
Abstract
Introduction:
Produce prescription programs (PPRs) are evidence-based strategies increasingly used to address food insecurity and prevent or manage diet-related chronic disease. Fresh to Flourish is a PPR implemented in 2 Colorado-based practices within the CommonSpirit Health system. This qualitative study explored: (1) how implementing Fresh to Flourish impacts provider-patient relationships, and (2) the fulfillment experience of PPR referral providers.
Methods:
Virtual 1:1 key informant interviews were conducted with healthcare providers. Interviews were recorded, transcribed verbatim, and independently double coded using a deductive codebook aligned with the 7 constructs of the Theoretical Framework of Acceptability of Healthcare Interventions.
Results:
Ten interviews were completed across 1 rural and 1 suburban Colorado practices. Four themes emerged: (1) providers perceived Fresh to Flourish as valuable to patient care; (2) discussions about financial strain and food insecurity prompted referrals; (3) providers appreciated the simple referral process and on-site program staff; and (4) providers shared insights about integrating Fresh to Flourish into clinical workflow and systems.
Conclusions:
As aligned with the supporting theory, providers demonstrated high affective attitude, ethical alignment, and perceived effectiveness of Fresh to Flourish, with minimal burden and strong self-efficacy. Overall, providers viewed Fresh to Flourish as impactful while emphasizing the need to expand access and reduce barriers.
Keywords
Introduction
Food insecurity remains a prevalent and persistent challenge in the United States, with meaningful implications for chronic disease prevention and management. In Colorado, more than 1 in 10 households experienced food insecurity in 2023, a pattern that mirrors national trends and has remained stable into 2025.1-3 Food insecurity is shaped by intersecting structural and individual factors, including transportation barriers, competing financial demands, mental health challenges, and limited time for food preparation.4-7 These constraints contribute to poor diet quality and worsen outcomes for diet-related chronic diseases commonly managed in primary care. Food is Medicine (FIM) interventions are increasingly integrated into healthcare settings as strategies to address food insecurity and improve health outcomes. 8 Produce prescription programs (PPRs), a key FIM approach, provide patients with vouchers or incentives to purchase fruits and vegetables, often alongside nutrition education and clinical referral pathways. Evaluations of PPRs demonstrate associations with improved fruit and vegetable intake, enhanced food security, and favorable cardiometabolic outcomes, including improvements in glycemic control.9-11 The Gus Schumacher Nutrition Incentive Program (GusNIP), the largest federal funder of PPRs, has supported rapid expansion of these programs nationwide, signaling growing adoption within healthcare systems. 12
Healthcare providers play a critical role in PPR implementation by identifying eligible patients, initiating referrals, and introducing conversations about food access within brief clinical encounters. 13 However, primary care providers face substantial constraints, including limited visit time, competing clinical priorities, administrative burden, and high rates of burnout.14-18 Prior research indicates that while providers value PPRs as tangible resources for patients experiencing food insecurity, implementation challenges—such as workflow integration, staffing capacity, and training needs—may influence uptake and sustainability.19-21 Despite this, existing literature has largely focused on patient-level outcomes, with less attention to how PPRs affect provider-patient relationships and providers’ sense of fulfillment in delivering care.
To address this gap, this qualitative study examined Fresh to Flourish, a produce prescription program implemented in 2 Colorado-based primary care practices within the CommonSpirit Health system. The study aimed to explore: (1) how implementing Fresh to Flourish influences provider-patient relationships, and (2) the fulfillment experience of healthcare providers who refer patients to the program.
