiveness and sustainability.
Introduction
The Medicare Shared Savings Program (MSSP) offers the opportunity to create an Accountable Care Organization (ACO). The MSSP has different participation options that allow ACOs to select arrangements that could be helpful for their beneficiaries and their organization. Medicare assesses the quality performance of participating ACOs in the categories of preventive health, care coordination and safety, and care for at-risk populations. 1
The long-standing Centers for Medicare & Medicaid Services (CMS) skilled nursing facility (SNF) 3-day rule requires patients to have a qualifying inpatient hospital stay for at least 3 consecutive days before Medicare will cover the cost for their identified skilled nursing or rehabilitation admission. ACOs can apply for an SNF 3-day rule waiver and partner with SNFs to allow for direct admission to an SNF without meeting the required 3-day rule. The SNF 3-day rule waiver applies only to patients attributed to the ACO who are admitted to an SNF affiliate of the ACO.
1
Patients can access skilled nursing care directly from the outpatient setting, the emergency department (ED), hospital observation status, or an inpatient stay of less than 3 days (Figure 1). The 3-day waiver effectively supports patient outcomes by expediting access to SNFs and reducing unnecessary hospital stays. Pathways to admission for patients attributed to an accountable care organization (ACO)
Our institution’s ACO implemented the SNF 3-day rule waiver program. Here, we report our experience with respect to the waiver’s benefits, challenges, and compliance requirements, as well as the interventions developed, outcomes achieved, and opportunities presented for both patients and health care facilities.
Methods
Study Design
Initial communications from our institution’s ACO to our 61 SNF affiliates regarding the implementation of the SNF 3-day waiver program commenced on December 5, 2023. Our ACO have about 65,000 lives across the upper Midwest with some members living across the United States. In February 2025, a retrospective analysis was conducted to assess our experiences throughout calendar year 2023 and 2024, including insights gained during the process and the resulting outcomes. Patients were classified according to where they accessed SNF care (ie, ED, inpatient stay <3 days, observational status, or outpatient in a bed). We quantified the number of patients attributed to our institution’s ACO who used the SNF 3-day waiver, as well as the number of waiver discharges by health care region and patient classification. The most frequent causes of patient admission to an SNF or transitional care unit (TCU) were analyzed. A TCU is a short-term, hospital-based unit for recovery, while a SNF is a separate residential setting that provides longer-term care. Interventions, described in this article, were implemented before and during the launch of the waiver program. The benefits and barriers encountered are reported.
Key Considerations in Waiver Program Implementation
Leadership
Organizational leadership supporting the ACO SNF 3 day waiver initiative is comprised of a variety practice leaders in related fields. This leadership team is comprised of a board of medical providers and administrators who oversee all aspects of ACO directed care. A broader multidisciplinary workgroup directly supports the practice and utilization of the SNF 3 Day Waiver. This workgroup includes medical providers, care management leadership, administrative and IT support. Staff from multiple hospital sites were involved with the initial implementation of this process and continue to monitor for successful utilization of the resource by staff involved in discharge planning. Furthermore, IT support has been vital to ensure staff can easily identify ACO eligible patients and locate participating facilities. The ACO team is also responsible for ensuring all involved staff are educated to this resource, new workflows integrate seamlessly into current practices and monitoring for appropriate staff utilization.
Compliance
Only eligible ACOs participating in certain MSSP performance-based risk tracks can apply for the SNF 3-day wavier. This includes those participating in a 2-sided risk model and those who apply during the annual application process.1,2 Since performance year 2017, the CMS has allowed a waiver for the requirement outlined in section 1861(i) of the Social Security Act, which mandates a 3-day inpatient hospital stay before a Medicare-covered posthospital extended care service. The waiver applies to eligible beneficiaries assigned to ACOs participating in a 2-sided risk model and allows them to receive covered posthospital extended care services from an eligible SNF that has a written agreement with the ACO for purposes of the waiver. Eligible SNFs include those operating under TCU bed agreements. 2
When applying for the 3-day waiver, the ACO must attest that it has developed an implementation plan that includes the following: • A communication plan between the ACO and its SNF affiliates • A care management plan for beneficiaries • A beneficiary evaluation • An admission plan
To qualify for SNF services under the waiver, beneficiaries must be attributed to the ACO, not currently reside in an SNF or other long-term care facility, be medically stable without the need for inpatient care, have certain and confirmed diagnoses, and require skilled nursing or rehabilitation services that cannot be provided on an outpatient basis. 2
To participate in the waiver as an SNF affiliate to the ACO, an SNF must maintain a minimum rating of 3 stars on the CMS 5-star Quality Rating System and enter into a CMS-compliant SNF affiliate agreement with the ACO. 2 A thorough understanding of the Medicare SNF 3-day waiver rules and ongoing oversight of its application are essential because CMS could hold an ACO accountable for noncompliance or improper use of the waiver.
