
Abstract
Background:
Our study examined health care utilization outcomes among individuals participating in Pathways, a community hub model that employs a community-based workforce to deliver care coordination services, in Southwest Washington.
Methods:
Using community health record and Medicaid claims data between August 2018 and August 2022, we defined our treatment group as Medicaid beneficiaries enrolled in Pathways (N = 395), and our control group as Medicaid beneficiaries referred to any care coordination program (N = 198). We employed difference-in-differences analyses to compare the change over time in the proportion of individuals using care and the amount of health care used per member per year (PMPY).
Results:
Relative to the control group, the treatment group experienced a significant increase in connection to outpatient care, with a higher proportion accessing primary (9.6%, P = .073), specialty (12.8%, P = .033), and outpatient mental health (11.8%, P = .031) care after enrollment in Pathways. We also observed encouraging trends in acute care use.
Conclusions:
Participation in Pathways was associated with connection to outpatient health care and promising decreases in acute care use among Pathways participants. Our findings support the evidence base for Pathways as an effective model of care coordination for people with complex health and social needs.
Keywords
Introduction
Poor integration between health care and social services systems present immense challenges for patient populations, especially for people with complex health and social needs.1,2 System fragmentation not only creates barriers to accessing needed care,3,4 it also drives increased care utilization and costs due to unnecessary duplication in services, ineffective interventions, and uncoordinated care.1,3 Moreover, siloed systems of health care and social services contribute to poorer health outcomes and reduced patient satisfaction.2,3
Care coordination programs, which have been widely implemented across the United States, aim to reduce system fragmentation, better synchronize services, and address needs by connecting people with health care and social services via a referral system.1,3,5,6 Although definitions and models of care coordination vary, many programs rely on case management led by a designated person or team that helps patients navigate system interactions and manage their care needs. 7 An ample body of evidence has demonstrated that care coordination programs are an effective strategy for increasing access to needed interventions and services that lead to improvements in health and health care utilization, enhanced patient experiences and satisfaction, and reduction in health care costs.6-9
The Pathways program (Pathways) employs a community hub model approach to care coordination. The community hub model works to more closely knit community-based organizations with health systems. For Pathways, an independent nonprofit entity serves a backbone or hub organization coordinating a network of community-based organizations. In turn, the partnering community based organizations hire and train community health workers (CHWs), frontline public health workers who are either trusted members of their community and/or have a deep understanding of the community being served, 10 to provide case management support to populations with complex and intersecting needs.11,12 Within Pathways, CHWs serve a critical role, identifying client needs; coordinating care and referrals across physical health, behavioral health, and social services partners; and providing support for navigation across the currently fragmented systems.1,5,13
To-date, Pathways has been implemented in over 35 communities across the United States 14 Prior evaluations of Pathways have reported changes in health care utilization related outcomes such as decreased cost per medical event, reduced hospital and emergency department admissions, per member per month cost savings, and reduced prescription charges, as well as positive impacts on health and wellbeing including increased confidence navigating systems and accessing resources, improved birth outcomes, and improved chronic disease control.11,15-17 While most previous outcomes evaluations of the Pathways model have focused on the birthing population and the impact of the model on health outcomes relevant to that population,16,18 preliminary evidence suggests that Pathways can successfully engage and help mitigate risks for adults with complex health and social needs.5,19 This evaluation expands on previous work by evaluating the relationship between Pathways participation and health care utilization outcomes among a general adult population with high medical and social needs.
In 2019, Soutwest Washington Accountable Community of Health (SWACH) implemented the Pathways model as a part of its HealthConnect Hub, a centralized care coordination system made up of several programs that vary in intensity. Some programs were COVID-related efforts to promote vaccine access and enable isolation, while others were care coordination efforts that supported the management of chronic conditions or met the needs of high-risk individuals recently released from emergency medical services or inpatient care. SWACH serves 3 counties in southwest Washington: Clark, Klickitat, and Skamania counties which differ in terms of geography, demographics, and population size. SWACH partnered with 12 different community-based organizations, community health centers, and community action agencies across its service region that served as the Coordinated Care Agencies for Pathways. As Coordinated care agencies, each site hired, trained, and managed the CHWs who led Pathways, supporting participants with navigating systems to receive care. In this article we assess the relationship between Pathways participation and health care utilization outcomes for individuals with high levels of health and social needs in southwest Washington State.