Methods
Theoretical Framework
This study applied the Theoretical Framework of Acceptability of Healthcare Interventions to examine how providers perceive the appropriateness of Fresh to Flourish across 7 constructs, including affective attitude, burden, ethicality, perceived effectiveness, and self-efficacy. 20
Intervention and Setting
Fresh to Flourish started in 2022, and is a PPR offered by CommonSpirit Health.22,23 The program operates out of 2 primary care practices in Colorado associated with Mercy Hospital (Southwest Colorado; population 19 811 people; Practice 2) and St. Mary Corwin Hospital in (Southeast Colorado; population 111 166 people; Practice 1).22,23 Eligibility criteria for Fresh to Flourish include (1) being a Medicaid member, receiving Supplemental Nutrition Assistance Program benefits, or being food insecure (Practice 2 only); and (2) having a diagnosed chronic condition or risk for developing 1 (including but not limited to diabetes, cardiovascular disease, lung disease, and behavioral health conditions, BMI >25 kg/m2). 22 The vouchers can be redeemed at local grocery stores, farmers markets, and farm stands. Fresh to Flourish staff enroll patients through the proactive screening and individual outreach process during regular visits, or by referral directly from providers. 22
Study Design
To expand on Fresh to Flourish’s evaluation, the leadership team partnered with researchers at Colorado State University to conduct individual interviews with health care providers (eg, key informants) at the 2 Fresh to Flourish implementation practices.
Provider Recruitment
Purposive sampling was used to ensure a representative sample of the diversity of healthcare providers were recruited at each practice (eg, MD and NP). 24 Participant eligibility criteria included: (1) employed at 1 of 2 practices participating in this study and (2) could refer patients to Fresh to Flourish. At each practice, the Fresh to Flourish implementation team recruited referring health care providers to participate in a virtual 30-min interview. Recruitment emails were sent between June 30 to July 25, 2025. Interested healthcare provider participants were asked to designate their availability on a shared Google document, and the research team scheduled the interview. This study was deemed exempt by both the CommonSpirit Health Institutional Review Board (#2030781-2) and Colorado State University Institutional Review Board (#6919).
Data Collection
Interviews followed a semi-structured interview guide (Table 1) which was based on key concepts from the Theoretical Framework of Acceptability of Healthcare Interventions. 20 All interviews were conducted via Zoom or a recorded phone-based application by a doctoral student trained in qualitative research methods (S.P.). All interviews were audio-recorded and professionally transcribed verbatim by Rev.com. 25
Semi-structured Interview Guide for Fresh to Flourish Referral Providers.

Data Analysis
All transcripts were uploaded into Atlas.ti (version 25) to digitalize and support transparent, rigorous coding.26,27 Using a deductive coding approach (ie, pre-determined codes based on literature, theory), a codebook was developed using the Theoretical Framework of Acceptability of Healthcare Interventions. 20 One research team member (S.P.) independently coded all transcripts in Atlas.ti followed by a second team member (S.S.) who independently coded 20% of the transcripts using the same codebook. 28 The 2 researchers met to create categories from the codes. The codes were then grouped into categories based on the theoretical framework (eg, affective attitude, ethicality, and perceived effectiveness were grouped together). The lead researcher then collapsed categories to construct salient themes. Representative quotations were selected to exemplify each theme. 28 The themes and representational quotations were shared with the Fresh to Flourish leadership team to triangulate the preliminary findings. 29
Results
A total of n = 64 recruitment emails were sent to health care providers and 10 Fresh to Flourish referral providers (n = 4 at practice 1; n = 6 at practice 2) agreed to be interviewed. In total there are 38 providers at practice 1 and 34 (89%) are referring providers. There are 28 providers at practice 2 and 15 (54%) are referring providers. Mean interview duration was 17 min (range: 10-24 min). All of the participants were Fresh to Flourish referring providers and specific roles (Figure 1). Most (n = 9, 90%) of the providers provided care for an adult population, and 1 provider (n = 1, 10%) specifically mentioned working with a pediatric population. Practice 1 serves a greater proportion of patients who are uninsured or receive Medicaid (61% of patients receive Medicaid) and includes a family medicine residency program, as compared to practice 2 (26% of patients receive Medicaid). Interviewees estimated the number of referrals per month. Overall, practice 1 interviewees referred more patients to Fresh to Flourish (range from 3 to 10 or more referrals per month) as compared to practice 2 (range from less than 1 to 3 referrals per month). For context on the Fresh to Flourish program, as of August 31, 2025, Fresh to Flourish provided 341 patients (n = 201 at Practice 2; n = 140 at Practice 1) with vouchers to purchase fresh produce (up to $350 in value) over a 6 months timeframe. 22