Patient Identification
Patients who are traditional Medicare beneficiaries are attributed by CMS to ACOs on the basis of plurality of care, which is determined in multiple steps and is generally based on the amount of Medicare-allowed charges for services received from primary care teams. Typically, MSSP ACOs receive their attributed beneficiaries file from CMS in late December for the upcoming year. Then, in January, the ACO receives membership files from Medicare Advantage Plan (MAP) partners. If a patient attributed to an MSSP ACO transitions from traditional Medicare to an MAP, CMS does not report this change to the ACO until the first-quarter roster is provided in March. This is an important factor to consider because the beneficiaries who enroll in an MAP are no longer eligible for attribution to the MSSP ACO.
For patients who have transitioned to an MAP, the SNF 3-day waiver provides a 90-day grace period for covered SNF services, which allows the ACO time to receive the updated rosters from CMS and MAP. The ACO is responsible for verifying the patient’s insurance before admission to an SNF affiliate, which can be difficult during the period between receiving the MSSP ACO attribution list and receiving the new MAP membership lists. Operationalizing a reliable feedback system between the ACO and SNF affiliate is critical to confirm patient eligibility and improve workflows.
Skilled Nursing Facilities
As mentioned previously, SNF affiliates must maintain a CMS rating of 3 stars or more to be eligible to participate in the ACO SNF 3-day waiver program. Medicare periodically monitors the star rating of SNF affiliates and updates the ACO Management System. SNF affiliates may fluctuate in their star rating throughout the year and can continue to admit ACO waiver patients if they remain listed as an eligible affiliate. Reviewing SNF star ratings and notifying SNF leadership if their site is falling below a 3-star rating is important throughout the year and is critical in October and November when end-of-year eligibility is finalized for the subsequent year. Upon a final disposition date, SNF affiliates that have not maintained a 3-star rating or greater are terminated from the approved affiliate listing and are immediately unable to admit patients under the SNF waiver program. When an SNF affiliate is terminated from waiver program participation, patient care can be affected, necessitating clear communication with referring and SNF staff and potentially requiring modifications to electronic health record (EHR) systems.
During the ACO affiliate disposition process, CMS reviews existing and newly applying SNF affiliates for their CMS star ratings and verifies matching of their tax identification numbers and CMS certification numbers through the Medicare Provider Enrollment, Chain, and Ownership System (PECOS). A mismatch will prompt a follow-up task on the ACO Management System dashboard, which requires timely resolution through collaborative efforts between ACO and SNF representatives. A mismatch may also alert an ACO that the affiliate has changed ownership recently, which terminates the SNF as an ACO affiliate under the existing agreement. The next spring, during the Medicare annual application cycle that typically opens in May and closes in August, the SNF may reapply to become an SNF affiliate with the ACO. In these cases, a new SNF affiliate agreement must be completed between the ACO and the SNF’s new owner.
Interventions
Data Analytics and Dashboards
Several dashboards and scorecards have been developed by our ACO team to monitor waiver utilization, quality of care, and outcomes of ACO patients. Other important factors to monitor include attribution and admission status, the origin source of admission to the facility, length of stay in the SNF or TCU, costs incurred, and ED utilization and readmissions during and after the stay.
Developing and monitoring a dashboard that tracks patients eligible for discharge under the SNF ACO 3-day waiver—and whether the waiver was used—helps ensure effective oversight. One of our ACO dashboards reports waiver discharges by site and location such as inpatient, ED, and outpatient settings. This information highlights comparisons between sites and identifies areas where greater awareness and ongoing education about the waiver option may be beneficial, particularly in the outpatient setting.
