
Abstract
Background:
When healthcare research evidence is not used in practice, this can lead to reduced quality of life for patients and inefficient resource allocation for services. Knowledge translation (KT) aims to bridge this gap by ensuring research reaches the right users at the right time. This study focuses on evaluating KT products and dissemination strategies within the Fraser Health Authorities Virtual Health Department to improve the uptake and sustainability of evidence-informed decision-making.
Methods:
This study was conducted in 3 phases: (1) a rapid review to identify KT strategies relevant to the Virtual Health Department, (2) a survey to evaluate preferences among the Virtual Health Department, and (3) qualitative interviews to gather insights on the use and improvement of KT products. Descriptive statistics were used to summarize survey data, and thematic analysis was applied to interview transcripts.
Results:
The rapid review identified 37 relevant KT strategies. Survey results indicated a preference for practical and visually appealing KT products such as checklists, infographics, and how-to guides. Qualitative interviews highlighted barriers such as capacity constraints and content overload, but also successes in building confidence and improving work practices.
Conclusions:
Effective KT strategies are essential for integrating research into practice. The study’s findings suggest that tailored, user-friendly KT products and ongoing engagement with end-users can enhance the uptake of research evidence. Future efforts should focus on embedding KT activities into organizational workflows and improving the accessibility of KT products.
Keywords
Background
Even though a great deal of health research is produced, much of it is not used in everyday healthcare. 1 This can lead to poorer health outcomes for patients 2 and inefficient use of limited healthcare resources.1,3 To address this gap, there has been a growing interest in knowledge translation (KT). 4 KT is defined as the “dynamic and iterative process that includes the synthesis, dissemination, exchange, and ethically sound application of knowledge to improve the health of populations, provide more effective health services and products and strengthen the health care system.” 4 Put simply, KT is about getting the right information to the right people (such as clinicians, policy makers, patients, and caregivers) at the right time, and in a way that is easy for them to understand and apply. 5 KT strategies vary widely and include passive dissemination (eg, reports and newsletters), targeted products (eg, toolkits, checklists, and infographics), interactive approaches (eg, workshops, facilitation, and co-creation), and increasingly, digitally mediated dissemination strategies embedded within organizational communication platforms. Effective KT is increasingly understood not simply as information transfer, but as the extent to which knowledge is accessible, relevant, timely, and integrated into decision-making processes. Effective KT helps ensure that healthcare decisions, policies, and programs are informed by the best available evidence, 6 which can improve patient care and overall health outcomes. 7
Recent work highlights the rapid evolution of digital KT, with growing emphasis on platforms, tools, and digital dissemination channels in supporting evidence uptake. Digital KT approaches increasingly leverage technologies such as mobile health applications, interactive web platforms, and text messaging to disseminate health information and support decision-making.8,9 A recent scoping review further demonstrates that digital platforms (eg, policy dashboards, social media tools, and online knowledge repositories) are becoming central infrastructures for sharing and applying evidence across health systems. 10 Global organizations such as WHO have also highlighted the need for more systematic digital KT mechanisms. Their 2024 global research agenda identifies digital platforms and coordinated digital KT strategies as key priorities for improving evidence-informed policy-making. 11 Despite the rapid expansion of digital KT infrastructures, relatively little research has examined how KT products are actually accessed, interpreted, and used within digitally mediated healthcare work environments. In particular, there is limited empirical evidence on how virtual care teams engage with internally produced KT products and what organizational conditions influence their uptake.
This study aims to evaluate KT within the Fraser Health (FH) Virtual Health department, highlighting the effectiveness of different dissemination strategies to foster evidence-informed decision making within a dynamic healthcare environment.
Virtual health contexts present distinct KT challenges due to their rapid pace of implementation, reliance on digital platforms, frequent policy and technology changes, and interdisciplinary teams working across clinical, technical, and operational domains. Unlike traditional clinical settings, virtual health teams often make decisions in environments where evidence is evolving, workflows are digitally mediated, and communication occurs primarily through asynchronous platforms (eg, Teams, dashboards, and shared repositories). These features heighten the risk of information overload while simultaneously increasing the need for timely, actionable evidence.
Fraser Health Context
As the largest regional health authority in British Columbia, Canada, FH serves more than 2 million Canadians. 12 FH has prioritized expanding virtual care, 13 with roughly 30% of visits being conducted virtually since 2019. At the time of this study, the Virtual Health department included 2 distinct teams: one responsible for enabling the implementation of virtual health services, and another dedicated to operationalizing regional virtual services. The enablement team includes staff whose job duties include improving the translation of research into FH practice while evaluating existing Virtual Health programming. These research and evaluation focused staff members actively collaborate with patients, clinicians, staff, and other end-users with the goal of integrating evidence-based practice into patient care. This study aims to: (1) identify dissemination specific KT strategies relevant to the Virtual Health department, and (2) assess the effectiveness of current KT dissemination strategies. This study focused exclusively on internal KT among Virtual Health staff and leadership, rather than patient-facing KT. The goal of this work is to improve the translation of research and evaluation results into practice, fostering a culture of continuous learning and evidence-informed decision making across the Virtual Health department.
Methods
This study involved 3 phases: (1) rapid review; (2) survey with Virtual Health staff and leadership; and (3) qualitative interviews with virtual health staff and leadership.
Phase 1: Rapid Review
This review aimed to identify KT strategies relevant to the Virtual Health department. A rapid review was chosen for its ability to provide timely results in a more structured approach compared to literature reviews, while being more efficient than systematic reviews. 14
Identifying Relevant Studies
Medline and CINAHL were searched in December 2023 for KT related terms. Results were limited to review articles from 2008 onwards to ensure inclusion of contemporary, digitally mediated KT strategies relevant to virtual and hybrid models of care. Grey literature was searched by scanning the first 10 pages of google using the strings “KT strategies” and “research dissemination strategies.” See Supplemental Appendix A for full search strategy. To be included, sources had to name specific KT strategies. No limits were placed on context, location, or knowledge-users.
