
Abstract
Introduction:
Iron deficiency anemia (IDA) is one of the most common nutritional deficiencies in infants and can significantly impact cognitive and physical development if left untreated. This study aimed to estimate the prevalence of IDA among infants aged 6 to 18 months attending well-baby clinics at primary health care centers (PHCCs) in City, Saudi Arabia, and to assess associated demographic and clinical factors.
Methods:
A cross-sectional study was conducted from May 2022 to April 2023 across 3 PHCCs in the City. Infants aged 6 to 18 months presenting for routine vaccination were included through non-probability consecutive sampling. Data were extracted from the electronic health record system, including demographic details, laboratory values (Hgb, MCV, MCH, RDW, and serum ferritin), and management records. IDA was defined as low hemoglobin, low MCV, and high RDW, or low hemoglobin plus low ferritin. Statistical analyses were performed using RStudio with significance set at P < .05.
Results:
Of 1,827 infants included, 732 (40.1%) had laboratory screening data available. The median age was 10.0 months, and 50.5% were male. IDA was identified in 38 infants (5.2%; 95% CI: 3.8%-7.0%). Male infants had a significantly higher prevalence of IDA than females (7.6% vs 2.3%, P = .005). No significant differences in IDA prevalence were found across PHC centers (P = .173) or by age group (P = .537). Proper management documentation was available for 113 infants, with 61.1% receiving appropriate care.
Conclusion:
The study found a moderate prevalence of IDA among infants aged 6 to 18 months, with male infants at significantly higher risk. The findings highlight the need for improved routine screening and follow-up management, particularly among high-risk subgroups, to prevent long-term developmental complications associated with iron deficiency anemia.
Introduction
Iron deficiency (ID) is recognized as one of the most widespread nutritional deficiencies globally, particularly affecting vulnerable populations such as women and young children. It is estimated that over 2 billion people around the world suffer from this condition. 1 Iron Deficiency Anemia (IDA), which accounts for approximately half of all anemia cases, presents a major global public health concern. Its prevalence varies significantly, ranging from 1% to 18% in high-income countries and escalating to 30% to 51% in developing regions.2,3
In Saudi Arabia, the burden of IDA is substantial, with a recent systematic review of 20,929 participants showing a pooled prevalence of 33.7%. 4 Specifically, a study in northwestern Saudi Arabia found that 49% of infants visiting well-baby clinics were diagnosed with IDA. 5 In Makkah, a retrospective chart review of approximately 21 thousand patients showed an overall prevenance of IDA of 38.7%. 6 Another study in preschool children name primary health care centers found IDA to be the most common type of anemia affecting anemic patients. 7 Similarly, in Qatif, 27.1% of 1-year-old infants attending primary health care (PHC) facilities were found to have IDA. 8 Research from Makkah indicated that anemia among infants under 1 year of age was more prevalent among children of mothers with lower or intermediate education levels, and significantly higher in firstborn children. 9
Globally, a recent systematic review and meta-analysis by Gedfie et al in 2022 reported a pooled prevalence of IDA at 16.42%. 10 In the United States, IDA was found in 9% of infants aged 1 to 2 years and similarly in 9% to 10% of adolescents. 11 Meanwhile, in several Middle Eastern countries, the prevalence of IDA among children has been reported to exceed 70%.12-14 Moreover, there is consistent evidence linking IDA in early life with neurological and behavioral disturbances in children.15-17
To address these concerns, the American Academy of Pediatrics (AAP) recommends routine anemia screening beginning at 12 months of age. 18 This protocol involves evaluating hemoglobin levels and identifying risk factors such as low birth weight, low socioeconomic status, and exclusive breastfeeding beyond 4 months without iron supplementation. 19 While current guidelines focus on screening at 12 months and continuing through 1 to 3 years for at-risk groups, 20 this study specifically included infants aged 6 months younger and older than that age. This age group was selected to capture early and later-onset anemia associated with rapid growth velocity and exclusive breastfeeding, risk factors that are common in this population but may occur around the standard 12-month screening age.