Education and Communication
In preparation for the implementation of the ACO SNF 3-day waiver program at our institution, staff responsible for discharge planning were offered education. Leadership provided information about the history of the ACO program and the positive effect of the waiver on patients. Communication was designed to ensure staff could easily identify which patients qualified for the SNF 3-day waiver and included resource materials, an EHR phrase for documentation, and process workflows.
During the launch of the waiver program, staff received regular reminders about the qualifying criteria and the list of participating affiliate facilities. Because this program marked a departure from the long-standing regulation requiring a 3-day qualifying hospital stay for skilled nursing coverage, social work and registered nurse case manager leaders provided daily support, reinforcing the benefits of the ACO SNF waiver and assisting with discharge planning.
Leaders engaged in the ACO program monitored patients attributed to the ACO to ensure each one met SNF 3-day waiver requirements for skilled nursing placement. Hospital data were reviewed regularly to ensure that qualifying patients benefitted from the waiver program. Ongoing monitoring led to team member discussions of ways to optimize workflows, fine-tune messaging, and educate staff members.
In addition, the ACO team established quarterly meetings with SNF affiliates, which improved communication regarding care transitions and benefitted all involved.
Workflow Implementation and Pathways
Before creating workflows, the team met with stakeholders, reviewed existing processes, and incorporated ACO requirements to create and update the team’s workflow. Workflows were developed for the ED, hospital, and outpatient settings and were designed to educate staff, streamline processes, clarify steps, reduce errors, and improve compliance.
Before the SNF 3-day waiver program was implemented, no covered benefit existed for patients to be admitted to an SNF from the outpatient setting without a qualifying 3-day hospital stay. Therefore, the team refined the workflow for sending referrals to eligible SNF facilities from an ambulatory provider. This new outpatient process for SNF referrals was initially problematic and required continuous improvement. Opportunities for improvement included initiating an outpatient referral process, assigning resource roles to navigate SNF admissions, developing a facility order set, completing outpatient assessments, and standardizing admission paperwork.
Results
Classification of Patients Attributed to Our Institution’s ACO Who Used the Waiver in 2024 (N=272)
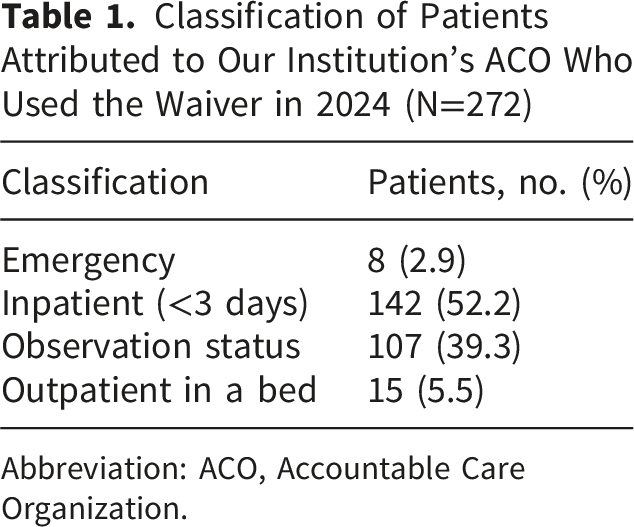
Abbreviation: ACO, Accountable Care Organization.
