
Abstract
Introduction
Diet quality in the United States remains poor and contributes to chronic disease. Food is medicine (FIM) interventions integrate healthy foods into health care to manage or treat diet-related illness. Although evidence supports the nutrition–health link, less is known about how to implement FIM programs effectively in real-world settings or how to design FIM research across complex delivery systems. Guided by the Exploration, Preparation, Implementation, and Sustainment (EPIS) framework, this qualitative study examines early implementation experiences from the American Heart Association’s Health Care by Food™ (HCXF) initiative to inform future FIM research.
Methods
We conducted five virtual focus groups with HCXF-funded FIM researchers and community-based organization (CBO) partners and interviewed one food vendor. Discussions explored lessons learned, evidence gaps, methodological improvements, implementation barriers, motivations for participation, and future research priorities. We performed thematic analysis and mapped themes to the EPIS framework.
Results
Themes spanned all EPIS phases. In Exploration, participants described a fragmented evidence base, measurement gaps, and uncertainty about payer requirements amid shifting policy. In Preparation, they emphasized earlier engagement of CBOs and vendors, limited partner research capacity, and tensions between standardization and cultural tailoring. In Implementation, unclear roles, logistical complexity, and variable capacity affected feasibility; recruitment and retention relied on trust-based engagement, and technology was helpful but constrained by access and use. In Sustainment, participants highlighted outcomes beyond clinical measures, payer-specific communication and champions, and the need for stronger national coordination to support scale and coverage.
Conclusions
Early HCXF implementation experiences suggest that advancing the FIM evidence base will require larger, more coordinated studies and clearer approaches to partnership governance, measurement, cultural adaptation, and trust-based engagement. Aligning implementation science–grounded study designs with payer needs, capturing outcomes beyond clinical endpoints, and strengthening national coordination may accelerate translation into scalable models and sustainable coverage.
Background
Diet quality in the United States remains poor. Most individuals do not meet national recommendations for fruits, vegetables, and whole grains and exceed recommended limits for sodium, saturated fat, and added sugars (per the 2020–2025 Dietary Guidelines for Americans 1 ), contributing to chronic disease burden.2,3 Food is medicine (FIM) programs seek to address diet-related chronic disease by providing healthy foods as part of health care aligned interventions, including medically tailored meals, medically tailored groceries, and produce prescriptions. 4 This approach reflects a shift from nutrition counseling alone toward incorporating food provision into clinical care and aligns with evidence linking poor diet to cardiovascular outcomes and premature mortality, 5 as well as policy attention to the costs of diet-related conditions. 6
A growing evidence base suggests that some FIM models can improve intermediate outcomes such as diet quality and nutrition security, and in some studies cardiometabolic risk markers. 5 Randomized trials in the United States remain limited in number and many important questions about intervention dose, duration, populations, and outcomes remain to be answered more systematically.
Even with this emerging evidence, the field lacks consistent guidance on how to deliver and study these interventions in routine care and community settings, where multi-partner coordination, workflow integration, staffing, and data capture shape what is feasible and how results should be interpreted for scale and coverage. FIM research has begun to examine how programs are designed and delivered in real-world settings, including FIM programs implemented through citywide systems, 7 food bank and health care partnerships, 8 Federally Qualified Health Center (FQHC) collaborations,9-11 and U.S. Department of Veterans Affairs12,13 and hospital workflows.14-17 Qualitative studies in this area describe recurring implementation issues that are directly relevant to conducting FIM research, including partner coordination,8,9,18 workflow integration,8,12,13,15,19 staffing capacity,8,9,15,18 referral and navigation processes,12,13,15 and limits in data capture8,20 needed to assess engagement and outcomes. Implementation science guidance for FIM research in health care settings is still developing, leaving feasibility, scalability, and sustainment incompletely characterized across routine practice contexts. 21
Many FIM interventions rely on coordination across health care organizations, community-based organizations (CBOs), and food vendors to deliver services and support patients, yet there is less empirical guidance on how to integrate these multi-partner models into clinical and CBO workflows, particularly in resource-constrained settings. Implementation science frameworks can support this work by specifying how contextual factors shape program delivery across phases of adoption and operation. The Exploration, Preparation, Implementation, and Sustainment (EPIS) framework offers an organizing structure to examine multilevel determinants of FIM research and implementation and to interpret variation in delivery and outcomes beyond efficacy alone. 21
In 2022, the American Heart Association launched the Health Care by Food™ (HCXF) initiative to strengthen the FIM evidence base and inform coverage decisions. As of 2026, HCXF has supported over 40 FIM research projects and planning grants, including ones focused on enrollment, engagement, and short-term behavior change. This study synthesizes early implementation experiences across the HCXF portfolio to inform the design and execution of the next phase of research as HCXF moves toward larger evaluations of clinical outcomes and cost effectiveness. 6 Because implementation conditions in multi-partner delivery systems shape who is reached, what is delivered, and how consistently outcomes can be measured across sites, identifying these determinants is critical for producing valid, interpretable, and coverage relevant evidence.