Given the significance of early identification and prevention of IDA, this study aims to determine the prevalence and associated factors of Iron Deficiency Anemia among infants aged 6 to 18 months attending well-baby clinics in Primary Health Care Centers (PHCCs) in City, Saudi Arabia.
Methods
Study Design and Setting
This was a cross-sectional study conducted among infants who attended well-baby clinics in 3 Primary Health Care Centers (PHCCs) in City. These 3 centers ([CENTER A], [CENTER B], and [CENTER C]) were selected as they are the major affiliated centers, ensuring a representative sample of this specific healthcare system. The data collection period extended from May 2022 to April 2023.
Study Population and Sampling
The study targeted infants aged 6 to 18 months who presented to the well-baby clinics for scheduled vaccination visits. A non-probability consecutive sampling technique was employed, including all eligible infants during the study period. Consecutive sampling was employed to minimize selection bias. Standardized data extraction from EHR was used to reduce information bias. The study included a census of all 1,827 eligible infants presenting during the defined 1-year study period to maximize statistical power. Infants were excluded if they had an acute febrile illness at the time of visit or a known history of chronic diseases.
Data Collection
Data were retrospectively retrieved from the electronic health record (EHR) system. Demographic variables included the infant’s age at the time of visit and gender. Clinical and laboratory data collected included the PHCC attended, whether anemia screening was performed, hemoglobin (Hgb) level, mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), red cell distribution width (RDW), and serum ferritin levels. In addition, documentation of whether appropriate medical management was provided was recorded. Infants were classified as anemic if their hemoglobin level was less than 11 g/dL or if their serum ferritin level was below 10 µg/L.
Ethical Considerations
The study received ethical approval from the Institutional Review Board (IRB). All data were handled with strict adherence to confidentiality and privacy standards. Identifiable information was neither collected nor accessed, and all data were anonymized.
Statistical Analysis
Data analysis was performed using RStudio (R version 4.3.1). Categorical variables were expressed as frequencies and percentages, while continuous variables were reported as medians with interquartile ranges (IQR). The 1-sample proportion test was used to estimate the prevalence of iron deficiency anemia. Differences in IDA prevalence by age group, gender, and PHC center were assessed using Pearson’s Chi-squared test or Fisher’s exact test, as appropriate. Comparisons based on gender or PHC center were evaluated using Fisher’s exact test or Pearson’s Chi-squared test, depending on the distribution. A P-value of less than .05 was considered statistically significant. Complete case analysis was used for prevalence estimation; infants without laboratory screening results were excluded from the IDA prevalence calculation.
Results
Demographic Characteristics of Infants
The final dataset included 1,827 infants aged 6 to 18 months who attended well-baby clinics at 3 Primary Health Care Centers ([CENTER A], [CENTER B], and [CENTER C]) in City. More than half of the infants (58.9%) were registered at the [CENTER A] center. Males made up 50.5% of the overall sample. The median age (IQR) of the infants was 10.0 months (8.0-13.0). Screening for complete blood count (CBC) was requested for 732 infants (40.1% of the sample). Of the total sample, proper management documentation was available for 113 infants, with 61.1% receiving proper care (Table 1).
Demographic Characteristics of Infants Aged 6 to 18 months.

Management data were available for 113 infants in the overall sample and 111 in the lab subgroup; remaining records were missing.