Study Screening and Selection
Title and abstract screening, followed by full text screening was completed by a single reviewer using Covidence. 14 Study selection was documented in a PRISMA flowchart (Figure 1).

PRISMA flow diagram.
Data Extraction
One reviewer independently extracted KT strategies from the included sources. Once a KT strategy was noted once, it was not extracted again.
Collating, Summarizing, and Reporting the Results
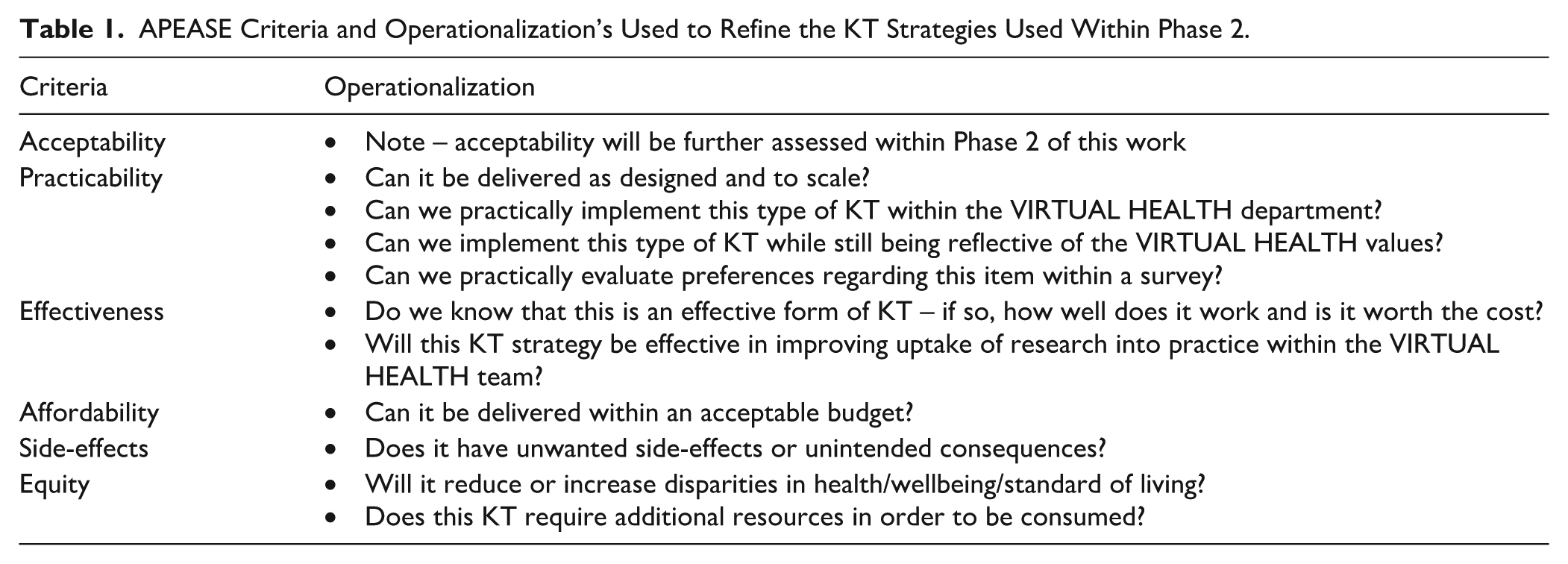
A full list of KT strategies can be found in Supplemental Appendix B. To identify strategies relevant to the Virtual Health department, each strategy was assessed using the APEASE criteria (Acceptability, Practicability, Effectiveness, Affordability, Side-Effects, and Equity). 15 Strategies not meeting all criteria were removed. See Table 1 for APEASE criteria operationalizations. KT strategies identified in Phase 1 were mapped to product types and dissemination modes, which directly informed survey item development and response options in Phase 2.
APEASE Criteria and Operationalization’s Used to Refine the KT Strategies Used Within Phase 2.
Phase 2: Survey
Phase 1 results were used to develop a survey to evaluate preferred KT strategies and modes of communication among the Virtual Health department.
Data Collection
Members of the Virtual Health department were invited to participate via email and internal communication channels on Microsoft Teams. Consenting participants completed an online survey (see Supplemental Appendix C). KT strategies (from Phase 1) were organized into 3 categories: audio/visual; written/printed materials; and training/education. Within each category, participants rated their likelihood of using specific knowledge products on a 5-point Likert scale from 1 to 5 (very unlikely to very likely). Participants were asked to check all that apply for where they would prefer to receive KT products (response options informed by Phase 1 and existing Virtual Health department dissemination channels).
Participants also evaluated 8 existing knowledge products to better understand current use of knowledge products (see Table 2). Products were selected based on recency, relevance to departmental priorities, and representation of different KT formats. Additionally, it would be infeasible to ask participants about all KT products. As such, only 8 were selected to avoid survey and cognitive fatigue. Specifically, they were asked their level of awareness for each product (response options: I am not aware of it; I am aware of it, but have not read it; I have read it, but not used it; I have actively used it in my work), and how relevant it was for their job (response options: not at all relevant; slightly relevant; moderately relevant; and highly relevant). Data was summarized with descriptive statistics.
Description of KT Products Which Were Evaluated Within the Survey.