Methods
We used a qualitative design with focus groups and interviews involving three stakeholder groups engaged in FIM research: researchers, CBO representatives, and a food vendor. We used purposive sampling to recruit participants. Eligible participants were directly involved in implementing HCXF-funded projects, along with one externally funded project included at the recommendation of HCXF leadership because it was similar in scope and implementation timeframe to the HCXF portfolio. The HCXF research team distributed email invitations using program contact lists. For each HCXF project, we invited the principal investigator and key implementation partners, including the CBO partner and food vendor involved in delivery.
Data Collection
In July 2025, we conducted five virtual focus groups (90 minutes each) and one individual interview (60 minutes) via Microsoft Teams. Three focus groups included HCXF-funded researchers, two included CBO representatives, and the interview included a food vendor. Sessions were organized by stakeholder role to facilitate discussion among participants with similar responsibilities.
The discussion guide covered lessons learned, evidence gaps, opportunities to strengthen study methods, implementation barriers, and motivations for research participation. A facilitator from the HCXF team led each session with support from two co-facilitators. The co-facilitators had prior involvement in HCXF and were known to many participants, whereas the lead facilitator had limited prior interaction with them.
Participants received a $75 gift card. All participants provided informed consent. The Heartland Institutional Review Board approved the study on May 20, 2025 (project no. 052025-1205).
Data Analysis
We coded de-identified transcripts inductively to develop themes grounded in participants’ accounts. The analytic team included four members with training in qualitative research and implementation science; several had prior involvement in HCXF, which informed contextual understanding but also necessitated attention to reflexivity. To address this, team members engaged in ongoing memoing and discussion to identify potential assumptions during analysis.
An initial codebook was developed through close reading of a subset of transcripts, using an inductive coding approach to identify preliminary codes. All four team members then independently coded each transcript in Dedoose, applying the shared codebook while remaining open to the addition of new codes as they emerged from the data. The coding framework was iteratively refined through repeated review of the data, with codes added, collapsed, or clarified based on team discussion and comparison across transcripts.
The team met regularly to review coding decisions and resolve differences through discussion and consensus. Rather than calculating interrater reliability, we emphasized analytic consistency through iterative consensus building, in line with interpretative qualitative methodologies. We maintained an audit trail and analytic memos documenting coding decisions, codebook iteration (including addition, refinement, and consolidation of codes), and summaries of team discussions regarding theme development.
Following coding, we grouped related codes into broader categories and examined patterns across transcripts to develop themes that captured recurring concepts and variations in participants’ experiences. Themes were reviewed and refined through comparison with the full dataset, and attention was given to identifying both convergent and divergent perspectives.
After inductive theme development, we organized themes within the EPIS framework to support interpretation within an implementation science context. This mapping was conducted after themes were generated inductively, allowing the framework to guide interpretation rather than constrain initial analysis. Themes were grouped according to the four EPIS phases: Exploration (identifying needs and assessing fit), Preparation (building capacity, partnerships, and readiness), Implementation (addressing delivery and operational challenges), and Sustainment (maintaining, adapting, and scaling interventions). Themes were also aligned with the appropriate EPIS context layer and construct, including outer context factors (e.g., sociopolitical context, funding, leadership, and patient/client characteristics), inner context factors related to organizational and individual characteristics, bridging factors that connect systems across settings, and innovation-related characteristics influencing implementation. Any discrepancies in framework alignment were resolved through team discussions and consensus.
