
Abstract
Introduction and Objectives
The incidence of heat-related illness continues to rise, disproportionately affecting older adults, marginalized racial and ethnic groups, low-income communities, and individuals with chronic medical conditions. Urban heat islands (UHIs) are urban areas with higher ambient temperatures than surrounding regions. This study aims to identify heat vulnerability factors among populations living in UHIs in Dallas, Texas.
Methods
A community-based, cross-sectional survey was conducted at three health fairs in Dallas, Texas from April to October 2025. Data was self-reported.
Results
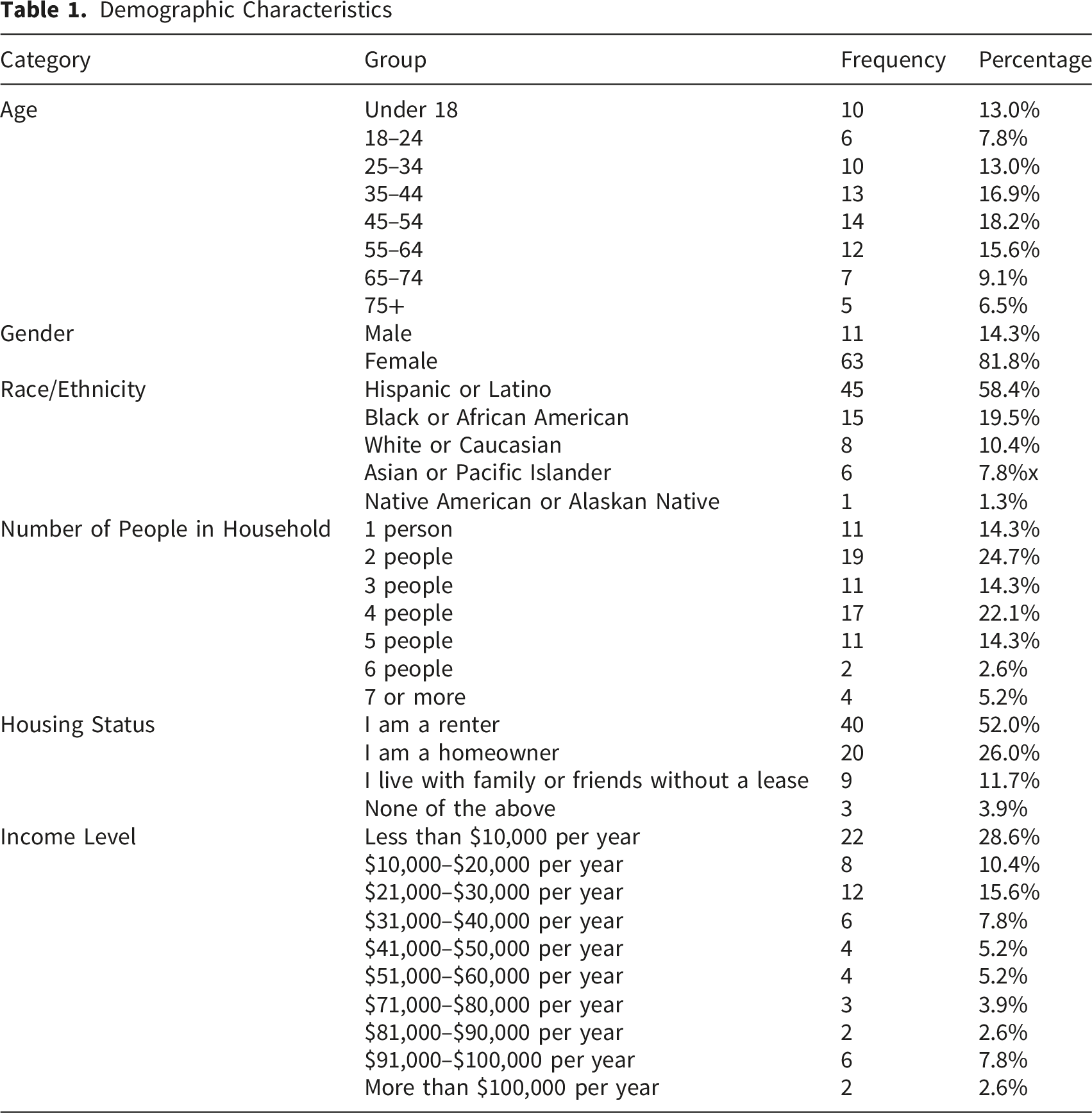
A total of 78 survey responses were collected. The sample was predominantly female (81.8%) and Hispanic/Latino (58.4%), with most participants reporting low-income status. Although most respondents had home air conditioning (93.6%), nearly half limited or avoided use due to electricity costs (47.4%). Some reported outdoor non–air-conditioned work (30.8%) or mobility limitations affecting access to cooling (12.8%). Only 42.3% knew the location of the nearest cooling center, and only 37.2% were aware of resources to help with power bills.