Phase 3: Qualitative Interviews
To understand how specific knowledge products were used and to improve KT within the Virtual Health department, Phase 3 involved 30- to 60-min interviews. This portion of the manuscript follows the “Consolidated criteria for reporting qualitative studies” 32 item checklist. 16 Interviews were conducted by MM2 and MK who both had master’s degrees and worked as the “Leader, Research, Evaluation and Learning” and the “Research and KT Lead” for the Virtual Health department at the time of interviews. All interviewees had prior relationships with those conducting interviews as they worked in the same department and were told the goal of interviews was to improve KT within the department. To mitigate potential social desirability or response biases arising from these prior relationships, participants were assured of confidentiality, encouraged to provide honest and critical feedback, and interview findings were triangulated with anonymous survey data from Phase 2. While these existing relationships may have increased the risk of social desirability bias, they also facilitated contextual understanding and open discussion of operational challenges within the department.
Paradigmatic Position
Interviews were guided by a pragmatic epistemology, which seeks to generate practical findings that can be readily applied in real-world settings while also tolerating multiple truths. 17 Although all Virtual Health members were exposed to the same KT products, everyone has unique experiences.
Sampling and Data Collection
Interviews were conducted with Virtual Health department managers and directors recruited via email and Microsoft Teams. Semi-structured, one-on-one, audio-recorded interviews were conducted virtually using Microsoft Teams. Interviews explored participants experiences with specific knowledge products, and if/how they used the knowledge products in practice, and any suggestions to improve KT practices in the future. The interview guide was developed by researchers and can be found in Supplemental Appendix E.
Data Analysis
Anonymized transcripts were imported into NVivo where thematic analysis was used. All transcripts were coded by 2 authors. One coded it deductively using codes based on a pre-existing evaluation framework used within the Virtual Health department and the other coded inductively to ensure that all relevant data was captured.
Results
Phase 1: Rapid Review
A total of 75 KT strategies were identified (see Supplemental Appendix B for all strategies)18-70 split into 3 categories: what (n = 37, KT products such as videos, infographics, reports, etc.); where (n = 30, platforms or venues for dissemination such as social media, email, academic conferences, etc.); and by whom (n = 8, actors who can share KT products such as champions, peers, researchers, educators, etc.). From the 75 KT strategies, 37 were identified as potentially relevant to the Virtual Health department. For a full list of reasons KT strategies were excluded, see Supplemental Appendix D.
Phase 2: Survey
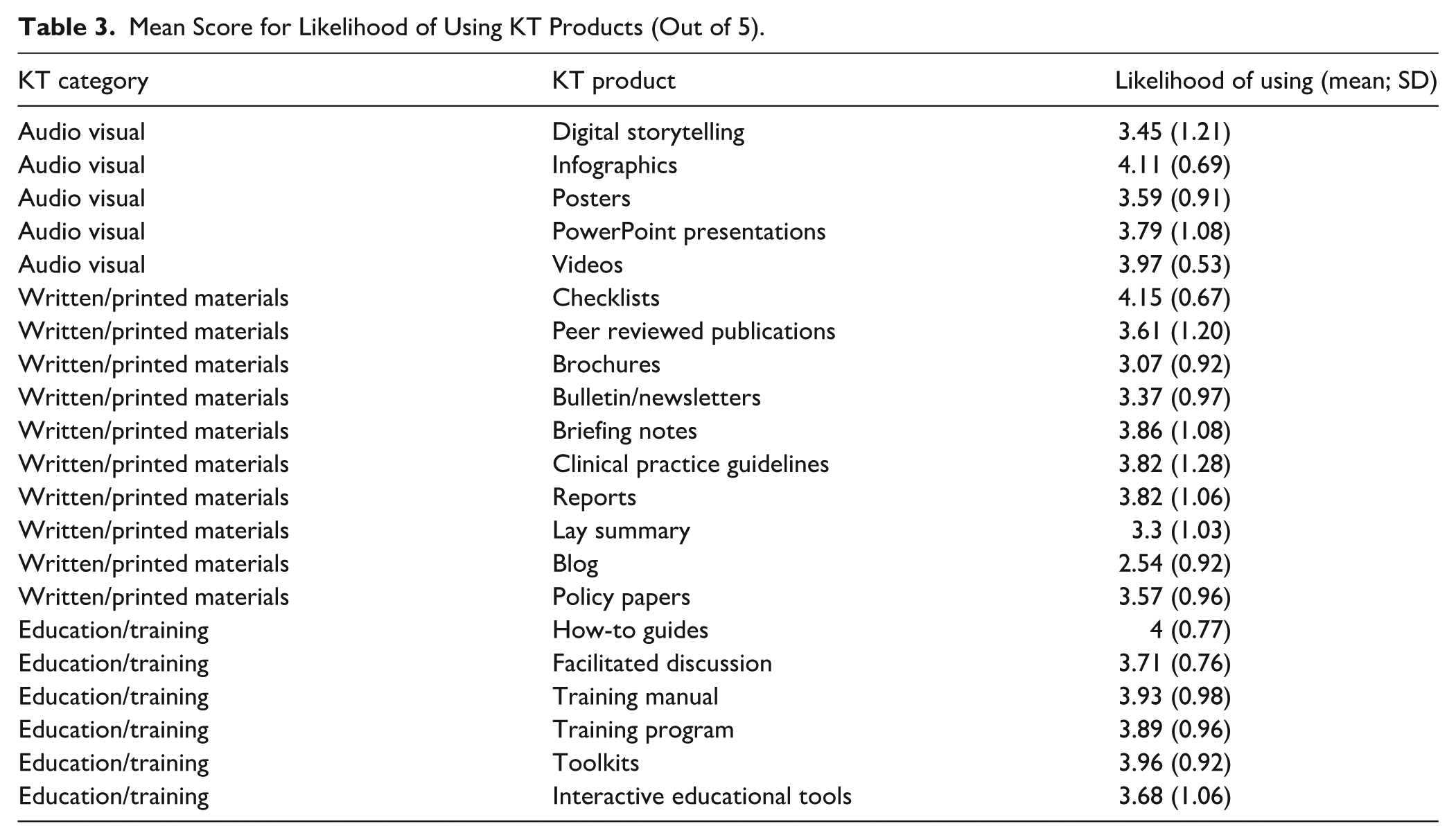
Thirty-three Virtual Health department members responded to the survey (>95% of the Virtual Health department). KT products most likely to be used include checklists (mean = 4.15 out of 5, SD = 0.67), infographics (mean = 4.11, SD = 0.69), how-to guides (mean = 4, SD = 0.77), videos (mean = 3.97, SD = 0.53), and toolkits (mean = 3.96, SD = 0.92). KT products least likely to be used include blogs (mean = 2.54, SD = 0.92), brochures (mean = 3.07, SD = 0.92), lay summaries (mean = 3.3, SD = 1.03), and newsletters or bulletins (mean = 3.37, SD = 0.97) (Table 3).