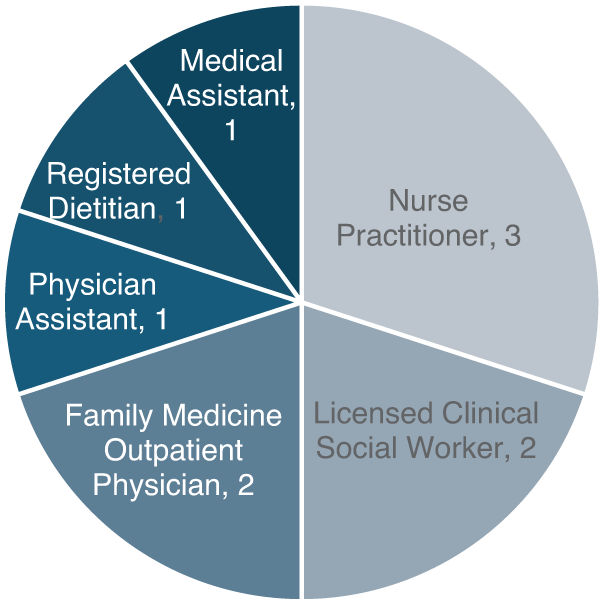
Interviewed Fresh to Flourish referring providers roles.
Four key themes were constructed across the interviews. Overall, there were minor differences between the themes between the 2 practices. First, providers found value in Fresh to Flourish when providing care to their patients. Second, patient conversations about financial and food insecurity are drivers for patient referral to Fresh to Flourish. Third, providers appreciated the simple referral process and on-site Fresh to Flourish staff members. Fourth, providers shared their goals for integrating Fresh to Flourish into clinical workflow and systems.
“I really like to think about Maslow’s hierarchies of needs. So if you don’t have your basic needs getting met, it’s really hard to get to the top of the pyramid, which is the self-actualization piece, (. . .) So making sure people have their base, the foundation of having access to food, housing, shelter, all of those things is important before you can start to do some of that [other work].” [CS2]
Another participant shared high affective attitude and that Fresh to Flourish made them feel fulfilled and helpful: “I think it is somewhat rewarding to know that you can have some options to help with whatever struggles are being identified, instead of just saying, “Oh, I’m sorry you can’t afford fruits and vegetables right now,” and then move on to the next thing.” [CS1]
“If people are financially constrained, I think that that’s the first thing that comes to my mind. And then after that, I would say people who just don’t eat enough, so their diet is deficient in vegetables and fruits is somebody else I would refer.” [CS6]
When describing the program to patients, providers shared that the program provides vouchers to purchase fresh fruits and vegetables. One participant shared that patients appreciate having the option to redeem their voucher at the local farmer’s market: “I do love and patients love that they can use them at the farmers’ market because that’s something fun that they can do as a family. And so their faces always kind of light up when they learn that they can be used at farmers’ markets.” [CS2]
“I send a message through Epic Chat to [Fresh to Flourish staff member] who runs the program here, and I connect the patient’s chart to that Epic Chat message.” [CS10]
Some participants suggested that having regular updates from the Fresh to Flourish staff would be helpful to know the number of people served, while others mentioned it did not affect their level of care. One participant appreciated learning how many patients were enrolled from the Fresh to Flourish team member: “[The Fresh to Flourish staff member] comes here and meets the patients. And she lets me know, “Oh, I spoke to this person,” or, “I enrolled this person.” And I like the collaboration.” [CS7]
“There’s a lot of patients that filter through my office that may not get cued up for referral, even though they meet criteria just because that day I saw them, we weren’t focused on that problem. Some kind of flag in their chart or something like that that would say, “Hey, this person has high social disparities or has had reported his problems affording healthy foods in the past,” that kind of thing would then just lead me to talk about that and probably generate more referrals.” [CS8]
Finally, participants expressed a goal of expanding Fresh to Flourish so that it would ultimately be available to all patients.
Discussion
As guided by the Theoretical Framework of Acceptability of Healthcare Interventions this qualitative study among the PPR Fresh to Flourish referral providers found that participants demonstrated high affective attitude, self-efficacy, ethical alignment, with minimal burden. Additionally, participants perceived Fresh to Flourish to be effective at improving patient health outcomes. Overall, participants emphasized how to integrate Fresh to Flourish into clinical workflow and systems, with the long-term goal to sustain the PPR.