Methods
Intervention
In HealthConnect Hub, the CHWs completed a needs assessment for each potential participant, then enrolled the participant in the care coordination program(s) that best addressed their needs. The Pathways program used a set of standardized “pathways” where each pathway represented a specific need (eg, housing) and had a measurable outcome (eg, obtained housing) that must be obtained for the pathway to be successfully closed (called “closed complete”). The CHW’s work with participants scaled to the level of need. A participant might engage in Pathways only for a few months or could stay in the program as long as a few years depending on their set of needs.
Individuals could enter the Pathways program through referrals from community organizations, medical organizations, or self-referral. While the original priority population for the program was individuals with complex medical needs (eg, co-occurring physical and behavioral health conditions) and social needs, all referred individuals were eligible to enroll into Pathways. A participant was considered enrolled once they had completed the needs assessment and the CHW marked them as enrolled in Pathways in the community health record (CHR).
Study Sample
Individuals were eligible for the study if they were aged 18 years or older, were identified in the HealthConnect Hub CHR system between February 2019 and August 2021 and had at least 6 months of Medicaid enrollment before and after their index date in the CHR data. The treatment group consisted of 395 individuals enrolled in Pathways; their index date was their date of enrollment in Pathways. The control group consisted of 198 individuals who had a status of referred for any HealthConnect Hub program (including Pathways) in the CHR but did not enroll in any program; their index date was their date of referral to the HealthConnect Hub program. At the time of the study, no other organizations in the region operated a Pathways program. Individuals were excluded from the study if they were determined ineligible for, or declined to enroll in, any HealthConnect Hub program.
Data Sources and Measures
CHR data and Medicaid claims data were the 2 data sources used for this study. CHR data was used to identify eligible participants, as well as characterize social needs and program participation among the treatment group. Medicaid enrollment and claims data were used to describe the sample in terms of demographics and health status, and to assess our key health care outcomes.
Health care outcomes were constructed using modified Healthcare Effectiveness Data and Information Set (HEDIS) metrics to divide utilization into several unique categories: primary care, specialty care, outpatient mental health visits, emergency department visits, inpatient stays, and dental care. Utilization outcomes were expressed as both the percent of individuals using care and as the average number of visits per member per year (PMPY).
Analysis
We described the demographic, health, and utilization outcomes for the sample, as well as social need among the treatment group, at baseline, defined as the 12 months preceding the index date. All regression models are linear difference-in-difference (DiD) analyses comparing the change in health care utilization outcomes over time (pre to post program) between the treatment and control groups with the interaction between time and treatment group as our primary statistic. DiD models assess the differences between the treatment and control groups while accounting for the differences that may naturally occur over time. Having access to healthcare data before and after the program, as well as samples who both did and did not receive services, made a DiD analysis ideal for this study. Parallel trends for all subgroups of healthcare utilization were met before conducting DiD analysis (Appendix A)
Our DiD models adjusted for age, race, sex, language, and medical complexity, and used generalized estimating equations (GEE) with an independent correlation structure for robust standard errors to account for patients being in the data more than once. A Poisson distribution was used to model the proportion of individuals using care and a negative binomial distribution was used to model the average amount of care used for each care type. All analysis was conducted in R 4.1.1. All study protocols were approved by the Washington State Institutional Review Board (Study #2021-014).
Results
Figure 1 shows the final sample for the analysis. Of the 2224 individuals identified in HealthConnect Hub CHR, 1167 (52.5%) matched to Medicaid data. Of those who matched to Medicaid data, 373 (32.0%) were excluded from the analysis due to being ineligible or declining to enroll in a HealthConnect Hub program. This resulted in 516 individuals enrolled in Pathways; of these, 395 (76.7%) had at least 6 months of Medicaid enrollment before and after their index date and therefore comprised the treatment group. Likewise, there were 278 individuals with a status of referred to any HealthConnect Hub program; 198 (71.2%) had at least 6 months of Medicaid enrollment before and after their index date and therefore comprised the control group.

Sample population.
Table 1 gives the demographics of the treatment and control groups. There were few differences between individuals in the treatment and controls groups. Individuals in the treatment group were more likely to speak a language other than English, while individuals in the control group were more likely to identify as female and Hispanic. With respect to health status, both groups had high rates of having at least 1 chronic condition, although this was higher in the treatment (76.4%) than the control group (63.3%).
Demographics of the Treatment (N = 395) and Control (N = 198) Groups.