We assessed thematic sufficiency by monitoring the emergence of new codes and themes across transcripts; as analysis progressed, few novel concepts emerged, suggesting that additional data collection was unlikely to yield substantially new insights. Unless otherwise noted, themes were consistent across stakeholder roles, including researchers, CBO representatives, and the food vendor.
Results
Participant Characteristics
Study Participants
Exploration
Participants generally viewed the diet and health relationship as well established, but they described the FIM evidence base as dispersed across small pilot studies and narrow intervention models, which complicated decisions about adoption and scale. This fragmentation was associated with persistent uncertainty about core intervention parameters, including dose, duration, and tapering, limiting the extent to which findings could inform broader implementation or policy decisions. Across stakeholder groups, a need for larger, coordinated studies to address these unresolved intervention design questions was described.
Measurement and data infrastructure limitations were also described, including difficulty assessing changes in diet quality, tracking adherence over time, and using electronic medical record data. These constraints reduced opportunities for implementation learning and limited the evidence available to inform sustainment.
FIM research was described as a pathway to policy change, but researchers reported limited clarity on the evidence payers require. Participants indicated that study questions do not always align with coverage decision points and that shifting federal and state policy environments add uncertainty. Cost effectiveness was viewed as relevant, although many questioned whether it is sufficient on its own to support broader system change.
Preparation
CBOs and the vendor described a preference for full partnership roles rather than late-stage implementation support. They emphasized early involvement in study design, budgeting, and outcome selection and formal recognition through mechanisms such as co-investigator roles or subawards. When engaged after protocols were set, partners reported frustration, difficulty navigating academic requirements, and unclear expectations within research teams. Across stakeholder groups, collaborative problem solving was described as a source of practical, low-cost solutions that leveraged existing resources within CBOs, vendors, and other organizations.
Constraints in CBO staffing, data systems, and logistics were viewed as limiting capacity to participate in research and deliver complex interventions. Researchers and CBOs emphasized the need for investment in research readiness, particularly for smaller CBOs that were viewed as trusted community partners but had limited resources for large scale implementation. In some settings, basic infrastructure gaps such as limited access to clean water, refrigeration, or childcare shaped what could realistically be delivered. Real-world barriers sometimes limited delivery even when they were not a part of the intervention itself.
Across stakeholder groups, a persistent tension between standardization and flexibility in FIM interventions was described. Standardized protocols were viewed as supporting scalability, evaluability, and payer confidence, whereas flexibility was described as necessary to reflect cultural practices and community preferences. Cultural tailoring was considered central to intervention fit but difficult to operationalize given variation in dietary preferences and traditional food practices.
Implementation
Role clarity was described as a key implementation requirement in multi-organization FIM studies. When responsibilities and communication channels were not specified, coordination was less efficient and clients or patients expressed uncertainty about whom to contact for questions or support.
Researchers and practitioners reported strong staff engagement in FIM programs, and staff often described providing food as meaningful work. Practitioners viewed FIM as expanding their ability to address patient needs that previously lacked a programmatic response. Participants indicated that this engagement supported morale and organizational readiness and may facilitate program uptake.
Implementation barriers were identified related to food sourcing and distribution, long travel distances in rural settings, and the coordination demands of multi-organization delivery. Some questioned the long-term scalability of models such as medically tailored meals. Variation in vendor capacity and limited provider engagement were viewed as additional constraints on consistency and quality.
Recruitment and retention were characterized as difficult, and participants contrasted FIM clients with the convenience samples often used in research; one participant characterized it as an “inconvenient sample,” but one that was meaningful. Engagement was attributed primarily to trust and relationships rather than program features or technology. Advisory boards, incorporation of lived experience, and practical incentives, including cooking tools, were framed as strategies that may support participation and continued involvement.
Participants viewed technology as a potential support for efficiency and access, but described constraints related to limited digital access, low app use, and high mobility among populations facing social and economic constraints. Many indicated that in the populations they serve that direct human contact was more effective than digital approaches for establishing trust and sustaining engagement.
Sustainment
Researchers and CBOs described outcomes that extend beyond individual clinical measures, including cultural connection, social relationships, local economic activity, and environmental considerations. They also noted that benefits may accrue at the household level, yet current evaluations were viewed as rarely capturing these broader effects.