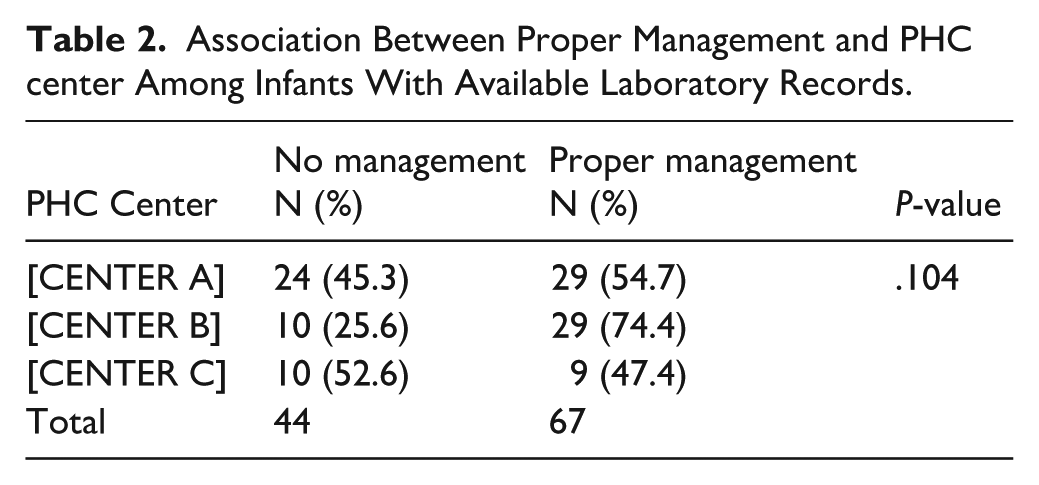
CBC screening requests were ordered for 732 infants, representing 40.06% of the sample (Figure 1). The subgroup with available CBC requests was subsequently analyzed in the following sections. More than half of that subgroup were males (53.5%), and 40.6% were from the [CENTER A] PHC institution. Proper management was provided for 60.4% of the subgroup with available lab records (Table 1). Further investigations revealed no significant difference in proper management practices across PHC centers among infants with available laboratory records (P = .104, Table 2).

A descriptive chart depicting the proportion of CBC requests and infants with iron deficiency anemia (IDA).
Association Between Proper Management and PHC center Among Infants With Available Laboratory Records.
Results of Laboratory Investigations
Among the 732 infants with available CBC records, low hemoglobin levels were found in 14.9%, low MCV in 13.7%, and high RDW in 32.5%. Serum ferritin levels were available for 685 infants, of whom 3.7% had low ferritin, and 63.8% had no ferritin ordered (Table 3).
Laboratory Results of Infants With CBC Data (N = 732).

Prevalence and Characteristics of Iron Deficiency Anemia (IDA)
Iron Deficiency Anemia (IDA) was defined as having low Hgb, low MCV, and high RDW or low Hgb plus low ferritin. Based on this definition, 38 infants (5.2%, 95% CI: 3.8%-7.0%) were diagnosed with IDA.
No significant difference was observed in IDA prevalence by age group (P = .537) or PHC center (P = .173). However, male infants had a significantly higher prevalence (7.6%) compared to females (2.3%, P = .005). The likelihood of receiving proper management did not significantly differ between infants with or without IDA (P = .535, Table 4).
Factors Associated With Iron-deficiency Anemia Diagnosis.

Discussion
The findings of this study revealed a 5.2% prevalence of iron deficiency anemia (IDA) among infants aged 6 to 18 months attending well-baby clinics in City. This rate is notably lower than figures reported elsewhere in Saudi Arabia, where prevalence has reached 49% in the northwestern region5,7 and 27.1% in Qatif. 8 Internationally, our results contrast with higher burdens observed in Jordan (21.5%), 21 Egypt (45.05%), 22 and the global pooled prevalence of 16.42%. 10 Instead, our findings align more closely with data from Qatar (7.8%) and the United States (9%).11,23
This comparatively low prevalence likely reflects the specific demographic served by institution, this population generally benefits from greater socioeconomic stability and access to iron-fortified nutrition compared to rural or mixed-income cohorts cited in previous studies. 24 However, a limitation of this study is that only 40.1% of eligible infants underwent screening. As physicians may have prioritized testing for infants with clinical indications, this could introduce selection bias, potentially overestimating the prevalence of IDA in this cohort compared to the general asymptomatic population.
Regarding risk factors, we observed no significant variation in IDA prevalence across different Primary Health Care Centers (PHCCs) or age groups, suggesting that geographical access and routine visit timing were not major determinants of risk in this population. In contrast, a significant gender disparity was evident, with male infants being more likely to develop IDA than females (7.6% vs 2.3%, P = .005). This finding is consistent with established literature15-17 and is biologically plausible; male infants typically exhibit a higher velocity of muscle mass accretion and blood volume expansion during the first year of life, resulting in greater iron utilization and a more rapid depletion of stores compared to females. While some studies have suggested that gender bias in feeding practices can contribute to nutritional disparities, the physiological demands of rapid male growth are considered the predominant cause of IDA in this specific age group.