In alignment with healthcare providers’ high affective attitude, ethical alignment, and perceived effectiveness, many participants shared that they wanted Fresh to Flourish to continue as a resource for patients. Having adequate resources for patient care increases healthcare provider motivation as well as their relationship with patients.30,31 Improving the relationship between patients and healthcare providers through solution-focused care and open communication, which can be facilitated through PPRs, can improve patients’ health outcomes.31-34 Overall, participants perceived this PPR to be worthwhile, despite having multiple responsibilities and limited time with each patient.
Although drivers of PPR referral and program goals were not primary research questions, these topics emerged organically during interviews as participants discussed organizational factors influencing referral practices. Providers described that Fresh to Flourish referrals were often initiated through conversations with patients about financial constraints and food insecurity. Given the limited time available during clinical encounters, participants noted that when these topics did not arise, opportunities for referrals may have been missed. In this context, some participants suggested that integrating food insecurity screening into the electronic medical record could serve as a reminder to initiate food-related conversations when a relevant referral option is available; however, these perspectives were offered specifically within the setting of an existing PPR and may not reflect provider preferences in the absence of actionable referral pathways. Prior studies similarly report growing adoption of food insecurity screening across healthcare settings, though implementation remains inconsistent.35-37 Importantly, ongoing debates in the literature highlight concerns about the potential burden on providers and patients when social needs are identified without clear mechanisms for response. 38 Taken together, these findings point to the importance of considering how social needs screening is implemented, particularly the alignment of screening practices with available resources, referral workflows, and clinical context, rather than assuming universal benefit across settings.
To enhance Fresh to Flourish sustainment, there are many considerations including increasing patient referral or need for the PPR, expanding funding, building partnerships, and enhancing evaluation. In this study, participants suggested developing a brief training about the eligibility criteria, goals, and how to discuss Fresh to Flourish with patients. Follow-through updates on the number of referrals had mixed feedback in this study, with some providers seeing benefit while others did not perceive it to affect care. Prioritizing training for healthcare providers is essential to the implementation of PPRs.39-41 To advance the evidence base and reach of PPRs, more work is needed to expand and diversify funding sources, conduct rigorous evaluation to create policy to support nuanced needs to sustain these programs, and build cross-sector partnerships.33,42,43
Strengths and Limitations
A key strength of this study is the inclusion of healthcare providers with direct experience referring to Fresh to Flourish, which generated rich, practice-based insights into implementation processes, perceived value, and opportunities for program improvement. However, despite efforts to recruit both referring and non-referring providers, participation was limited to those actively making referrals; therefore, perspectives from eligible providers who did not refer patients were not captured and warrant future study. The small sample size likely reflects competing clinical demands and variable awareness of the program. Finally, differences in patient populations across the 2 practices, particularly higher proportions of uninsured or Medicaid-insured patients at practice 1—may influence transferability of findings.
Conclusions
Overall, Fresh to Flourish may enhance healthcare provider fulfillment by offering a practical, clinic-embedded resource to address food insecurity within routine primary care. Providers perceived the program as effective in improving patients’ access to healthy foods while fitting within existing clinical workflows. Future research should examine barriers among non-referring providers and identify strategies to support broader adoption, including provider training, sustainable financing, and integration into primary care systems.
Footnotes
Ethical Considerations
This study was deemed exempt by both the CommonSpirit Health Institutional Review Board (#2030781-2) and Colorado State University Institutional Review Board (#6919).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the Gus Schumacher Nutrition Incentive Grant Program, project award no. 2021-70030-35797/project accession no. 1027395 and grant no. 2022-70423-38073/project accession no. 1029091, from the U.S. Department of Agriculture’s National Institute of Food and Agriculture, National Institutes of Health (K01DK128023; PI: Stotz), and CommonSpirit Health’s Mission and Ministry Fund.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The deidentified datasets generated during and/or analyzed during the current study are available from the corresponding author* on reasonable request.