Conclusions
This assessment demonstrates that heat vulnerability in Dallas extends beyond environmental exposure and is driven by energy poverty, limited resource awareness, and structural inequities. Despite access to air conditioning, financial barriers and preparedness gaps constrain adequate heat responses.
Keywords
Introduction
Extreme heat events are increasing in frequency, duration, and intensity due to climate change. In 2023, global populations were exposed to an average of 50 excess days of health-endangering heat when compared to expected outcomes without climate change. 1 Heat-related deaths in adults older than 65 years old have increased by 167% since the 1990s, which is more than double than expected without climate change. 1
Beyond classic heat-related illnesses, extreme heat exposure has wide-ranging systemic health effects. 2 Heat-related illness exists along a clinical spectrum, including heat exhaustion, characterized by dehydration, electrolyte abnormalities, weakness, dizziness, and nausea, and heat stroke, a life-threatening condition defined by core body temperature ≥40°C with central nervous system dysfunction and multiorgan failure.3,4 However, heat also exacerbates chronic and acute disease processes. Cardiovascular risks increase during extreme heat events, including higher rates of acute myocardial infarction, arrhythmias, decompensated congestive heart failure, and ischemic and hemorrhagic stroke. 5 Respiratory morbidity similarly rises, with worsening asthma and chronic obstructive pulmonary disease due to airway inflammation and increased ozone and particulate matter formation.6-8 Heat exposure is associated with acute kidney injury and progression of chronic kidney disease through dehydration and renal hypoperfusion.9,10 Pregnant individuals face elevated risks of adverse outcomes, including preterm birth, stillbirth, low birth weight, and congenital anomalies such as congenital heart defects.11,12 Extreme heat also negatively affects mental health, with documented associations with increased anxiety and depressive symptoms, heightened suicidality, and increased aggressive behavior and interpersonal violence.13-18 These pathways contribute to excess all-cause and cause-specific mortality during extreme heat events. 19 Health risks are further amplified when high temperatures coincide with elevated levels of fine particulate air pollution (PM2.5), creating a dual environmental threat in which heat stress and poor air quality synergistically worsen inflammation, cardiopulmonary strain, and mortality risk.8,20
The heat-related effects of climate change on health have been found to disproportionately affect vulnerable populations such as older adults, marginalized racial and ethnic groups, low-income communities, and those with chronic medical conditions. 21 Older adults with medical comorbidities are at an especially increased risk due to impaired thermoregulation, medication side effects, and limited mobility. Disparities in populations severely affected by heat-related illnesses are driven by complex social, historical, and economic factors including discriminatory housing practices such as redlining, which have resulted in urban heat islands (UHIs) with less green spaces and higher ambient temperatures. 22
Urban heat islands are characterized by a rise in temperatures in urban areas as compared to surrounding rural and suburban areas due to human activity and infrastructure.23,24 Dallas, Texas faces significant challenges in this regard, with large populations facing extensive urban heat island effects. This is exacerbated by the geography and climate patterns of the region. In Dallas and other Southwestern U.S. cities, Hispanic/Latino neighborhoods are, on average, 2–4°F (1–2°C) hotter than wealthier or predominantly White neighborhoods during summer heat events. 25 Historically redlined neighborhoods in major Texas cities, areas that disproportionately include Black and Hispanic/Latino residents, experience higher land surface temperatures and increased rates of outpatient visits and inpatient admissions for heat-related illness.26,27 The disproportionate burden of heat-related illness and morbidity is further compounded by higher rates of outdoor employment, limited access to healthcare, and a greater prevalence of chronic conditions such as diabetes and hypertension. 22 This study aims to conduct a community-based survey to characterize heat vulnerability factors and preparedness in predominantly Hispanic/Latino and Black communities in Dallas County. Understanding these factors at the community level may help identify gaps in awareness, access to resources, and preparedness.