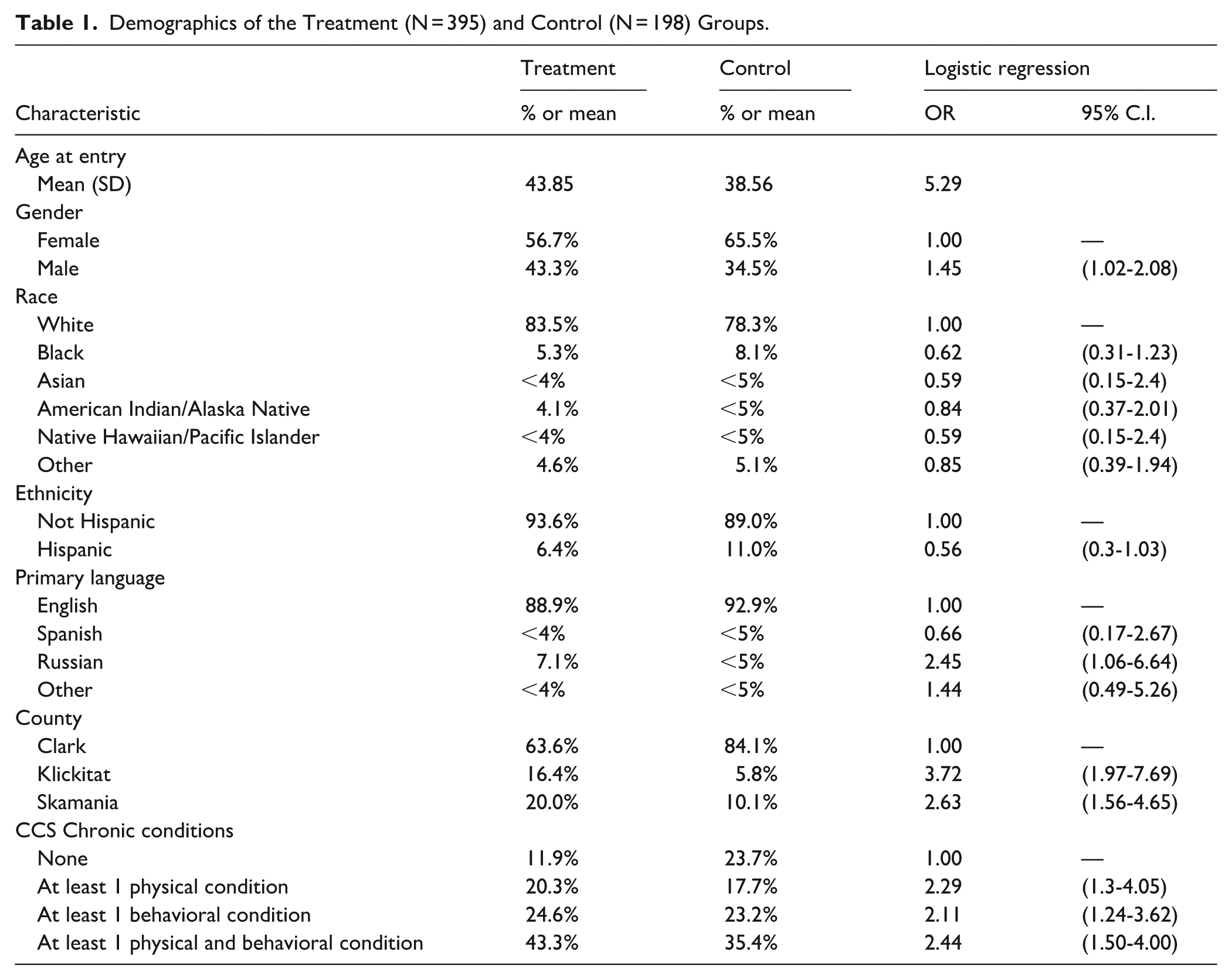
Table 2 also shows the top social needs identified by individuals in the treatment group. Individuals in the control group are not included because, by definition, they did not enroll in any HealthConnect Hub program and most did not complete a needs assessment. More than three quarters of individuals in the treatment group identified a housing need. Transportation, food, and clothing needs were also reported by more than half of the individuals in the treatment group.
Identified Social Needs of the Treatment (N = 395) Group.