Mean Score for Likelihood of Using KT Products (Out of 5).
When asked where they would prefer to receive KT products, participants most often chose Microsoft Teams (67% of respondents), online educational courses provided through FH (64%), online databases (48%), within team meetings (45%), and educational workshops (34%). The least preferred methods included Facebook, Twitter, and informal meetings and discussions (all of which were selected by zero respondents). For all responses, see Table 4.
Participant Preference for Certain Modes of Delivery for KT Products.

The open textbox for additional thoughts received 3 responses. Two suggested that KT products are challenging to find within the existing Microsoft Teams structures and recommended a central repository and meetings to discuss knowledge products once they have been completed.
Evaluation of Existing FH Knowledge Products
Across the eight knowledge products evaluated, an average of 38% of participants were not aware of the knowledge product, 20% were aware but had not read them, 25% read them, and 16% had actively used them. See Figure 2 for information on individual KT products.

Level of awareness for each KT product.
Regarding relevance, an average of 14% of participants found the knowledge products not at all relevant, 27% found them slightly relevant, 23% moderately relevant, and 27% highly relevant to their job. Among those who rated them at least “somewhat relevant,” an average of 24% of participants also reported having “used” the knowledge product. See Figures 3 and 4 for information on each KT product.

Perceived relevance of each KT product.

Percentage of participants who reporting using a KT product among those who rated the KT product at least “somewhat relevant.”
The most relevant KT products included patient engagement guidelines (KT type = how-to-guide, 64% of participants found moderately or highly relevant), Virtual Health Evaluation Toolkit (KT type = toolkit, 61% found moderately-highly relevant), and the Virtual Hospital Program Current State Assessment (KT type = report, 58% found moderately-highly relevant). KT products participants were least aware of include Immigrant, Refugee, and Indigenous review (primary KT type = report, 61% were unaware), the Virtual Hospital Program Evidence Synthesis (KT type = report, 48% were unaware), and the Virtual Hospital Program Current State Assessment (KT type = report, 42% were unaware).
Phase 3: Qualitative Interviews
Ten interviews were conducted with managers and directors from the Virtual Health department, offering insight into how knowledge products are shared, received, and used, as well as organizational conditions that shaped their uptake.
Theme 1:
KT Uptake Is Shaped by How Knowledge Products are Introduced, Framed, and Integrated
Participants emphasized that engagement with KT products depended less on the content itself and more on how products were introduced and embedded within team activities. Active dissemination formats, particularly facilitated discussions during meetings or team days were consistently described as enhancing awareness, relevance, and use.
For example, Remote Patient Monitoring (RPM) patient journey maps were among the most frequently used products, which participants attributed to their introduction through a facilitated, interactive session: We were all engaged and using those patient journey maps to inform recommendations and actions and next steps. It was a facilitated activity at one of our team days.
However, participants also highlighted accessibility challenges related to product design. One participant who identified as neurodivergent, described difficulty engaging with the visual layout: It’s very wordy, very busy, very overwhelming . . . I get lost in it.
Across products, participants described similar patterns. Patient Profiles were valued for strategic planning because they translated complex evidence into visually digestible formats: They really helped us determine which patient population [to focus on] . . . it helped inform that decision. It shows exactly which outcomes are impacted by each of these different virtual care services . . . this is really useful to see where we focus our efforts.
In contrast, products that lacked active dissemination or clear framing, such as the Immigrant, Refugee, and Indigenous review, were less frequently engaged with, even when participants recognized their intrinsic value: We’re not really partnered with any Indigenous clinical service areas . . . so I see why it’s not been a focus. There are great ideas in here. I don’t know that our team specifically would be able to action some of these things.
Together, these findings suggest that KT uptake is closely tied to dissemination format, usability, and alignment with existing project workflows, rather than product quality alone.
Theme 2:
Organizational Capacity Constraints Limit Engagement, Even When Products are Valued
Limited time, competing priorities, and tight timelines were pervasive barriers to engaging with KT products. Participants consistently described having to triage information based on immediate necessity rather than interest or perceived value: I would love to read all of these, to be quite honest, but because I only have so many hours in my day, I do tend to read out of necessity versus nice to have.
Timing also influenced usability. Several participants noted that evidence often arrived too late to inform decisions already underway: Sometimes the timing is a bit of an issue — not that the data isn’t useful, but it comes in later than we needed it. At that point, we’re too far down the path.
Awareness challenges compounded these constraints. Many participants described a lack of awareness of ongoing research and evaluation efforts that extended beyond not knowing where to find KT products, to not knowing that they existed at all: Until I did that survey [phase 2], I wasn’t aware that there was that published evaluation and learnings for the [Virtual Psychiatry Unit], but I have printed it out . . . I think it could be really useful.
Even when participants were aware that a product existed, retrieving it was often difficult due to fragmented storage locations and inconsistent naming conventions: If I know something exists and it’s related to my work, then I just search on Teams and try whatever I think you might have saved it as. . .