This study is informed by the Social Determinants of Health framework, which recognizes that environmental exposures such as extreme heat intersect with socioeconomic, housing, occupational, and structural conditions to shape health risk. 28
Methods
A community-based, cross-sectional survey was administered to evaluate heat vulnerability factors and preparedness among residents of predominantly Hispanic/Latino and Black communities in Dallas County. Participants were recruited through convenience sampling at three local community health fairs held between April and October 2025. Each booth included bilingual educational materials on heat stroke and heat exhaustion and information on nearby cooling centers and local resources. All individuals attending the health fairs and willing to complete the survey were eligible to participate. No additional exclusion criteria were applied. Surveys were offered in English and Spanish and were self-administered. The survey did not collect identifying information regarding household membership; therefore, if there were responses from individuals from the same household, they could not be identified or combined and were analyzed as independent responses. During the first of the three health fairs, mist fans were distributed at the educational booth as an incentive for attendees to engage with heat-related illness education and complete the survey. A longer survey was initially utilized at the first health fair, consisting of 29 questions. Informal participant feedback and on-site observations suggested that the survey was too long, as there were several participants who either declined to complete the survey or who did not complete the questions printed on the back page. Based on these observations, the survey was condensed to 17 questions for the subsequent 2 health fairs to improve completion rates (see Figures 1 and 2). Survey (short version) Heat survey (original long version)

The initial and condensed versions of the survey collected information across six domains: (1) demographics and annual household income; (2) housing characteristics and air-conditioning (AC) access and use; (3) employment and occupational heat exposure; (4) knowledge of resources such as cooling centers and utility assistance programs; (5) availability of social support during extreme heat events; and (6) knowledge of heat-related illness symptoms and appropriate responses. See Figure 1. All responses were self-reported and collected anonymously.
The study protocol was reviewed by the Institutional Review Board and determined to be exempt from IRB oversight under Category 2: research involving surveys, as data was recorded anonymously and posed minimal risk.
Data Analysis
Descriptive statistics were calculated using Microsoft Excel. Frequencies and percentages were used to summarize categorical variables. Incomplete or missing responses were included in the analysis when possible, and percentages were calculated using the number of respondents for each individual question as the denominator. Due to the structure of the surveys and the nature in which respondents were captured, no further analyses investigating associations relating sociodemographic and heat risks were feasible. Surveys were also not structured to collect detailed census area level data, so geospatial analyses were also not feasible for this study.
Results
Demographic Characteristics
Most participants reported having a working air-conditioning system at home (n=73, 93.6%), though nearly half limited or turned off their air-conditioning use in the summer due to concerns about power bills (n=37, 47.4%). Mobility limitations affecting the ability to seek cooling were reported by 12.8% of participants (n=10). 30.8% (n=24) worked outdoors or in indoor environments without air-conditioning. Time spent outdoors on hot days varied, with 38.5% (n=30) spending less than one hour and 32.1% (n=25) spending 1–2 hours.
Awareness of heat-related resources was limited. Only 42.3% (n=33) of participants knew the location of the nearest cooling center, and only 37.2% (n=29) were aware of resources to help with power bills.
Social support during extreme heat was reported by most participants, with 62.8% (n=49) indicating they had a neighbor, friend, or family member who could check on them during hot days.
Self-reported knowledge about heat-related illness was relatively high, with 74.4% (n=58) reporting that they are able to recognize the signs and symptoms. While still a majority of participants, slightly fewer (62.8%, n=49) reported that they knew what actions to take if they or someone they knew experienced heat-related illness.