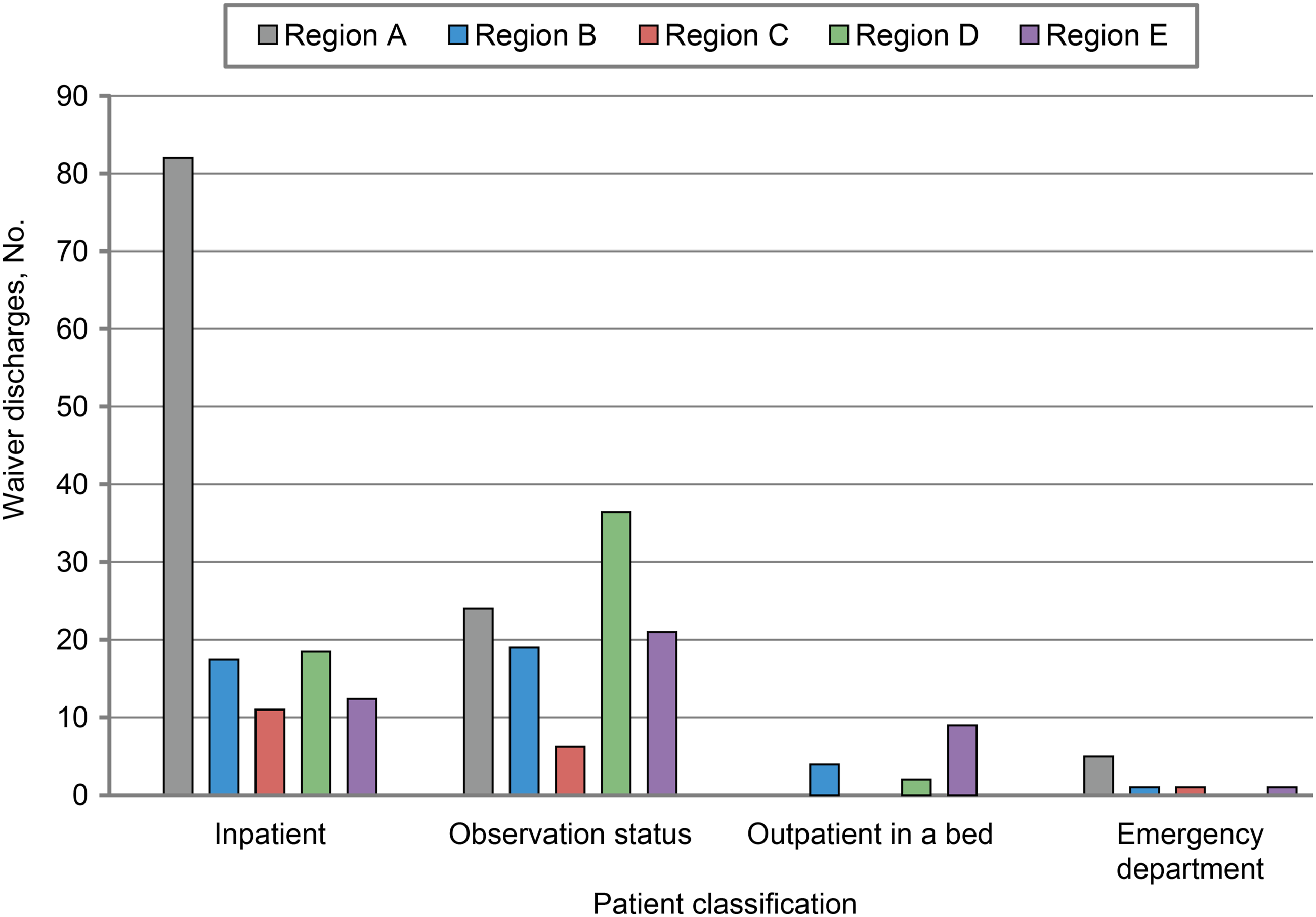
Waiver discharges by health care region and patient classification
Discussion
Benefits
The implementation of an SNF 3-day waiver program benefits patients, hospitals, SNFs or TCUs, and the ACO, although the extent of the effect is difficult to precisely quantify and may vary. Earlier access to an SNF can preserve patients’ independence and mobility and facilitate a successful return home. Avoiding an unnecessary or prolonged hospital stay saves the patient money and mitigates the risks associated with hospitalization. Without the 3-day waiver in place, nonqualifying patients may have to bear the cost of SNF charges themselves. Additionally, the waiver program positively affects a patient’s overall experience, allowing them to proceed to the least restrictive environment for care sooner than what was previously covered.
From the hospitals’ perspective, particularly those with high occupancy and census management issues, avoiding hospitalization or reducing length of stay is valuable. According to external research, the national average cost per inpatient day is $3,025. 3 However, this figure may be an overestimation, given that patients awaiting skilled nursing care are typically more stable for discharge and no longer undergoing costly interventions and imaging at this stage of their hospital stay. 3 In addition, during periods when many facilities are boarding patients in the ED or are facing delays in surgical scheduling due to bed availability, the benefit of the 3-day waiver is magnified. We showed that implementing the waiver reduced hospital bed days per patient, allowing more critically ill patients to occupy those beds while avoiding nonvalue-added bed days. The number of bed days can vary widely. Patients may leave 1 day early after an inpatient stay, whereas others may have a prolonged observation stay admission that lasts a week or longer, with no funding for an SNF stay and no availability for an alternative caregiver. Patients identified for SNF admission by the ED or outpatient clinic avoid a hospital bed all together. Our ACO has used a conservative average of 3 days for each use of the waiver as a rule of thumb for calculations. In addition to saving money, avoiding prolonged or unnecessary hospital stays can positively affect qualityand safety.