Participants expressed concern that valuable research outputs were not consistently reaching those best positioned to act on them: I worry sometimes a lot of this good information doesn’t get seen by the right people.
Rather than reflecting disinterest, these accounts conveyed frustration and a sense of missed opportunity: It almost causes me dismay, like — ‘Oh my God, there’s all this potential, and these are the things the rest of the world is doing, and we could do this.’
Participants also identified challenges related to the KT dissemination strategy itself. Notification fatigue, disorganized communication channels, and broken or buried links were described as practical barriers to engagement: People are getting unread message fatigue. I’ll click on something and mean to come back to it, but then it’s buried in the feed and I forget.
While meetings were viewed as an effective venue for sharing KT products, participants noted that reliance on synchronous dissemination could unintentionally exclude staff who were unable to attend or who joined the organization later: Some of these were presented in a meeting, but if you missed it — or were hired after — then it becomes something that just comes up offhand in a conversation.
These findings highlight that KT uptake is constrained by organizational conditions that limit attention and cognitive bandwidth, challenging assumptions that producing more or better KT products alone is sufficient. Additionally, current dissemination approaches may inadvertently contribute to information loss and uneven access, reinforcing capacity-related barriers to sustained KT engagement.
As 1 participant succinctly summarized the limits of KT efforts in the absence of organizational capacity and follow-through: These documents are only as good as the people who read and use them.
This statement encapsulates a broader recognition among participants that the impact of KT products is contingent not only on their quality, but on the time, attention, and structures required to engage with them.
Theme 3:
Actionability and Role Alignment Determine Perceived Relevance
Participants frequently assessed KT products based on whether their purpose, intended audience, and practical implications were clear. When relevance to one’s role or sphere of influence was ambiguous, engagement diminished.
Several participants questioned how particular research outputs were meant to inform their work: Sometimes I’ll hear about a project in research and evaluation and think, ‘Okay . . . but does this tie into anything I’m working on? Or is it something completely different?’
Others emphasized the need for clearer ownership and follow-through: Who was the audience for this document? Were there actions that were meant to come out of it? I see a lot of great ideas here, but I don’t know who’s responsible to move this forward.
Program specific products, such as the RPM evidence syntheses, were viewed as less relevant by participants outside the implementation portfolio: I’m assuming the RPM evidence synthesis and RPM patient journey maps are lower [in relevance] because those are program specific.
These findings underscore the importance of explicitly articulating intended use cases, audiences, and decision points during dissemination.
Theme 4:
KT Products Support Confidence, Advocacy, and Practice – When Conditions are Right
When KT products were timely, relevant, and well-integrated, participants described meaningful impacts on confidence, competence, and practice.
Research and evaluation projects . . . profoundly impacted my confidence in the service that we’re providing and also provided further ideas of how we could go even further and what the next steps would be to improve the service and expand the service.
Evidence was frequently used to support advocacy and “level-setting” discussions with leadership: My goal is that Leadership above and [beyond] our partners can see that it’s not just, you know, we’re making things up or saying this is why we should go in. There’s evidence to back that up. The evidence review . . . was significantly helpful level setting with our executive team.
Participants also described skill development through involvement in KT and evaluation processes: It was upskilling me almost in a certain sense, you know, to be better at critical thinking, defining criteria, and scanning the literature.
Beyond decision-making, KT products prompted reflection and improvement in work practices: It made an impact because I learned something new, and I got to participate and shape some of the concepts.
These impacts were not automatic but occurred when KT products aligned with participants’ roles, needs, and organizational context.
Cross-Cutting Enablers of Effective KT
Across themes, participants identified several enabling conditions: early engagement and co-development, tiered information that allowed users to engage at different depths, reinforcement over time, and visually digestible formats. These enablers functioned less as independent themes and more as mechanisms that moderated the barriers and impacts described above.
Engagement – Integrated KT Approach
Participants emphasized the value of being engaged early in the process and co-developing knowledge products. When participants felt their needs were heard, research was more meaningful and actionable.
Getting clarity on what the question is, who the end user is, and what they need — that really helps. For instance, the Virtual Hospital Service review was really useful because our team was actively trying to figure out the opportunities and challenges in that space. I think this was relevant because — number one — we asked for it.
Tiered Information and Tailored Communication
Participants appreciated knowledge products that offered layered content. Layered content refers to KT products designed with multiple levels of detail, such as executive summaries, visual overviews, and detailed appendices, allowing users to engage at a depth appropriate to their role and time constraints. The ability to repackage and reframe content for different audiences increased its usability and reach.
Having tiers of content is important. The detailed evidence scope might be appropriate for the project team, but not for senior leadership. Having layers of the onion helps me give people the right level of the story. I appreciated that most of the summary was at a high level — I got a broad understanding quickly. But I also went into the appendices and followed links to the original documents. That flexibility was helpful.
KT Strategy – Practicality and Reinforcement
Participants highlighted effective aspects of the KT strategy — especially those that created visibility and reinforced usage over time. Meetings and word of mouth were especially effective for generating awareness and buy-in. Reminders, particularly about tools like the Evaluation Toolkit, helped sustain engagement.
It was easy to use and well explained — when it’s appropriate to use, how to use it — and there were reminders along the way, like, ‘Hey, don’t forget this toolkit exists.’ That was really helpful.
Visual Appeal and Digestibility
Visually engaging formats and clear layouts increased the usability of KT products. Participants noted that documents with logical flow, concise language, and visuals – such as infographics or patient quotes – were easier to digest and more engaging. These formats helped users better connect with the content and consider its relevance in practice.
Making it more engaging, more concise, and more digestible — that way people can actually take it in and think about how they can use it. Generally, I find the infographic style or the visual style is much easier to digest.