Messaging, champions, and advocacy were described as influencing coverage decisions for FIM. Several noted that evidence alone may not be persuasive to policymakers or insurers and that narrative communication can carry weight in these settings. They also noted that advocacy approaches differ by payer type and that the field still lacks a coordinated strategy for engaging insurers.
The FIM field was described as expanding but not well coordinated. Many called for stronger national leadership to set shared priorities, align research efforts, and develop tools that connect local studies to broader policy change.
Mapping FIM Implementation Themes to the EPIS Framework
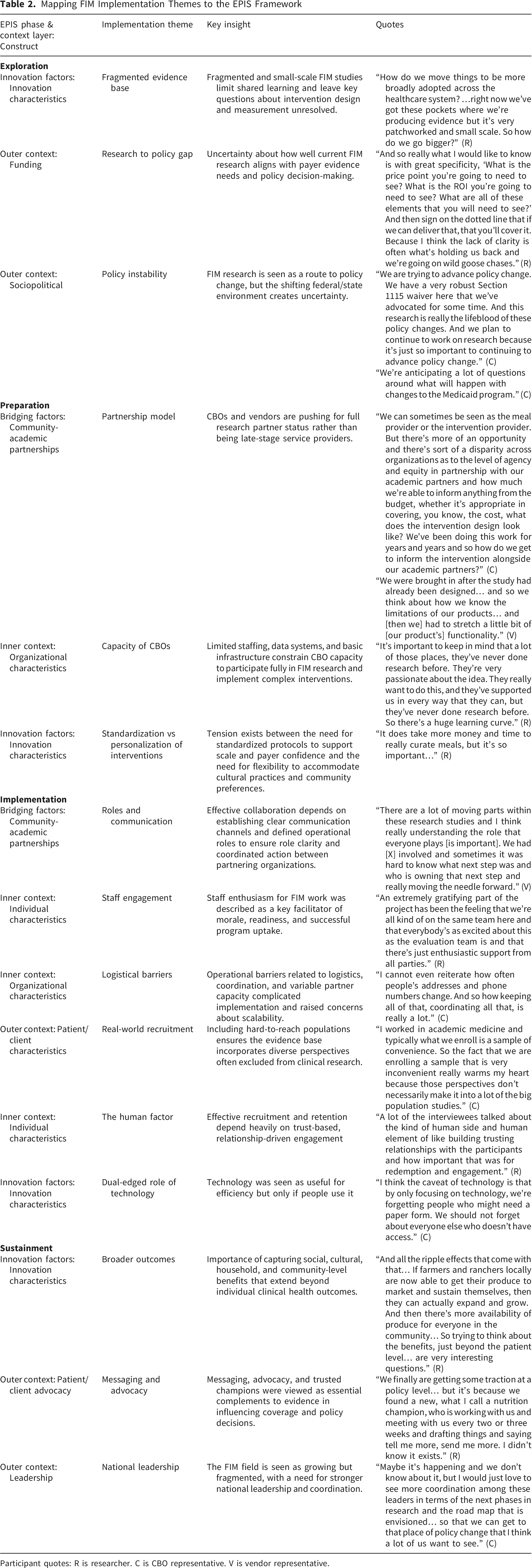
Participant quotes: R is researcher. C is CBO representative. V is vendor representative.