Results

Discussion
This community-based survey highlights the complex and multilayered nature of heat vulnerability in predominantly Hispanic/Latino and Black communities in Dallas, Texas. Although nearly all participants reported having access to a working air-conditioning unit, almost half limited its use due to concerns about electricity costs. This finding suggests a disconnect between access and actual utilization and underscores the growing challenge of energy poverty, defined as the inability to afford adequate household energy services necessary for health and well-being. 29 Energy poverty poses heightened risk during extreme heat events, when the inability to cool indoor environments substantially increases the risk of heat-related illness, particularly among older adults, individuals with chronic illnesses, and low-income families. This reflects a broader pattern described in the literature: energy insecurity acts as a mediator between structural inequality and health outcomes, amplifying heat-related morbidity even when cooling technologies are technically available. 30 In other words, ownership of an air-conditioning unit alone may not fully reflect heat resilience: economic, social, and infrastructural conditions affect whether households can safely utilize cooling resources.
Despite relatively high self-perceived recognition of heat-related illness symptoms among participants, our findings reveal a meaningful gap between knowledge and preparedness. The number of respondents who reported that they could identify signs of heat-related illness surpassed those who knew what actions to take. Even fewer were aware of available cooling centers or energy assistance programs. This discrepancy highlights that awareness alone is insufficient to ensure safety during extreme heat events. Without accessible, trusted, and culturally tailored information, knowledge alone may be insufficient to ensure protective action. These gaps in resource awareness highlight a need for targeted and multilingual efforts to improve community education and resource access. These disparities in access to information and resources compound the environmental heat-related risk to vulnerable populations.
Nearly one-third of participants reported outdoor or high-heat occupational exposure, indicating that structural and occupational factors substantially contribute to total heat burden. These findings suggest a need for strengthened workplace protections, employer education, and policies that ensure safe working conditions during extreme heat, particularly for communities disproportionately represented in outdoor labor.
Although older adults comprised a smaller portion of our sample, the challenges identified in this sample, particularly limited resource awareness and electricity costs, are likely to have amplified consequences in older adults. This is due to impaired thermoregulation, mobility limitation, and higher chronic disease burden which previous literature has identified. 5
Despite these vulnerabilities, the survey findings suggest the presence of notable community strengths. A majority of participants reported having a neighbor, friend, or family member, who could check on them during periods of extreme heat. These social support networks may function to mitigate vulnerability and could be leveraged in targeted intervention strategies such as heat safety buddy systems, neighborhood check-in programs, and community-based alert networks. However, these strengths coexist with profound socioeconomic challenges. Nearly 30% of the sample reported annual household incomes under $10,000 per year, and over 50% reported annual household incomes of $30,000 or less per year, reflecting significant economic hardship. Such financial strain directly intersects with energy poverty, housing conditions, limited transportation, and reliance on high-heat occupations, collectively amplifying vulnerability.
The results of this study can be understood through the Social Determinants of Health (SDOH) framework. 28 This helps contextualize how structural factors, such as historical housing discrimination, occupational exposures, and socioeconomic disadvantage, intersect to increase vulnerability to extreme heat. 22 Additionally, SDOH examines the social conditions under which people live, and the support they are given by their communities. Many participants live in renter-occupied housing located in historically under-resourced neighborhoods shaped by redlining and disinvestment. 26 These areas often experience intensified urban heat island effects due to limited tree canopy and high concentrations of impervious surfaces. Consistent with this framework, our findings suggest that environmental exposures cannot be divorced from the social and economic systems that shape them.
Within the SDOH framework, institutional and policy-level conditions such as energy pricing, housing instability, and limited public investment may constrain individual capacity to protect against extreme heat. In this context, financial limitations, air-conditioning use, limited awareness of resources, and occupational heat exposure can be understood not only as individual-level factors, but as outcomes which stem from systemic barriers. For example, the 30.8% of participants working outdoors or in non-air-conditioned environments face occupational heat exposure that is determined by labor policies and workplace protections, conditions largely outside individual control.
Our findings also align with the growing body of literature illustrating heat inequities in Hispanic/Latino communities in the Southwestern United States, where neighborhoods are often 2–4°F hotter than predominantly White or higher-income areas. 25 As noted above, many participants reported having social support during extreme heat, which may represent an important protective factor within the community. Additionally, most participants reported knowledge regarding the signs and symptoms of heat-related illness. These community assets align with the social and community context domain of the SDOH framework, which views social cohesion, informal support systems, and shared knowledge as buffers for the impacts of climate-related stressors. 31 Leveraging these strengths, while addressing structural barriers such as energy poverty and limited access to cooling resources, may be an effective strategy for community-centered interventions.