Participant-Suggested Improvements to KT approaches
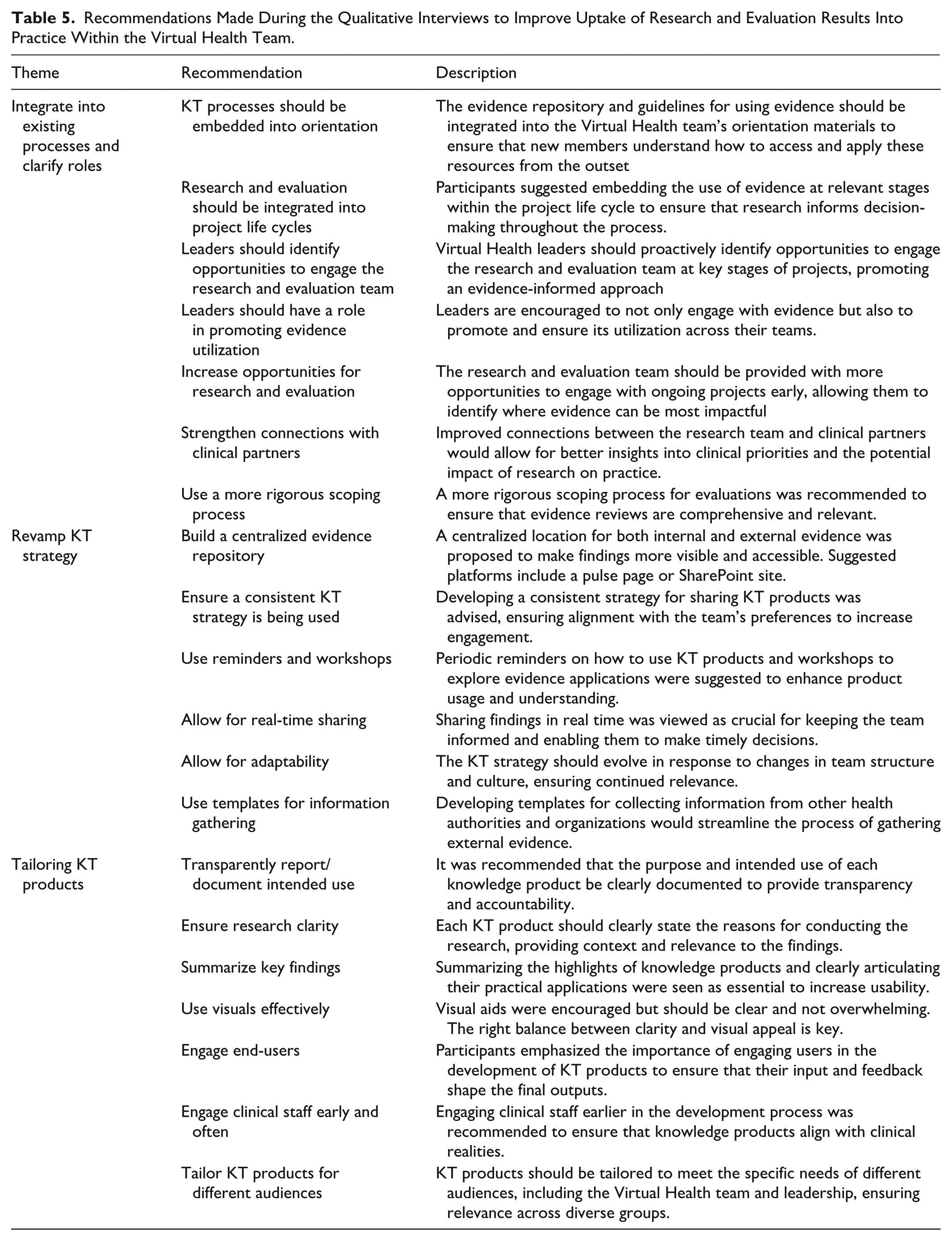
Participants offered practical suggestions to enhance KT effectiveness, including interactive sessions, short videos, searchable repositories, and clearer summaries (see Table 5 for a list and description of all recommendations). These suggestions reflect experiential insights into how KT products could better fit within everyday workflows rather than abstract preferences.
Recommendations Made During the Qualitative Interviews to Improve Uptake of Research and Evaluation Results Into Practice Within the Virtual Health Team.
Participants emphasized that effective knowledge products are brief, visually engaging, and connected to practical applications. They valued opportunities for discussion, follow-up sessions, and integration into regular workflows.
Create some sort of interactive session with those knowledge products, because then it puts us in front of our faces, makes us interact with it, and creates the space for us.
The need for enhanced accessibility and contextual relevance was also clear.
Sometimes people need a little hand-holding to understand — why was this done? What does it show? How might I use it?
Suggestions included leveraging quick videos, chat streams, summaries, and client stories to support real-time understanding and application.
Maybe you could do a little quick video — here’s what we created, here’s the outcome, this is how you might use it.
Participants also recommended improving visibility and navigation of KT materials by providing searchable, organized summaries.
Maybe there’s a table of contents, alphabetized, with hyperlinks to summaries or infographics — something quick to find and easy to digest.
Stronger collaboration between clinical, evaluation, and KT teams was suggested to ensure early identification of support needs, encourage co-creation, and support a shared understanding of what KT services can offer.
I think it needs to be built into our regular processes — not just an extra step at the end, but part of the whole workflow.