From the ACO standpoint, use of the SNF 3-day wavier can decrease overall costs and risk of readmissions and avoid unnecessary hospitalization and ED visits. For a 2-sided risk organization, the financial implications of avoiding unnecessary inpatient stays are substantial. A 3-day waiver program benefits the ACO by serving as a tool to decrease costs associated with expensive inpatient stays while balancing against the cost of increased SNF utilization. Additionally, the 3-day waiver program may improve relations with SNFs, leading to better patient outcomes.
The most frequent causes of patient admission to an SNF or TCU were related to restorative rehab, intravenous therapy, and orthopedic diagnoses. In comparison, a study of the outcomes and trends in SNF 3-day waiver use from 2014 to 2019 4 showed that the top reasons for waiver use were injuries with falls and musculoskeletal and circulatory conditions. We found that the population of patients who used a waiver had lower medical acuity, as indicated by lower diagnosis-related group weights (1.28 for patients admitted by using the 3-day waiver vs 1.68 for patients who did not use a waiver). In addition, readmissions were lower among waiver users (10.5% vs 11.8%, respectively). Based on an average 3-day stay in 2024, the use of the waiver for 272 SNF admissions resulted in approximately 816 bed days saved for our ACO. In some cases, there might have been extended stays in the ED with no transition to a SNF, however, as admission to SNFs required the Medicare mandatory 3-day inpatient stay, the previous process was to admit the patient for 3 days to meet the eligibility criteria, and therefore, a good proxy for days saved.
Barriers
Throughout the process of SNF 3-day waiver implementation, several hurdles were addressed, although some remain a challenge. The most significant ongoing challenge was the identification of patients who are attributed to the ACO and qualify for the SNF 3-day waiver. Creating an EHR indicator for patients attributed to the ACO and training care team members to look for the indicator addressed most of the identification concerns. Ongoing issues include timely updates from CMS and MAP reporting for patients who were attributed or removed from attribution to the ACO. The CMS quarterly electronic files are uploaded to the EHR and trigger the ACO indicator. Occasionally, manual review is required to confirm a patient’s eligibility for the SNF waiver and attribution to the ACO. Direct communication with other ACOs may be necessary to confirm their participation in the 3-day waiver program and affiliated SNFs. Limited access to their information, especially on nights and weekends, creates transition-of-care delays.
Another ongoing challenge is maintaining eligible SNFs. Maintaining a selection of ACO SNF affiliates across a broad service area is important for identifying a facility that is both desirable and convenient for the patient and their family. If an SNF becomes ineligible during a calendar year, the SNF may not be able to maintain affiliate status for the current or upcoming performance year. They would have to reapply the next spring, which results in a participation gap of more than 1 year.
Traditionally, for SNF care to be covered by Medicare, patients are admitted to an SNF after a required 3-day inpatient stay. However, outpatient workflows were not readily available, and the process to admit a patient to an SNF was unfamiliar to clinic care teams and staff. The team worked to identify and manage new workflows to accommodate SNF 3-day waiver admissions directly from the outpatient setting, but implementation has been slow, resulting in minimal admissions through these locations. Barriers included limited social work resources and lack of necessary orders for SNF admission. Initially, patients were boarded in the ED while waiting for SNF admission. However, this process is now being streamlined through an automated outpatient workflow.