EPIS Framework
Figure 1 displays the study themes positioned within the EPIS phases and corresponding context layers, illustrating how determinants spanned outer context, inner context, bridging factors, and innovation characteristics. Study-informed EPIS model for FIM implementation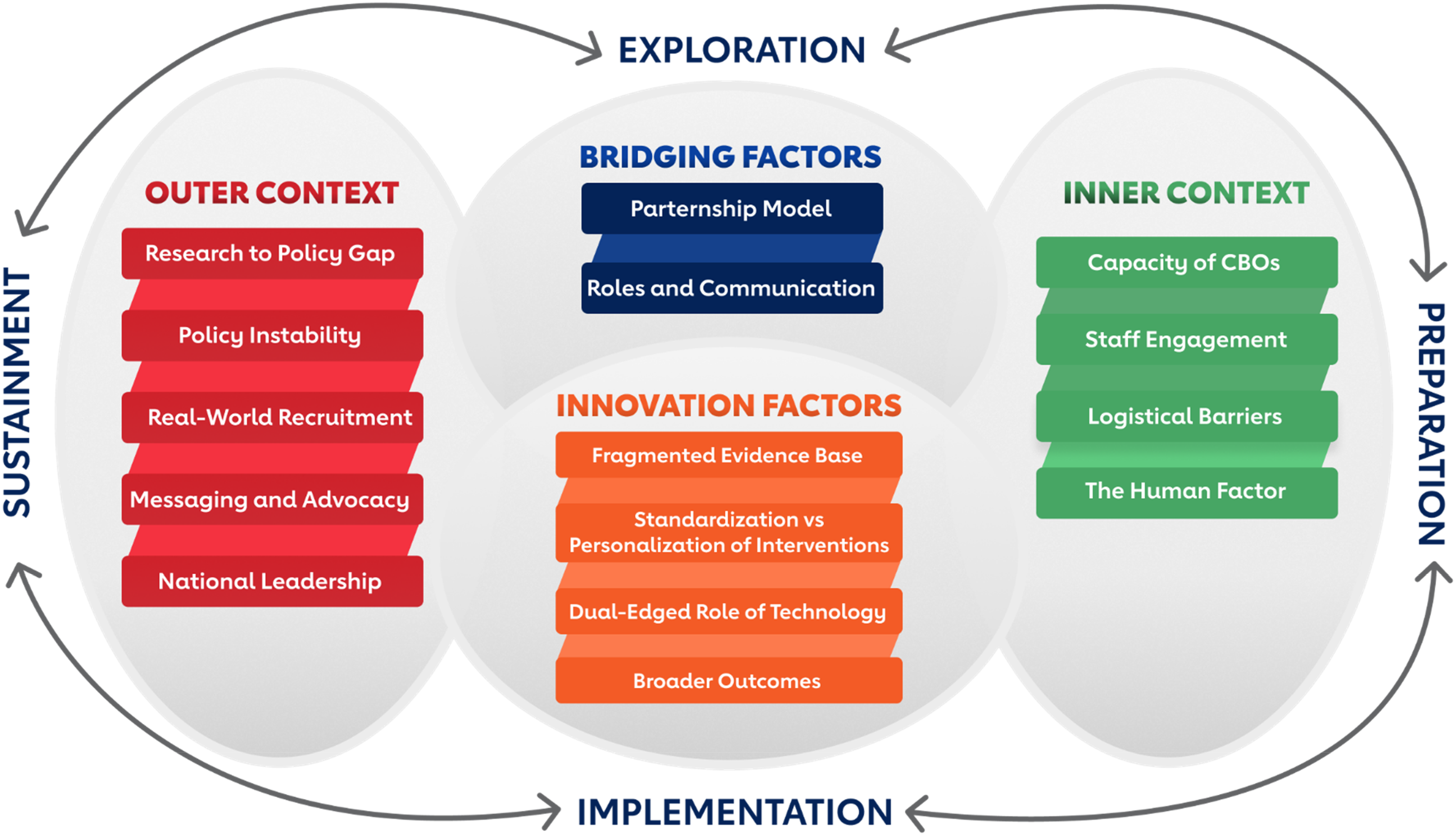
Discussion
This qualitative study applied the EPIS framework to examine implementation determinants shaping FIM research in routine delivery settings. Participants expressed optimism about FIM alongside unresolved questions about intervention parameters, measurement strategies, and the evidentiary pathway to coverage. These results support the view that implementation science can inform FIM study design by clarifying feasibility constraints, supporting partner alignment, and identifying factors likely to affect sustainment. As the body of implementation-focused studies grows, they reinforce the value of explicitly measuring feasibility, acceptability, and delivery constraints alongside clinical endpoints.13,21,22
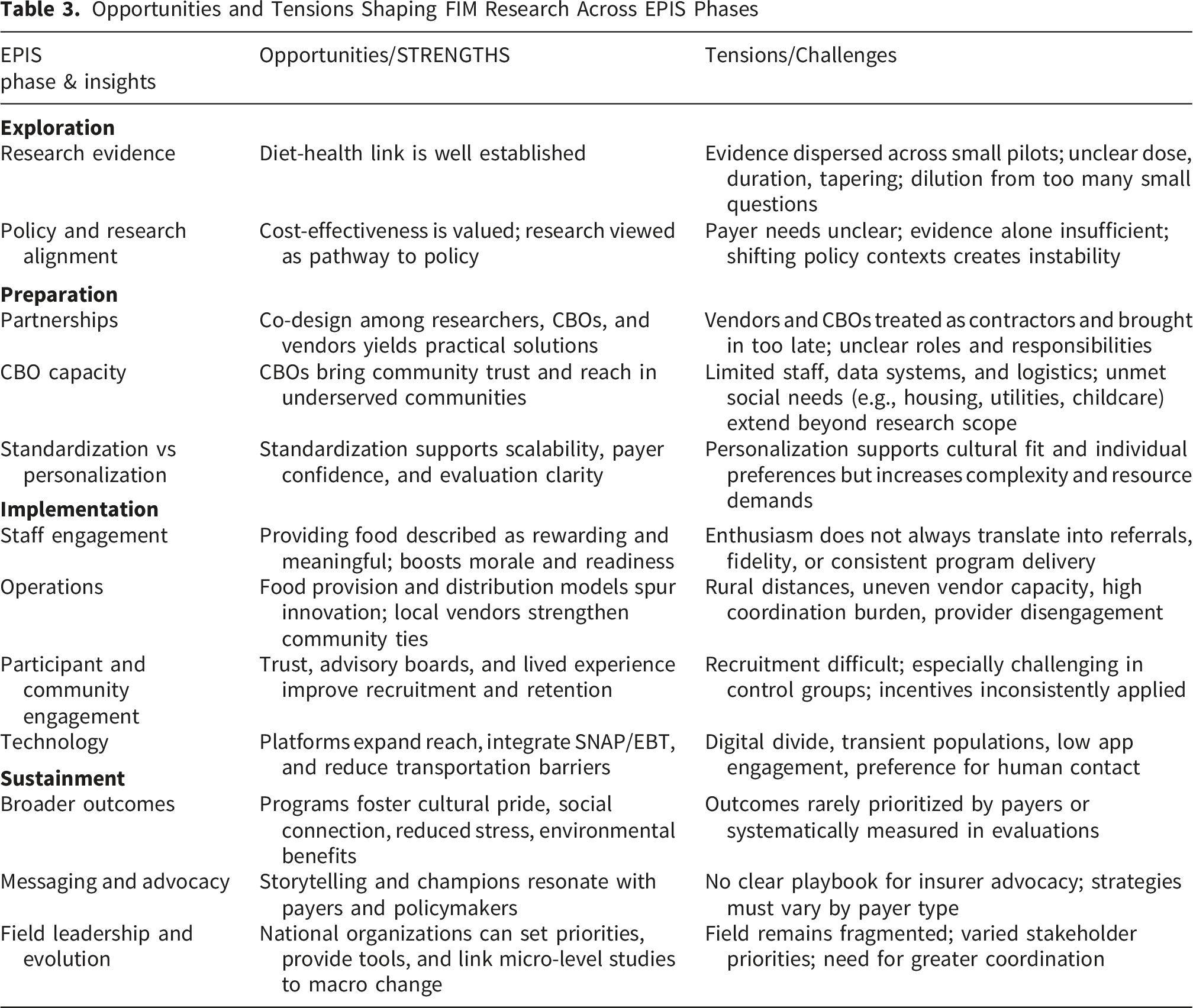
Opportunities and Tensions Shaping FIM Research Across EPIS Phases
Supporting Cumulative Learning as the Evidence Base Expands
Participants’ descriptions of an evolving and heterogenous evidence base are consistent with rapid diversification in FIM research across intervention types, settings, and delivery partners. Heterogeneity in study designs supports innovation and may be necessary while optimal intervention parameters (including dose and duration) remain uncertain. However, cross-study synthesis is limited when similar intervention intensity is described or measured inconsistently across studies, even when variation in intensity itself is expected as the field tests different models. Reviews of FIM programs in specific populations similarly conclude that variation in program components and inconsistent reporting make it difficult to compare studies, reinforcing the need for shared definitions and common metrics.20,23 These findings point to value in pairing local adaptation with greater coordination across projects, including shared definitions of core intervention components and use of a validated set of common measures, such as those developed by HCXF, 24 to support comparison and aggregation while allowing sites to tailor delivery models to context.