Table 3 gives the proportion of individuals in each group who had each type of visit. Over 90% in each group had at least one interaction with any type of health care provider in the baseline and post periods. Among the treatment group, the proportion of individuals accessing primary care, specialty care, and outpatient mental health care increased after enrollment in the Pathways program; by contrast, the proportion of individuals accessing each type of outpatient care decreased in the control group, resulting in significant findings for the DiD analyses (primary care DiD = 9.6%, P = .079; specialty care DiD = 12.8%, P = .033; outpatient mental health care DiD = 11.8%, P = .031). The DiD analyses did not show any significant results for the proportion of individuals using emergency department, inpatient, or dental care.
Change in Proportions of Those Utilizing Health Care Among the Treatment (N = 395) and Control (N = 198) Groups.
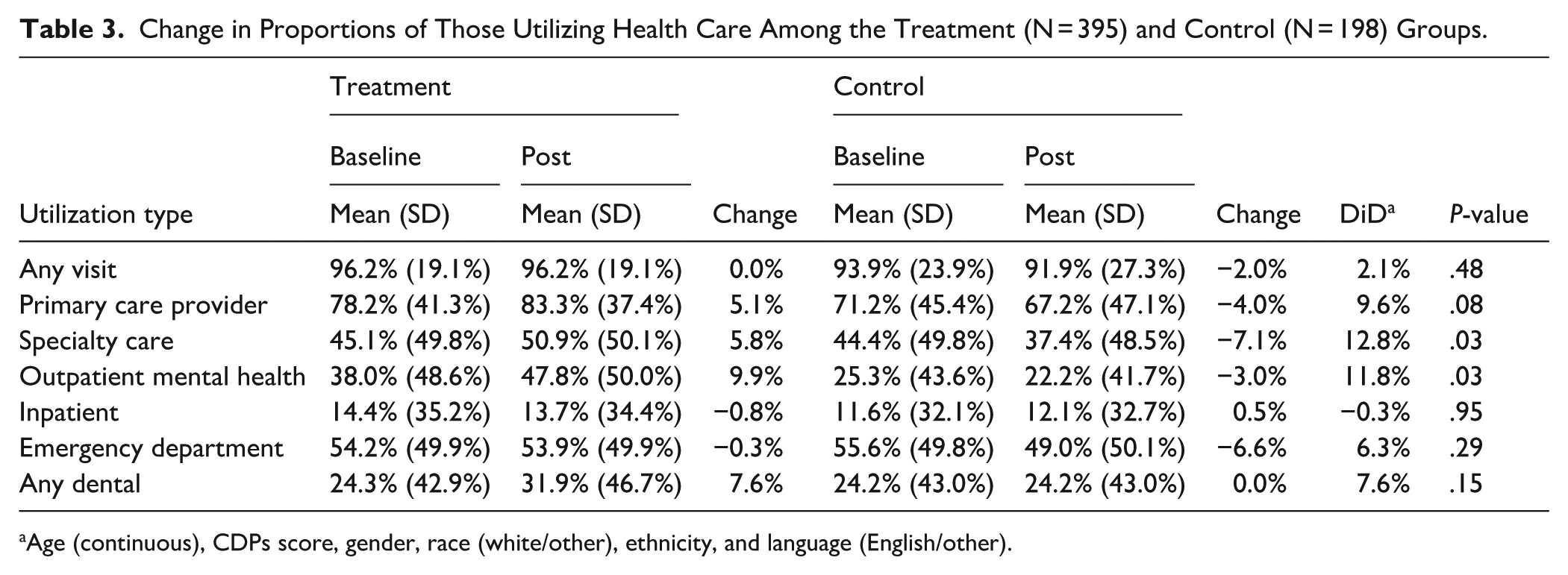
Age (continuous), CDPs score, gender, race (white/other), ethnicity, and language (English/other).
Table 4 provides changes in the average amount of each type of care individuals received among everyone in the treatment and control groups (PMPY). We did not observe any difference in the amount of any type of outpatient care, acute care, or dental care between the 2 groups.
Change in PMPY Utilization Rates Among All Individuals in the Treatment (N = 395) and Control (N = 198) Groups.

Age (continuous), CDPs score, gender, race (white/other), ethnicity, and language (English/other).