A critical finding of this study is the gap in screening adherence. The American Academy of Pediatrics (AAP) recommends routine anemia screening starting at 12 months, particularly for infants with risk factors such as low socioeconomic status or exclusive breastfeeding without supplementation. 25 The fact that nearly 60% of infants in our cohort missed this recommended screening suggests that reliance on physician recall is insufficient. This highlights an urgent need for systemic interventions, such as the implementation of mandatory ‘hard-stop’ electronic alerts in the EHR system to prompt physicians to order a CBC during the 12-month vaccination visit. Furthermore, among those diagnosed with IDA, documentation of proper management was often incomplete, signaling a need to enhance clinical follow-up protocols to prevent long-term cognitive and developmental consequences.
Limitations
To our knowledge, this is the first study to specifically investigate IDA prevalence among infants aged 6 to 18 months in City primary care setting. However, several limitations must be considered when interpreting these results.
First, the study utilized a cross-sectional design, which captures data at a single point in time. While this allowed us to identify associations between risk factors (such as gender or age) and anemia, it precludes the establishment of causal relationships or the determination of temporal sequences between exposures and outcomes.
Second, the reliance on convenience sampling from 3 specific affiliated centers limits the external validity of our findings. As this population consists largely of Institution dependents, they may share specific socioeconomic or environmental characteristics that differ from the general population in City, thereby restricting the generalizability of the results to the broader community.
Finally, the retrospective nature of data collection introduced potential information biases. Data regarding dietary habits and breastfeeding history relied on physician documentation of parental accounts, which is subject to self-report and recall bias. Caregivers may have provided socially desirable responses or inaccurate recollections of feeding practices during clinic visits, and the lack of standardized detailed dietary records (eg, exact duration of exclusive breastfeeding or timing of solid introduction) prevented a more granular analysis of nutritional root causes. Future research should utilize prospective designs with broader sampling to overcome these inherent limitations.
Conclusion
In conclusion, this study highlights a moderate prevalence of iron deficiency anemia (IDA) at 5.2% among infants aged 6 to 18 months attending well-baby clinics in primary health care centers (PHCCs) in the city. While the overall prevalence is lower than in some previous local studies, the findings underscore critical concerns, particularly the significantly higher risk among male infants and the substantial gaps in ferritin testing and documentation of proper management. The absence of significant differences in IDA prevalence across age groups and PHC centers suggests that targeted interventions should prioritize risk-based rather than location-based approaches. These results emphasize the importance of strengthening routine screening protocols, ensuring timely follow-up, and improving adherence to clinical guidelines to prevent the adverse developmental impacts of undiagnosed and untreated IDA during early childhood. To do so, we strongly recommend implementing mandatory electronic alerts within HER systems to enforce universal screening adherence at the 12-month visit. Furthermore, establishing standardized clinical protocols for follow-up and providing targeted nutritional counseling for high-risk groups, particularly male infants, are essential to mitigate the developmental risks of iron deficiency anemia.
Footnotes
Author’s Note
Renad Nasser Balubaid is now affiliated to Department of Pediatrics Neurology, King Abdulaziz Medical City, Ministry of National Guard – Health Affairs, Jeddah, Saudi Arabia. Ibrahim Sallah Alibrahim is now affiliated to Department of Pediatrics, King Abdulaziz Medical City, Ministry of National Guard-Health Affairs, Jeddah, Saudi Arabi.
Ethical Considerations
The study received ethical approval from the Institutional Review Board (IRB) of King Abdullah International Medical Research Center (KAIMRC) [NRJ23J/158/06]. All data were handled with strict adherence to confidentiality and privacy standards.
Consent to Participate
Informed consent was waived by the Institutional Review Board due to the retrospective nature of the study using electronic medical records.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author* upon reasonable request.