Barriers to Success
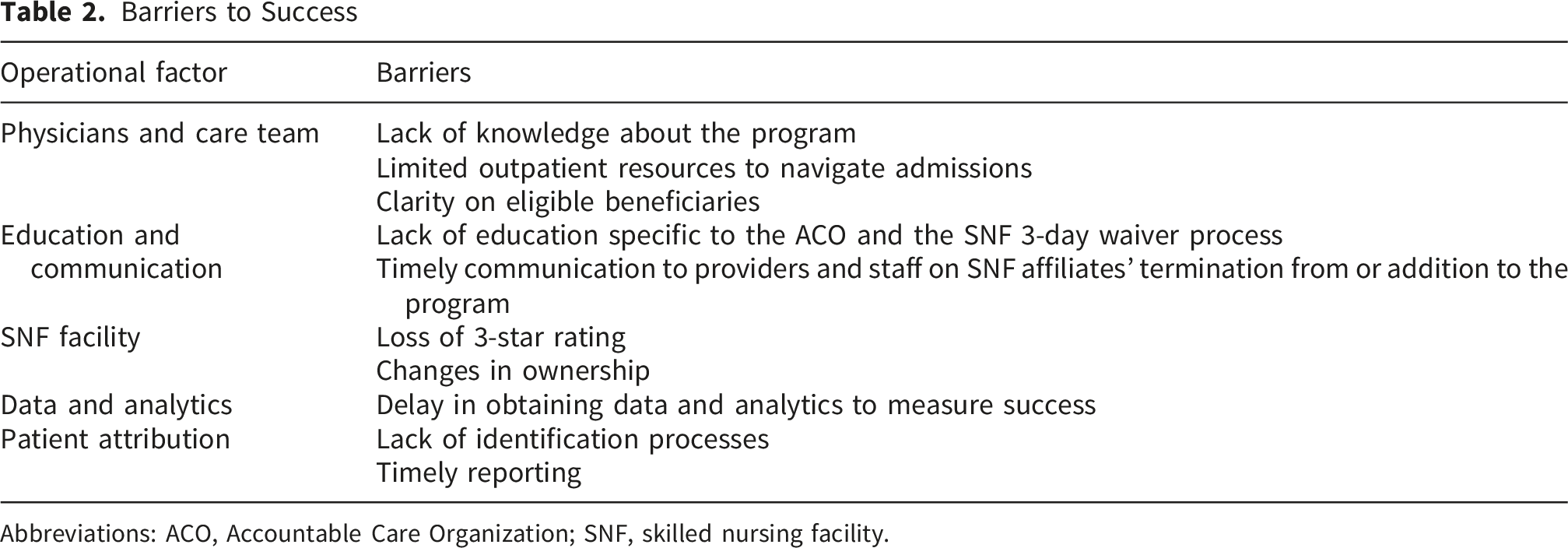
Abbreviations: ACO, Accountable Care Organization; SNF, skilled nursing facility.
Conclusion
The implementation of the 3-day SNF waiver within our ACO has shown substantial benefits for patients, their family members, hospitals, SNFs, and the ACO itself. By allowing direct admission to SNFs without the Medicare mandatory 3-day inpatient stay, patients can access necessary care more efficiently, resulting in the reduction of unnecessary hospital stays and associated costs as well as, unnecessary extended stays in the ED. This initiative has improved patient outcomes, facilitated better utilization of hospital resources, and strengthened partnerships with SNF affiliates.
Despite the numerous advantages of the 3-day waiver program, several challenges remain regarding the identification of attributed patients, compliance with CMS regulations, and maintaining a network of eligible SNF affiliates. Continuing education, workflow development, and ongoing monitoring are essential to overcoming these barriers and ensuring the program’s success.
Overall, the 3-day SNF waiver has proven to be a valuable tool in enhancing patient care and optimizing health care delivery within our ACO. Ongoing efforts to refine processes and address challenges will further improve the program’s effectiveness and sustainability.
Footnotes
Acknowledgment
The Scientific Publications staff at Mayo Clinic provided editorial consultation, proofreading, and administrative and clerical support. AI was used to assist in generating the cover letter for submission. Microsoft Copilot was used in the Education and Communication section of the main text to summarize information sent to staff. AI-generated material was reviewed and rewritten.
Author Contributions
Introduction: J.S.N.
Methods, Study Design: L.J.B.
Example of Waiver Application: J.S.N.
Key Considerations in Waiver Program Implementation, Compliance: A.R.H.T.
Patient Identification: L.J.B.
Skilled Nursing Facilities: L.J.B.
Interventions, Data Analytics and Dashboards: J.W.M., G.J.S.
Education and Communication: L.Y.L., T.J.M.
Workflow Implementation and Pathways: L.J.B., T.J.M.
Results: J.S.N., J.W.M.
Discussion, Benefits: K.S.J.
Barriers: K.S.J., V.L.A.
Conclusion: K.A.M.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All relevant data supporting the findings of this study are reported within the article or are available from the corresponding author upon reasonable request.