Discussion
In the United States, health care and social services systems are highly siloed, resulting in complex systems that are difficult for people with high levels of health and social needs to navigate.1-4 Pathways specifically addresses this challenge through community-based care coordination that supports program participants in navigating different health care and social services systems to receive the care they need. In 2019, SWACH implemented Pathways to promote whole-person health in their region. The findings from this evaluation provide evidence that community hub models of care coordination, like Pathways, can have significant associations with health care utilization outcomes for individuals with high health and social needs. By leveraging a control group consisting of individuals who were referred (ie, had a health or social care need) but did not receive services through HealthConnect Hub, the present study enables insights about the differences between addressing needs through the more coordinated model of Pathways versus “usual care” (ie, trying to access needed care in a fragmented system). Importantly, our evaluation demonstrated a positive association of the Pathways program on connection to outpatient health care including primary care, specialty care, and outpatient mental health care. Interestingly, while the proportion of individuals connecting to care increased, the average amount of care used PMPY stayed largely the same. Taken together, this suggests that Pathways may be most successful at helping an individual overcome the initial challenge of getting connected to care, but that once an individual is connected to care, there is no association with the amount of care they need.
Overall, individuals in the study sample had high levels of acute care use. More than 50% of those enrolled in Pathways had used the emergency department at least once in the year before enrollment and this proportion remaining relatively constant even after engaging with the program. Further, the amount of emergency department visits among those who used care was substantial, averaging over 4 visits per person at baseline. While we did not observe significant changes in the proportion or amount of acute care use, previous evaluations of similar interventions that leverage care coordination to address health and social needs have shown significant reductions in emergency department use and hospitalizations.20,21 Individuals use the emergency department for multiple reasons beyond emergent needs, having difficulty accessing primary care appointments, having greater trust in receiving quality care at an emergency department, or using the emergency department to address social needs.22,23 Because there are so many different reasons someone may use the emergency department, a 1 size fits all approach to diverting individuals to more appropriate outpatient care is unlikely to be successful. As such, understanding the unique drivers of acute care use in a given population is essential to better support individuals in using appropriate outpatient care.
Finally, the findings of this study highlight that care coordination programs like Pathways can successfully engage people with high levels of health and social needs. More than 3 quarters of the treatment group had at least 1 chronic physical or behavioral health condition and a similar proportion of participants reported a housing need at intake. Case studies of prior Pathways implementations similarly highlight successful engagement in of a broader adult population with high levels of health and social needs.5,19 Altogether, these data underscore the need for care coordination interventions like Pathways that seek to address health and social needs in tandem for a wide range of populations. Given the distinctions between the health and social sectors in terms of organizational structure, financing, workplace culture, and other factors,24,25 additional studies would benefit from examining the effect of these interventions on social service utilization. 26
Limitations
These findings should be interpreted in the context of the study’s limitations. First, participants were not randomly assigned to the treatment or control group, so it is possible that observed differences in utilization outcomes may be attributable to unobserved bias such as differences in social needs rather than the Pathways program. Moreover, the study population was limited to individuals enrolled in Medicaid and thus may not be generalizable to individuals with other types of insurance coverage or those who are uninsured. In addition, with a small sample size we observed variations in baseline utilization trends which make it difficult to confirm parallel trends. The study also lacks health outcome measures which represents a key aim of care coordination efforts like HealthConnect Hub. SWACH is located in counties with predominantly non-Hispanic White populations, and while the demographics of the study sample reflect the demographics of the southwest Washington population more broadly, the findings may not be generalizable to more racially and ethnically diverse areas.
Conclusion
This study demonstrates the association of Pathways on patterns of health care utilization. Participants had significantly increased access to outpatient care. The findings of this study help underscore the importance of care coordination efforts for improving access to care for individuals with high levels of health and social care needs.
Footnotes
Appendix A: Parallel Trends Graphs
Acknowledgements
The authors would like to acknowledge support and insight from the program staff at SWACH for their ongoing support of this evaluation work. Finally, we would like to thank the research staff who helped with this study including JB Rinaldi for their project support.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Washington State Institutional Review Board (IRB #2021-014).
Consent to Participate
Washington State Institutional Review Board (IRB #2021-014) waived the need for written informed consent.
Author Contributions
Conceptualization, SER, KGJ, and HCC; Data curation, KGJ; Formal analysis, KGJ; Funding acquisition, HCC; Supervision, SER and HCC; Writing – original draft, SER, RM, and HCC; Writing – review & editing, SER, RM, KGJ, and HCC. All authors have read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This evaluation work was funded by Southwest Washington Accountable Community of Health (SWACH). The funding body played no role in the design of the study, the collection or interpretation of data, or the writing of this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset used in this study was derived from community health records and health insurance claims that include individual-level identifiers and protected health information that are not publicly available due to human subjects protection requirements. We are unable to provide this dataset for public use.