Stakeholders’ accounts also indicate that measurement and data infrastructure remain constraints on implementation learning. Limited capacity to assess diet quality, track adherence over time, and obtain complete follow up data from electronic records can reduce interpretability of outcome variation and obscure which implementation strategies are associated with better performance. Implementation research in food bank–health care partnerships and FQHC settings identifies persistent challenges in tracking and sharing program data and in staffing capacity, emphasizing why measurement infrastructure is foundational to implementation learning.8,10,25
Aligning Research Questions With Policy and Coverage Decisions
Participants linked FIM research to policy change and coverage expansion but acknowledged uncertainty in how evidence is weighted in coverage decisions. Policy analyses of medically tailored meals suggest that even when economic models are favorable, decision-relevant evidence often depends on whether evaluations incorporate real-world variation in program design, dose, duration, and ancillary services. 26 Future studies may benefit from specifying the decision context at the design stage, since evidence needs may differ across Medicaid programs, commercial insurers, employers, and health systems. Participants also characterized cost effectiveness as relevant but insufficient on its own, emphasizing feasibility, operational requirements, and the role of credible messengers in communicating value. Implementation studies in Medicaid pilots further indicate that reach and enrollment can be constrained by contact instability, staff time, and workflow complexity; these are practical factors that shape real-world impact irrespective of modeled cost-effectiveness. 27 Study designs that align endpoints and analyses with a defined policy use case may produce findings that are more interpretable for the intended decision maker.
Treating Partnership Design as a Research Strength
CBOs and the vendor emphasized early involvement and formal recognition as research partners. Their accounts describe co-design as improving study fit and feasibility by incorporating delivery partner expertise in community engagement, logistics, and cultural fit. Hospital-based pilots that used participatory design and iterative testing demonstrate how early partner input can improve workflow integration (e.g., referral platforms) while also clarifying delivery costs and operational requirements relevant to scalability. 15 Our findings support partnership structures that specify roles, decision authority, and communication channels at study initiation to reduce coordination burden and support consistent implementation and evaluation.
Participants also described capacity constraints among some CBOs, particularly smaller and local organizations that are often central to trust-based outreach. Across multi-partner models identified in the literature, recurring barriers include staffing capacity, partnership maintenance, and data-sharing infrastructure, suggesting that ‘research readiness’ investments are often prerequisites for stable implementation.8,9 Our findings support a role for deliberate investment in CBO research readiness, including staffing, training, and data infrastructure, to support meaningful participation and sustain multi-partner collaboration.
Advancing the Field’s Approach to Standardization and Cultural Fit
Stakeholders described tension between standardization to support scalability and payer confidence and flexibility to reflect cultural practices and community preferences. FIM studies may benefit from specifying which elements must remain consistent across sites and which elements can be adapted. Perinatal FIM implementation research similarly argues for defining core program functions while allowing structured adaptation of form, with the aim of improving interpretability across sites.20,23
Defining core intervention functions can support interpretation, while structured adaptation of form can improve cultural fit. For example, a multi-site produce prescription study could hold constant eligibility criteria, minimum dose, enrollment duration, the targeted behavior change goal, and primary outcomes with common follow-up time points. Sites could adapt delivery modalities and food options to local context and document what was changed and why, allowing subsequent assessment of whether specific adaptations are associated with engagement, retention, or diet quality across settings.
Designing for Real World Feasibility and Sustained Engagement
Participants described a gap between pilot level evidence and the real-world implementation conditions needed for long-term operation in community settings. Many of the factors that later affected implementation were identified early, during Exploration and Preparation, and participants reported that these determinants carried forward into later phases. Consistent with this, other multi-clinic FIM initiatives show that structured pre-implementation planning can substantially refine target populations and intervention specifications before delivery begins. 11 As study designs progress to embed in clinical workflows, lessons learned from involving vendors have substantial applicability to partnerships with clinical teams. Involving their perspectives early and having them as substantive partners in the research design will be critical in bridging the gaps between research and clinical implementation.