This study has several limitations. First, the use of convenience sampling limits generalizability, as participants may not represent the broader community or other heat-vulnerable groups. Certain high-risk subgroups, including outdoor workers, older adults, and individuals with chronic illness may be under-represented in this sample. Consequently, our ability to comprehensively assess heat-vulnerability in these groups is limited.
All data was self-reported, introducing potential recall and social desirability biases that may inflate perceived knowledge or preparedness. Because the study design was cross-sectional, we cannot infer causal relationships between heat-related knowledge, resource awareness, and actual behaviors. We also did not evaluate the actual accessibility or effectiveness of resources such as cooling centers or utility assistance programs, limiting our ability to assess how well these interventions function in practice. Finally, although sessions were conducted in English and Spanish, language and cultural nuances may not have been fully captured, which could affect interpretation of themes related to risk perception and social support.
Overall, the findings suggest that improving heat resilience in vulnerable Dallas communities may require a multidimensional approach. Financial barriers to air-conditioning utilization appear to be an important contributor to heat vulnerability in this sample. Policy efforts should focus on expanding utility assistance programs and improving community awareness of these programs. Other interventions such as improving the energy efficiency of homes could also provide significant long-term benefits. Urban planning interventions such as increasing tree canopy and green space can also be used to mitigate urban heat island effects. 23 Since the population is primarily Hispanic/Latino, providing culturally tailored and multilingual health communication is critical. Finally, ensuring occupational protections for outdoor workers is an essential component of a comprehensive heat-adaptation strategy.
This study highlights that heat vulnerability in this sample appears to be shaped by far more than individual behavior; it emerges from the interaction of environmental exposures, economic constraints, and longstanding structural inequities. Addressing energy poverty and enhancing community-level resources will be critical for protecting populations disproportionately affected by extreme heat as climate change continues to intensify.
Conclusion
This community-based survey describes that heat vulnerability in this sample from Dallas appears to be driven not only by environmental exposures but also by energy poverty, limited awareness of available resources, and structural inequities. Future studies should incorporate measures that assess both perceived and actual knowledge of heat-related illness and protective behaviors. Including objective knowledge-based questions and measures of self-efficacy may help better distinguish between confidence and competence in recognizing and responding to heat-related illness and reduce the potential impact of social desirability bias in self-reported responses. Future studies should use surveys that can capture more data points to allow for more in-depth statistical analyses such as bivariate and also geospatial analyses. Future research should also focus on assessing the effectiveness, accessibility, and utilization of existing resources such as utility assistance programs, cooling centers, and workplace heat protections. Additional areas of research should include efforts to mitigate the urban heat island effect as well as identify the most effective public health education strategies for high-risk populations.
Footnotes
Acknowledgements
We would like to acknowledge the contributions of Elsa Zhang for her help with the survey development, Dr. Arthur Hong for his guidance and support, Dr. Folshade Afolabi for her guidance and support, and Isabelle Carroll for her guidance and support in this project.
Ethical Considerations
This study was reviewed by the UT Southwestern Medical Center Institutional Review Board and determined to be non-regulated (STU20250485).
Consent to Participate
Written consent was obtained from participants.
Author Contributions
Sanjna Bhatia: Conceptualization, Methodology, Formal Analysis, Investigation, Original Draft Preparation, Reviewing & Editing
Maya Garg: Conceptualization, Methodology, Formal Analysis, Investigation, Original Draft Preparation, Reviewing & Editing
Authors Maya Garg and Sanjna Bhatia contributed equally to this manuscript
Anusha Govind: Conceptualization, Methodology, Original Draft Reviewing & Editing
Michael Wu: Methodology, Data analysis, Original Draft Reviewing & Editing
Sheila Modi: Conceptualization, Methodology, Formal Analysis, Investigation, Original Draft Preparation, Reviewing & Editing
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding for the mist fans that were distributed during the first health fair was provided by Texas Physicians for Social Responsibility.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on request, and requests will be reviewed by all authors.