Discussion
This study evaluated the engagement, relevance, and use of KT products created for the Virtual Health department within a large health authority. Through a multi-phase process that combined a rapid review, survey, and qualitative interviews, this study reveals a nuanced understanding of the factors influencing the uptake and effectiveness of KT products and offers practical insights for improving the dissemination and impact of research and evaluation findings. Findings from both the survey and qualitative interviews suggest that suboptimal uptake reflects not only product design but also the characteristics of digitally mediated work environments, including asynchronous communication channels, competing digital information streams, and notification fatigue. Across phases limited awareness, fragmented dissemination channels, competing priorities, and constrained cognitive bandwidth emerged as central determinants of KT uptake, often overriding perceived relevance or quality of the products themselves. These findings suggest that KT effectiveness in virtual health environments may be shaped less by the intrinsic quality of knowledge products and more by the broader digital information ecosystem in which they are embedded.
Barriers to KT Product Use
Several barriers to the successful integration of KT products into practice was identified. A lack of awareness emerged as a significant issue, as many participants reported being unaware of the products. This finding aligns with existing literature, which underscores the importance of effective communication strategies in promoting the visibility of KT products. 71 Similarly, the lack of time to engage with products was frequently cited, with participants noting that competing priorities limited their capacity to explore or implement findings. Survey findings reinforce these qualitative insights: across all KT products, over one-third of respondents were unaware of their existence, and fewer than 1 in 5 reported active use. Together, these data suggest that awareness and access, not perceived relevance alone, represent critical bottlenecks in KT uptake.
These barriers must be viewed within the broader context of healthcare systems, which are often operating under significant resource and capacity constraints. Time and cognitive attention are finite, and it cannot be assumed that simply adding more KT resources or expecting end users to “make time” is a viable solution. Instead, these findings highlight the need for KT strategies that are efficient, embedded within existing workflows, and responsive to the realities of healthcare work. 72 Designing KT products that are streamlined, intuitive, and integrated into existing systems and routines is essential for ensuring their effectiveness in practice.18,73
Enablers of KT Product Use
KT products evaluated in this study were found to build participant confidence, support advocacy, and improve their work practices. This is consistent with previous research which demonstrates that engaging with research evidence can empower healthcare professionals by enhancing their knowledge and skills, thereby boosting their confidence in clinical decision-making. 74 Similarly, evidence-based KT products can support advocacy efforts by providing credible data that professionals can use to influence policy and practice changes. 1
The use of interactive and collaborative dissemination formats, such as workshops and team meetings, was particularly effective in increasing awareness and facilitating the application of KT products. Facilitated discussions helped contextualize information, encouraged dialog, and supported practical problem-solving among team members. These finding supports previous research on the value of participatory approaches in KT, which have been shown to foster greater ownership and application of evidence. 75
Reflections on Specific KT Products
Survey results indicated a preference for practical and visually appealing KT products such as checklists, infographics, how-to guides, videos, and toolkits. Participants preferred receiving KT products through existing digital platforms such as Microsoft Teams, online educational courses, and educational workshops. These findings reinforce the importance of embedding KT efforts within established digital and organizational infrastructures to support sustained engagement. 76 Importantly, the preference for receiving KT products through digital platforms such as Microsoft Teams does not necessarily translate into ease of access. Qualitative findings illustrate how fragmented storage locations, inconsistent naming conventions, notification fatigue, and reliance on synchronous dissemination can undermine visibility and retrieval. This helps explain why, despite strong stated preferences for digital delivery in the survey, awareness and use of KT products remained low across several highly relevant resources.
The survey and qualitative interviews suggest that the perceived relevance of KT products is tied to their applicability and the extent to which they address immediate operational needs of the Virtual Health department. Products like how-to guides and toolkits may be highly valued because they provide actionable steps and resources that can be applied in practice 52 whereas reports are often lengthy and detailed, requiring significant time and effort to read. Despite being reported among the most relevant KT products, the Virtual Hospital Program Current State Assessment was also among the products the Virtual Health team was least aware of. This paradox highlights a critical issue in KT efforts: even highly relevant products may fail to achieve impact if dissemination strategies are insufficient or poorly aligned with how staff access information.
These findings also point to a broader issue of accessibility in KT design. While accessibility is often framed primarily around patient-facing materials, this study highlights the need to extend universal design principles to internal KT products intended for healthcare workers. Ensuring that KT products are easy to navigate, visually clear, concise, and compatible with varied staff positions and workflows may enhance their usability and uptake across diverse roles and professional groups.
Implications for Future KT Product Development
Our findings suggest several implications for future KT product development and dissemination. Strategic and intentional dissemination approaches are required to address barriers related to awareness and time constraints. Tailored dissemination strategies that embed KT products within existing workflows, digital platforms, and routine team activities are more likely to enhance uptake and perceived relevance. Simplifying content, using visual design principles, and ensuring products are concise and action-oriented may further improve accessibility and impact. In keeping with participant recommendations, we translated these findings into a concise KT product summarizing cross-cutting enablers and practical improvements, modeling an evidence-informed approach to KT design (see Figure 5 for exemplar KT product and Supplemental Appendix for a checklist on KT development).

Exemplar KT Product Based on recommendations.
Involving end users early in the conceptualization and iterative development of KT products may also enhance alignment with real-world needs and preferences. Co-design approaches can help ensure that KT products are not only evidence-informed, but also practical, usable, and responsive to organizational contexts. Ongoing evaluation and feedback mechanisms, such as periodic surveys, focus groups, or workshops, can support continuous refinement and ensure KT products remain relevant as organizational priorities and evidence evolve.
Findings also underscore the importance of explicitly articulating the intended audience, decision points, and expected actions associated with KT products. Both survey and interview data indicate that relevance is assessed not only by topic, but by alignment with one’s role and sphere of influence. KT products that lack clear ownership or follow-through risk being perceived as informational rather than actionable, limiting their integration into practice even when the evidence is valued.
While the findings are context-specific, many of the challenges identified such as information overload, capacity constraints, and digital dissemination fatigue are likely relevant across other healthcare settings, particularly those implementing virtual or hybrid models of care. As such, the insights generated may have broader applicability for organizations seeking to strengthen KT practices in similarly complex and resource-constrained environments.