As the evidence base expands, studies should more directly address the operational demands of multi-partner FIM program delivery to support comparability and coverage decisions. Participants highlighted challenges including rural travel distances, variable vendor capacity, and coordination workload, consistent with prior studies emphasizing the importance of partner networks and infrastructure for reliable delivery and scale.7,28 Future studies may benefit from assessing feasibility, partner workload, and operational requirements alongside effectiveness. Recruitment and retention were also described as dependent on trust-based engagement, with advisory boards, lived experience input, and practical supports functioning as core implementation strategies; consistent with prior work, engagement was facilitated by ongoing communication and navigation supports, while logistical and financial barriers persisted.18,29 Participants also viewed technology as potentially improving efficiency and access, though feasibility was limited by digital access, low uptake, and population mobility, suggesting that digital tools are most effective when offered as optional supports alongside low-technology alternatives and direct human contact, particularly for participants with unstable contact information or limited device access, reinforcing the need for flexible, mixed-mode engagement approaches.27,30
Broadening the Definition of Value to Support Sustainment
Stakeholders described outcomes beyond individual clinical measures, including household level benefits, social connection, cultural meaning, and community economic effects. Long-running health system programs have demonstrated the feasibility of embedding evaluation measures beyond clinical outcomes, including patient experience, program satisfaction, and local economic effects. 14 These accounts are consistent with the view that FIM may produce impacts that are salient to participants and delivery partners even when they are not emphasized in payer decision making. Future studies may benefit from maintaining clinical and economic endpoints while also measuring broader impacts, particularly when these outcomes affect participation, partner commitment, and sustainment.
Participants also described the influence of champions, messaging, and advocacy on coverage decisions and noted that engagement approaches may differ by payer type. Research programs may benefit from specifying dissemination and translation strategies early, including identification of credible champions and tailoring messages to distinct decision maker audiences.
Limitations
This study has several limitations. Participants were drawn from HCXF-funded projects, and perspectives may not reflect experiences across the broader FIM field. Participation rates were moderate and varied by stakeholder group, which may have introduced nonresponse bias if those who participated differed systematically from those who did not. Only one food vendor participated in the study, which may limit the breadth and representativeness of perspectives captured from the vendor viewpoint. Although we used strategies to support analytic rigor, qualitative interpretation may be influenced by the research team’s perspectives. All facilitators had prior involvement with HCXF, which may have affected participant responses or discussion dynamics. Because participants were funded through HCXF, responses may have been influenced by social desirability bias, with participants potentially emphasizing favorable experiences or framing findings in ways they perceived as aligned with funder expectations. Findings are intended to provide in-depth, context specific insights rather than generalization. The study also did not include clinical partners; future work should examine how partnerships with clinical organizations shape FIM implementation and research processes.
Conclusion
Stakeholders’ accounts suggest that as FIM research expands, the central challenge is not interest or momentum, but how to generate comparable, decision-relevant evidence across diverse delivery models. Use of the EPIS framework helps identify actionable opportunities to strengthen future research, including greater cross-study coordination, clearer articulation of evidence needs and pathways to coverage, investment in partnership research infrastructure, and intervention specifications that balance evaluability with routine delivery conditions. These approaches may support an evidence base that is more consistent and decision relevant as the field moves toward larger studies of clinical outcomes and cost effectiveness.
Footnotes
Acknowledgements
The authors would like to thank the HCXF researchers, community-based organizations, and food vendor who generously shared their perspectives. We also appreciate the constructive comments from reviewers, which helped refine the framing and interpretation of our findings.
Ethical Considerations
The study was conducted in accordance with applicable ethical standards and was approved by the Heartland Institutional Review Board on May 20, 2025 (project no. 052025-1205).
Consent to Participate
Verbal informed consent was obtained from all participants prior to participation in the study. The consent process was audio-recorded.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All authors work as part of the Health Care by Food™ initiative at the American Heart Association. The Health Care by Food™ Initiative is supported by anchor funding from the Rockefeller Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The qualitative data generated and analyzed during the current study are not publicly available due to the need to protect participant confidentiality.