Strengths and Limitations
A key strength of this study is its comprehensive multi-method design, combining a rapid review, survey data, and qualitative interviews. This approach enabled triangulation of findings and provided a rich understanding of KT product use from multiple perspectives. The high survey response rate further strengthens the reliability of the findings by reflecting a broad cross-section of the Virtual Health department.
Several limitations should be acknowledged. Findings are specific to the Virtual Health department within FH, which may limit generalizability. However, the identified barriers and enablers are likely shared across other healthcare contexts, particularly those undergoing digital transformation. Increasingly, healthcare organizations internationally are adopting virtual and hybrid models of care characterized by distributed teams, asynchronous communication platforms, and rapidly evolving digital infrastructures. These conditions create common challenges for KT, including information overload, fragmented communication channels, and competing demands on staff attention. As such, the findings may offer transferable insights for organizations seeking to embed KT within digitally mediated healthcare environments.
Consistent with rapid review methodology, screening and data extraction in Phase 1 were conducted by a single reviewer to balance rigor with timeliness, which may have introduced selection bias. In Phase 3, interviews were conducted by colleagues within the same department, which may have increased the risk of social desirability bias. To mitigate this, confidentiality was emphasized, critical feedback was encouraged, and interview findings were triangulated with anonymous survey data.
Because interviews in Phase 3 were conducted by colleagues within the same department, participants may have moderated their feedback due to social desirability or perceived professional relationships. Although confidentiality was emphasized and triangulation with anonymous survey data was used to mitigate this risk, the potential influence of interviewer positionality should be acknowledged.
Additionally, this study focused on proximal KT outcomes (awareness, relevance, and use) rather than downstream clinical or patient outcomes. While these proximal outcomes are essential precursors to practice change, future research should examine how KT product engagement translates into measurable impacts on clinical decision-making, service delivery, and patient outcomes.
Future Research Directions
Digital Knowledge Translation
The preference for using platforms like Microsoft Teams highlights the need for KT strategies to adapt to the increasingly digital nature of communication within healthcare organizations. Future research should explore how emerging technologies such as artificial intelligence, machine learning, and predictive analytics can enhance the accessibility, relevance, personalization, and timeliness of KT products. Digital tools may also provide novel opportunities for tracking the engagement and impact of KT products over time, enabling real-time refinement based on usage patterns and feedback.
While digital platforms are becoming more common, disparities in access to technology and varying levels of digital literacy among healthcare workers could present barriers to effective KT. Future research should explore strategies to make KT efforts more inclusive, ensuring that all healthcare workers, regardless of their digital skills or access to technology, can engage with and apply KT products effectively. This might include creating parallel low-tech KT products or providing ongoing training and support to build digital capacity within healthcare teams.
Sustainability and Long-Term Impact
Further research should explore the specific characteristics of KT products that facilitate their adoption across different clinical settings. Longitudinal studies could be conducted to understand the sustained impact of KT interventions on clinical decision-making and patient outcomes over time. While short-term gains in KT product use and engagement are important, the ultimate goal is to foster long-term changes in practice and organizational culture. A key research question for future studies is how KT interventions can be sustained over time, especially in the face of changing organizational priorities, staff turnover, and evolving clinical guidelines. Research should focus on identifying factors that contribute to the sustainability of KT efforts and how these can be embedded within organizational structures for long-term success.
Conclusion
This study provides a comprehensive examination of KT strategies within the FH Virtual Health department, highlighting both barriers and enablers to effective knowledge dissemination and use. Through a multi-phase approach involving a rapid review, a survey, and qualitative interviews, the study identified key preferences for KT products and modes of delivery, as well as critical factors influencing their adoption and impact. Capacity constraints, content overload, and lack of clinical input pose significant challenges. However, the study also underscores the potential for KT products to improve confidence, support advocacy, and enhance work practices. By addressing identified barriers and building on successes, future KT efforts can further support the integration of evidence into practice, ultimately improving patient care and organizational outcomes. Embedding KT activities into organizational workflows and enhancing the accessibility of KT products are essential steps forward. Ongoing engagement with end-users and the development of tailored, user-friendly KT products will be crucial in enhancing the uptake of research evidence.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319261445471 – Supplemental material for “These Documents Are Only as Good as the People Who Read and Use Them”: A Phased Evaluation of Knowledge Translation Practices in Virtual Health
Supplemental material, sj-docx-1-jpc-10.1177_21501319261445471 for “These Documents Are Only as Good as the People Who Read and Use Them”: A Phased Evaluation of Knowledge Translation Practices in Virtual Health by Megan MacPherson, Maria Montenegro and Mahabhir Kandola in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We would like to acknowledge that this work was conducted within the Fraser Health Authority. Fraser Health provides care on the unceded and traditional homelands of the Coast Salish and Nlaka’pamux Nations.
Ethical Considerations
All methods were carried out in accordance with relevant guidelines and regulations, along with an ethical approval statement and informed consent to participate according to the Declaration of Helsinki. The study was approved by the Ethics Research Committee of the Fraser Health Authority.
Consent to Participate
Informed and written consent was obtained from all individual participants included in the study. Participation was on a voluntary basis.
Consent for Publication
Participants in this research gave consent for the information they provided to be published in an anonymized format.
Author Contributions
MM1 and MM2 were responsible for study conceptualization. MM1 was responsible for the completion of phase 1. MM1 and MM2 were responsible for creating the survey, recruiting participants, and data analyses and interpretation in phase 2. MM2 and MK were responsible for creating interview guides and conducting interviews in phase 3. MM1 and MM2 were responsible for data analysis for phase 3. MM1 drafted this manuscript, and all authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Research Foundation of Innovative Medicines Canada Team Grant in Virtual Care.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author* on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.